You might also like
- INF1DDocument16 pagesINF1DRadu TuguiNo ratings yet
- 1000 MCQ Bank QuestionsDocument157 pages1000 MCQ Bank Questionsapi-2629165193% (59)
- Method Statement For Hot Tapping Rev 0Document9 pagesMethod Statement For Hot Tapping Rev 0Thomas100% (4)
- OSCE7Document89 pagesOSCE7mghiami67% (3)
- Level 7 Sentence Completion 3Document4 pagesLevel 7 Sentence Completion 3AnhĐứcNgôNo ratings yet
- CG A001 04 Radiographs Guideline PDFDocument10 pagesCG A001 04 Radiographs Guideline PDFmahmoudNo ratings yet
- 129 SAQsDocument13 pages129 SAQsSuryanarayana Murthy Kaivaram100% (3)
- The Dental Foundation Interview Guide: With Situational Judgement TestsFrom EverandThe Dental Foundation Interview Guide: With Situational Judgement TestsNo ratings yet
- Previous Adc QuesDocument11 pagesPrevious Adc QuesChander Kanta100% (3)
- Dentistry in The USADocument5 pagesDentistry in The USAEmeka V. Obi0% (1)
- Sample-Questions-Part 2-OSCE PDFDocument10 pagesSample-Questions-Part 2-OSCE PDFaram meyedy100% (1)
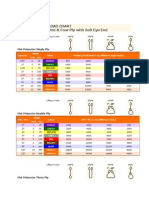
- Webbing Sling Load ChartDocument2 pagesWebbing Sling Load ChartThomas100% (1)
- Method Statement For Insulation Works and JacketingDocument8 pagesMethod Statement For Insulation Works and JacketingThomas100% (8)
- OSCE Study Plan - ADC PASS DR Mohamed Soliman GroupDocument3 pagesOSCE Study Plan - ADC PASS DR Mohamed Soliman GroupVishakha SabooNo ratings yet
- App - Written Examination DentistDocument8 pagesApp - Written Examination DentistNazNo ratings yet
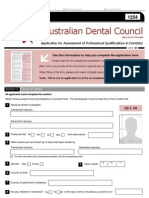
- ADC Assessment ApplicationDocument5 pagesADC Assessment ApplicationMuhammad ZainNo ratings yet
- Dental EmergenciesDocument23 pagesDental Emergenciesmw1974No ratings yet
- Adc March 2013 MCQ Part BDocument2 pagesAdc March 2013 MCQ Part BEsha Arora100% (2)
- SAQs VariousDocument16 pagesSAQs Variousapi-26291651100% (3)
- ORE Application FormDocument24 pagesORE Application FormNahelMoskvaNo ratings yet
- SOP GD and Dental Specialist FINALDocument20 pagesSOP GD and Dental Specialist FINALarpita7dr9693No ratings yet
- OSCEs For Dentistry PDFDocument3 pagesOSCEs For Dentistry PDFMohammed IssaNo ratings yet
- Bosch Pestel AnalysisDocument13 pagesBosch Pestel Analysisanett1996No ratings yet
- Overseas Registration Exam Application: Dentists Holding Dental Degrees From Outside The UK and EEADocument21 pagesOverseas Registration Exam Application: Dentists Holding Dental Degrees From Outside The UK and EEAPamungkas Dhani100% (2)
- Application For Initial Assessment - Dentist AS1 v10Document11 pagesApplication For Initial Assessment - Dentist AS1 v10Neha GurdasaniNo ratings yet
- ADC Written Exam Studying Strategy: 4 Months Study PlanDocument4 pagesADC Written Exam Studying Strategy: 4 Months Study PlanPepo Beloved100% (1)
- OSCE - Health PromotionDocument13 pagesOSCE - Health PromotionbabukanchaNo ratings yet
- The ADA Practical Guide to Patients with Medical ConditionsFrom EverandThe ADA Practical Guide to Patients with Medical ConditionsNo ratings yet
- ADC Practical Exam ListDocument8 pagesADC Practical Exam Listsreekanth vsNo ratings yet
- A.H.E.A.D: Mds / Adc / Nbde & Ndeb CoachingDocument12 pagesA.H.E.A.D: Mds / Adc / Nbde & Ndeb CoachingAhead Dental CoachingNo ratings yet
- GDC UkDentist Application MQ29UKDE253WDocument9 pagesGDC UkDentist Application MQ29UKDE253WMatthew QuigleyNo ratings yet
- Adc Books For Part 1Document2 pagesAdc Books For Part 1Rashmin Bhavsar43% (7)
- Sep 2014Document14 pagesSep 2014mandy100% (1)
- ADC Part-1 Course: Australian Dental CouncilDocument3 pagesADC Part-1 Course: Australian Dental CouncilAishwarya Menon100% (1)
- Me (Scenarios) (Printed)Document17 pagesMe (Scenarios) (Printed)Anup Lal RajbahakNo ratings yet
