Professional Documents
Culture Documents
Ergonomics Risk Assessment
Uploaded by
Yuli WicahyoCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Ergonomics Risk Assessment
Uploaded by
Yuli WicahyoCopyright:
Available Formats
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 1
Contents
EXECUTIVE SUMMARY ............................................................................................................... 5 - 6
1.0 PROJECT OVERVIEW.................................................................................................................. 7
1.1 Introduction........................................................................................................................................ 7
1.2 Langley Memorial Hospital ................................................................................................................... 7
1.3 Project Steering Committee................................................................................................................. 8
1.4 Intended Outcomes of the Project ................................................................................................... 8 - 9
1.5 Project Timeline and Plan ............................................................................................................. 9 - 11
1.6 Communication ................................................................................................................................. 11
1.7 Conclusion........................................................................................................................................ 11
2.0 MUSCULOSKELETAL INCIDENT ANALYSIS ......................................................................... 12
2.1 Introduction...................................................................................................................................... 12
2.2 Methodology for establishing baseline statistics ............................................................................ 12 - 14
2.3 Prioritizing By Department ........................................................................................................... 14 - 16
2.4 Conclusions ..................................................................................................................................... 17
2.5 Recommendations for future consideration ................................................................................... 17 - 18
3.0 RISK ASSESSMENT PROCESS AND TOOLS........................................................................ 19
3.1 Introduction...................................................................................................................................... 19
3.2 Conducting ergonomics risk assessment ..................................................................................... 19 - 20
3.3 Overall process for risk assessment ............................................................................................ 21 - 23
3.4 Department Specific Process For Risk Assessment ........................................................................... 23
3.5 Final report format ...................................................................................................................... 23 - 24
3.6 Challenges in Creating Risk Assessment Process and Tools ............................................................... 24
3.7 Conclusions ..................................................................................................................................... 25
4.0RISK ASSESSMENT DATABASE .............................................................................................. 26
4.1 Introduction...................................................................................................................................... 26
4.2 Development .................................................................................................................................... 26
4.3 Description of database .............................................................................................................. 26 - 27
4.4 Conclusion....................................................................................................................................... 28
5.0 CONDUCTING RISK ASSESSMENT ........................................................................................ 29
5.1 Introduction...................................................................................................................................... 29
5.2 Risk Factor Identification ............................................................................................................ 29 - 30
5.3 Risk Factor Assessment .................................................................................................................. 30
5.4 Risk Factor Control .................................................................................................................... 30 - 31
5.5 Follow-up on Recommendations ......................................................................................................... 31
5.6 Consultation and Communication During Risk Assessments .......................................................... 31 - 32
5.7 Challenges encountered .............................................................................................................. 32 - 33
5.8 Positive notes .................................................................................................................................. 33
6.0 GENERAL FINDINGS AND RECOMMENDATIONS ................................................................ 34
6.1 Introduction...................................................................................................................................... 34
6.2 Recommended program elements for MSI prevention..................................................................... 34 - 38
6.3 Facility-wide Findings of the Risk Assessments ............................................................................ 38 - 39
6.4 Facility-wide recommendations for MSI prevention based on general findings from the
risk assessments ....................................................................................................................... 39 - 42
7.0 DEPARTMENT-SPECIFIC FINDINGS AND RECOMMENDATIONS ..................................... 43
7.1 Introduction...................................................................................................................................... 43
7.2 Admitting including Bed Control and Switchboard .......................................................................... 43 - 44
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 2
7.3 Critical Care Unit .................................................................................................................................... 44
7.4 Diagnostic Imaging ......................................................................................................................... 44 - 46
7.5 Emergency ............................................................................................................................................ 46
7.6 Extended Care Units ....................................................................................................................... 46 - 47
7.7 Food and Nutrition Services ............................................................................................................. 48 - 49
7.8 Health Records ...................................................................................................................................... 49
7.9 Housekeeping ................................................................................................................................. 49 - 50
7.10 Laboratory ..................................................................................................................................... 50 - 51
7.11 Laundry and Linen Services ........................................................................................................... 51 - 52
7.12 Maintenance......................................................................................................................................... 52
7.13 Maternity and Pediatrics ................................................................................................................ 52 - 53
7.14 Medical Unit .................................................................................................................................. 53 - 54
7.15 Motor Services ..................................................................................................................................... 54
7.16 Operating Room including recovery room........................................................................................ 54 - 55
7.17 Pharmacy ..................................................................................................................................... 55 - 56
7.18 Portering ....................................................................................................................................... 56 - 57
7.19 Psychiatry ............................................................................................................................................ 57
7.20 Rehabilitation Services, including Occupational Therapy, Physiotherapy and Recreation .................. 57 - 58
7.21 Social Work ......................................................................................................................................... 58
7.22 Sterile Processing ......................................................................................................................... 58 - 59
7.23 Stores and Shipping/Receiving ...................................................................................................... 59 - 60
7.24 Surgical Unit including Surgical Day Care ....................................................................................... 60 - 61
8.0 PROJECT OUTCOMES......................................................................................................... 62
8.1 Introduction............................................................................................................................................ 62
8.2 Risk Assessments Reports Completed................................................................................................... 62
8.3 Recommendations from Risk Assessment Reports Completed ........................................................ 63 - 65
8.4 Intended outcomes ......................................................................................................................... 65 - 67
8.5 MSI incident statistics: comparisons at the projects conclusion ....................................................... 67 - 69
8.6 Project costs and savings ............................................................................................................... 69 - 70
8.7 Whats happening at LMH to affect change? ........................................................................................... 71
8.8 Project feedback from managers and steering committee members ................................................. 71 - 72
8.9 Conclusions ........................................................................................................................................... 72
9.0 CONCLUSIONS ..................................................................................................................... 73
9.1 What worked? ................................................................................................................................. 73 - 75
9.2 What would we change? ......................................................................................................................... 75
9.3 Whats next? ................................................................................................................................... 75 - 76
9.4 Acknowledgements ................................................................................................................................ 76
Appendix A
Table 1: Ergonomics Risk Assessment Project Plan and Timeline .................................................................. iii
Figure 1: Ergonomics Risk Assessment Project Plan and Timeline (Estimated vs. Actual) .............................. iv
Appendix B
Brief Review of MSI Statistics in the Healthcare Sector .................................................................................... v
Table B-1. General MSI Statistical Findings for LMH, 1998-2000 .................................................................... vi
Methodology for Priorization Based on Incident Statistics ............................................................................... vii
Below, results are shown for our example for all departments using the above equation. ................................. viii
The graphed results for the 10 departments are shown below. ......................................................................... ix
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 3
Appendix C
Workers Compensation Board of British Columbia Occupational Health and Safety Regulation;
Ergonomics (MSI) Requirements. ......................................................................................................... x - xi
C - 2, Overall Risk Assessment Process ................................................................................................... xii
C - 3a, Ergonomics (MSI) Risk Assessment Process Flow Chart ........................................................ xiii - xiv
C - 3b, Department Specific Risk Assessment Process with Consultation ............................................. xv - xvi
C - 4, Employee MSI Symptom Survey ........................................................................................... xvii - xviii
C - 5, Ergonomic (MSI) Risk Factor Identification and Assessment ............................................................. xix
C - 6, Ergonomic (MSI) Risk Factor Identification and Assessment;Sample final report .......................... xx - xxv
C - 7, Ergonomic (MSI) Risk Factor Identification and Assessment ........................................................... xxvi
C - 8, General Ergonomics Risk Factor Checklist ................................................................................... xxvii
C - 9, Office Ergonomics Checklist ....................................................................................................... xxviii
C - 10, Manual Material Handling Checklist ............................................................................................ xxix
C - 11, Patient Handling Checklist ................................................................................................. xxx - xxxi
C - 12, Risk Assessment Standards and Guidelines ..................................................................... xxxii - xxxiv
Appendix D
Ergonomic (MSI) Risk Factor Identification and Assessment ................................................................... xxxv
Ergonomics Risk Assessment Project Status of Recommendations ........................................................ xxxvi
Appendix E
Workplace Health and Safety ........................................................................................................ xxxvii
Procedures ........................................................................................................................................ xxxvii
Musculosketal Injury Prevention Program
NO MANUAL LIFT POLICY ........................................................................................................... xxxviii
Appendix F - 1
Summary Of Recommendations From Risk Assessments ..................................................................... xxxix
Appendix F - 2
Project Outcomes: Percent Change in Pre-Project Values vs. Post-Project Values ...................................... xl
Appendix F - 3
FOLLOW-UP SURVEY FOR MANAGERS
Ergonomics Risk Assessment Project at LMH...................................................................................... xli
Useful Web Sites..................................................................................................................... xlv - xlvi
References ................................................................................................................................xlvii - lii
Acknowledgements ........................................................................................................................... liii
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 5
EXECUTIVE SUMMARY
Musculoskeletal injuries (MSIs) are the most
common type of injury sustained by healthcare
workers. As a healthy, skilled and experienced
workforce is crucial to the provision of the best
patient care possible, employers must actively support
and carry out injury prevention strategies designed
to provide a safe and healthy workplace that will
retain and attract healthcare personnel and minimize
the high costs of injury.