- ADC General Overview of The ADC ExamDocument11 pagesADC General Overview of The ADC Exammesssi269No ratings yet
- Preparation Strategy For ADC Written ExaDocument1 pagePreparation Strategy For ADC Written ExaVishnu Priya KarthikNo ratings yet
- What Is Root Canal Treatment?Document2 pagesWhat Is Root Canal Treatment?Vishakha SabooNo ratings yet
- Reference For Australia Dental Council ExaminationDocument6 pagesReference For Australia Dental Council ExaminationBeh Wee RenNo ratings yet
- Risk Assessment FormDocument3 pagesRisk Assessment FormThomas100% (1)
- March 2018 Free Not For SaleDocument33 pagesMarch 2018 Free Not For SaleOsama Mahmoud100% (1)
- A Step by Step Process of ORE Application 2Document12 pagesA Step by Step Process of ORE Application 2رغد شوكت تايه مسعودNo ratings yet
- Practical Examination Handbook May 2016Document32 pagesPractical Examination Handbook May 2016mandyNo ratings yet
- Ethics of DentistryDocument20 pagesEthics of DentistrytayabakhanNo ratings yet
- Written Examination Handbook Dentist 2018Document17 pagesWritten Examination Handbook Dentist 2018Anup Lal RajbahakNo ratings yet
- ADC Assessment ApplicationDocument5 pagesADC Assessment ApplicationDileep SharmaNo ratings yet
- Ethics in Nursing Research PDFDocument2 pagesEthics in Nursing Research PDFBrittney0% (1)
- The New Zealand Dental Registration Examinations PolicyDocument7 pagesThe New Zealand Dental Registration Examinations PolicyBilal AhmedNo ratings yet
- List of Tools and TacklesDocument3 pagesList of Tools and TacklesThomas80% (5)
- U S L I D: Nited Tates Icensure FOR Nternational EntistsDocument36 pagesU S L I D: Nited Tates Icensure FOR Nternational EntistsShirley Tatiane MartinsNo ratings yet
- Ore SampleDocument8 pagesOre SampleAyesha Awan100% (1)
- ADC Books ImportantDocument2 pagesADC Books ImportantJats_Fru_1741No ratings yet
- SEPT 2016 ADC ShanayaDocument38 pagesSEPT 2016 ADC ShanayaHeba MohamedNo ratings yet
- ORE DMGuidanceDocument19 pagesORE DMGuidanceHarry ArdiyantoNo ratings yet
- ORE Part 1 Schedule 30th & 31st JulyDocument6 pagesORE Part 1 Schedule 30th & 31st JulyLokesh Bakshi100% (1)
- NDEB Equivalency Process Required DocumentsDocument3 pagesNDEB Equivalency Process Required DocumentsSara FarisNo ratings yet
- 2 Part+1+Tutorial+DetailsadcDocument4 pages2 Part+1+Tutorial+DetailsadcAnup Lal RajbahakNo ratings yet
- OTC COURSES 2020 Information Booklet PDFDocument38 pagesOTC COURSES 2020 Information Booklet PDFMuhammad SajidNo ratings yet
- Clinical Schedule For Australian Dental Council Part 2 Exam CoachingDocument6 pagesClinical Schedule For Australian Dental Council Part 2 Exam CoachingdrrushikNo ratings yet
- ADC Certification of Document GuidelinesDocument2 pagesADC Certification of Document GuidelinesInventor SolidworksNo ratings yet
- MFDS Part1 DetailsDocument2 pagesMFDS Part1 DetailskaizalNo ratings yet
- Dental Foundation Training Portfolio User GuideDocument56 pagesDental Foundation Training Portfolio User GuideEdgar PalmaNo ratings yet
- Registering As A Dentist With The General Dental Council (Overseas Qualified)Document18 pagesRegistering As A Dentist With The General Dental Council (Overseas Qualified)zahra seraj0% (1)
- 2019 AFK Protocol - Revised 12102018 PDFDocument10 pages2019 AFK Protocol - Revised 12102018 PDFsNo ratings yet
- NATIONAL DENTAL BOARDS (NDB) / PART I: Passbooks Study GuideFrom EverandNATIONAL DENTAL BOARDS (NDB) / PART I: Passbooks Study GuideRating: 1 out of 5 stars1/5 (1)
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideFrom EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideNo ratings yet
- Atmosphere Management: O Consumption (CFM) CO Production (CFM) Activity SourceDocument16 pagesAtmosphere Management: O Consumption (CFM) CO Production (CFM) Activity SourceThomasNo ratings yet