Drawing on its commitment to leadership in health
and safety, the South Fraser Health Region (now part
of the Fraser Health Authority in Greater Vancouver,
British Columbia, Canada), applied for and received
funding in the amount of $140,000 from the Workers
Compensation Board of B.C. (WCB) for a compre-
hensive ergonomics risk assessment project. The goal
of the 18-month project was to conduct ergonomics
(MSI) risk assessments to provide a complete picture
of the risks associated with working in a medium-
sized acute care facility (including extended care
units). Intended outcomes included heightened
awareness of methods for reducing risk, data on risk
factors and recommended controls associated with
job functions, and reduced suffering, injury duration
and costs.
The project was defined and directed by a Steering
Committee with input from the Joint Occupational
Safety and Health Committee (JOSH). The scope
covered risk factor identification (e.g. force,
repetition, awkward posture), assessment and
recommendations for control measures for all
occupations at the facility. Specific project activities,
including risk assessments, were conducted on site
by an ergonomist.
Based on the multi-disciplinary nature of the topic,
stakeholders and setting, a communication plan was
devised and implemented. Monthly updates with
consultation on processes and opportunities for
feedback and input were provided. Information on
the projects plan, progress, specific activities and
results were regularly communicated through various
means such as presentations, newsletters, employee
bulletins and displays.
Initial research was conducted to collect and review
tools for risk assessment. A standardized method-
ology and practical tools for risk assessment
appropriate for the healthcare setting were
specifically developed for this project, as existing
tools to meet project objectives were not found. A
database was created to house the data collected with
the capability to generate reports on job-specific risk
factors and recommendations.
A flow-chart of an overall process for risk assessment
based on regulatory requirements was developed.
Applying a weighting scheme using site injury
statistics created a prioritized listing of department-
specific occupations for assessment. A symptom
survey that was short and easy to use was created
and distributed to staff to gather preliminary
information and employee feedback on risk factors.
On site assessments, job observations and interviews
were conducted to gather information. A series of
checklists appropriate for the healthcare setting were
developed to assist with the identification of risk
factors. Worksheets were designed to record relevant
information related to risk factors. A standardized
template to report and present risk assessment
information was designed.
A total of 120 risk assessments were successfully
completed within the projects timeline using the
established methodology and tools. Staff openly and
actively participated in all phases of the project and
feedback was positive. Completed risk assessment
reports contained information on risk factors
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 6
identified and assessed, with recommended control
measures linked back to risk factors and prioritized
to assist managers with implementation planning.
In many cases, the process confirmed risk factors
and control measures that managers were already
aware of and were addressing or provided additional
impetus for accomplishing change.