- Atmosphere Management: O Consumption (CFM) CO Production (CFM) Activity SourceDocument16 pagesAtmosphere Management: O Consumption (CFM) CO Production (CFM) Activity SourceThomasNo ratings yet
- Guidelineforgasturbineinletairfiltrationsystems 1Document116 pagesGuidelineforgasturbineinletairfiltrationsystems 1ThomasNo ratings yet
- Risk Assessment - ScaffoldingDocument4 pagesRisk Assessment - ScaffoldingThomasNo ratings yet
- Endo Problems SolvedDocument5 pagesEndo Problems SolvedThomas100% (1)
- MCQ ExamDocument9 pagesMCQ ExamAnup Lal RajbahakNo ratings yet
- HCG LevelsDocument1 pageHCG LevelsThomasNo ratings yet
- Project Design PNP FoodDocument3 pagesProject Design PNP FoodAllen Lucre ReondangaNo ratings yet
- Facts: LBP V CA, G.R. 221636Document7 pagesFacts: LBP V CA, G.R. 221636Ian KeithNo ratings yet
- Flyer BFD Englisch BarrierefreiDocument2 pagesFlyer BFD Englisch Barrierefreiluizlucena3No ratings yet
- Position Paper GuidelinesDocument4 pagesPosition Paper GuidelinesAkash Deep Tyagi0% (1)
- LLDA vs. CADocument6 pagesLLDA vs. CARaymondNo ratings yet
- Testy 2014 C AnglictinaDocument4 pagesTesty 2014 C AnglictinaAntonioNo ratings yet
- Proposed Rule: Legal Assistance Eligibility Maximum Income GuidelinesDocument16 pagesProposed Rule: Legal Assistance Eligibility Maximum Income GuidelinesJustia.com100% (1)
- Packaging Procedures For Medical Waste DisposalDocument1 pagePackaging Procedures For Medical Waste DisposalStericycle100% (1)
- Taxation Ch3Document27 pagesTaxation Ch3sabit hussenNo ratings yet
- JPLG Human Resources - SomalilandDocument4 pagesJPLG Human Resources - SomalilandMohamed Ali100% (1)
- Arie Rimmerman-Family Policy and Disability-Cambridge University Press (2015) PDFDocument226 pagesArie Rimmerman-Family Policy and Disability-Cambridge University Press (2015) PDFWederson SantosNo ratings yet
- Wiesel Versus AppleDocument18 pagesWiesel Versus AppleMike Wuerthele100% (1)
- Internal Stakeholders IssuesDocument14 pagesInternal Stakeholders IssuesdivyadeoNo ratings yet
- Robert TilleyDocument10 pagesRobert TilleyAnonymous iI88LtNo ratings yet
- Closing The Gap: Health Coverage For Non-Poor Informal-Sector WorkersDocument30 pagesClosing The Gap: Health Coverage For Non-Poor Informal-Sector WorkersMuhammad Fikru RizalNo ratings yet
- Tele MedicineDocument12 pagesTele MedicineNoorul Faedzah RosliNo ratings yet
- Sangai English @bossboss Ar (PAS)Document10 pagesSangai English @bossboss Ar (PAS)Nguwruw Chungpha MoyonNo ratings yet
- Hci-Loi Gida Hhsra 092015 PDFDocument10 pagesHci-Loi Gida Hhsra 092015 PDFlevypamintuanNo ratings yet
- HRM Chapter 5Document14 pagesHRM Chapter 5Bibi Jamiatun MohamadNo ratings yet
- Equality Impact Assesment Milson RoadDocument5 pagesEquality Impact Assesment Milson RoadMasbro CentreNo ratings yet
- Letter From EPA Region 7 Administrator Karl Brooks To West Lake Community Advisory Group (CAG) Chairman Douglas Clemens, May 23, 2014Document2 pagesLetter From EPA Region 7 Administrator Karl Brooks To West Lake Community Advisory Group (CAG) Chairman Douglas Clemens, May 23, 2014EPA Region 7 (Midwest)No ratings yet
- Complaint in The Case of 75 Former NFL Players v. National Football League, Riddell Inc. Et Al.Document86 pagesComplaint in The Case of 75 Former NFL Players v. National Football League, Riddell Inc. Et Al.Michelle QuigleyNo ratings yet
- Otda Foil Request 2Document4 pagesOtda Foil Request 2sammyschwartz08No ratings yet
- Critique of The Nigerian National Health Plan and PolicyDocument7 pagesCritique of The Nigerian National Health Plan and PolicyUmeh ChukwudiNo ratings yet
- CA - Nov'21 (Date Wise)Document970 pagesCA - Nov'21 (Date Wise)MEHAK MALIKNo ratings yet
- BTC House Rules: Baguio Teachers' CampDocument1 pageBTC House Rules: Baguio Teachers' CampPoPo MillanNo ratings yet