Based on the multi-factorial nature of risk factors
for MSI, risk was addressed by recommending a
variety of control measures. Emphasis was placed
on providing cost effective and quickly implemented
solutions. Capital items requiring longer-term
budgeting plans were also recommended where
appropriate. At the conclusion of the projects
timeline, some recommendations had already been
implemented. Further training, consultation,
evaluation and re-assessment will continue to take
place through the Fraser Health Authoritys
ergonomics program to assist with consideration and
implementation of outstanding recommendations
and to assess the effectiveness of controls
implemented.
A comparison of MSI incident data before and after
the project yields compelling results. Although there
was an increase in the frequency of both reported
MSIs (up 6%) and lost time MSIs (up 2%), there was
a corresponding decrease in severity (down 43%),
reflecting a substantial decrease in days lost and
WCB costs (down 44%). The average cost per MSI
WCB claim decreased by $1,200 and the average
days lost decreased 10.2 days. Overall, the project
yielded a net benefit to the organization of $74,000
when accounting for savings in WCB costs and costs
to run the project. These reported costs do not
include the costs to implement control measures
(costs were assumed by the individual departments)
and cost savings do not reflect indirect costs
(estimated to be 4 times the direct costs).
This project was conducted under the terms of the
contract and with the direction and input of the
Steering Committee. By completing assessments on
all occupations within the facility, WCB Ergonomics
(MSI) requirements with respect to risk identification
and risk assessment were exceeded. This decision
was made so that a complete set of risk assessments
for department-specific occupations would be
available. This was a large-scale undertaking,
however, the completed set of risk assessments can
now provide the groundwork for future MSI
prevention initiatives within the healthcare sector.
The expertise and knowledge gained from this in-
depth process will assist the Fraser Health Authority
in the development of a streamlined process for risk
assessment based on prioritization of occupations
and tasks and using the methodology, tools, data and
experiences gained from this project. Further
evaluation and follow-up including analysis of cost
effectiveness of implemented controls will be
conducted. In addition, this project will allow the
health authority to plan prevention activities for
target areas where immediate and sustainable results
can be demonstrated.
Others outside the health authority can use the
information from completed risk assessments as a
basis for conducting assessments within their own
facilities. The developed and field-tested tools and
methodology can be adopted by in-house personnel
so that significantly less time is spent on activities
associated with risk identification and assessment
and more focus can be placed on risk control.
The valuable data collected and information
presented through this process will assist in planning
and implementing prevention activities thereby
reducing injuries and their associated costs and
making healthcare a safer environment to work.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
7
ergonomic risk assessment and recommendations
of control strategies as per the WCB Occupational
Health and Safety Regulation (see Appendix C-1,
page x).
The project was to cover all tasks, including patient/
resident handling, material handling and computer-
based tasks. With few exceptions, all occupations
within the facility (120 occupations) were reviewed.
The projects scope included MSI risk identification
and assessment, and recommended controls. Due to
timeline constraints, implementation of recommend-
ations was not included as part of the projects overall
plan, although follow-up and reporting on outcomes
within the project timeline have been included and
will carry on after the projects completion.
1.2
Langley Memorial Hospital
Langley Memorial Hospital (LMH) is one of four
acute care hospitals in the South Fraser Health
Services Area of Greater Vancouver and serves the
City and Township of Langley, B.C. and surrounding
area. In one of the fastest growing communities in
B.C. with a population of 110,000, the hospital
provides primary care, specialized services and
geriatric services. Built in 1948, LMH has grown
from a 48-bed hospital to its current size of 430 beds
(200 acute care and 230 extended care). LMH is
staffed by over 800 full-time equivalents.
Langley Memorial Hospital was chosen as the
project site because it represents a typical medium-
sized facility in the province, provides a range of
services commonly offered at acute care centres
and, typical of many hospitals, has high
1.0
PROJECT OVERVIEW
What: Ergonomics (Musculoskeletal
1
Injury)
Risk Assessment Project
Where: Langley Memorial Hospital, Langley
British Columbia, Canada
When: February 2001 July 2002 (18 months)
Who: Project defined and directed by Steering
Committee; specific project activities
conducted by ergonomist; funding
provided by Workers Compensation
Board of B.C.
Project costs: $140,000 total, including salaries
and benefits, database develop-
ment and expenses (travel, office
supplies).
1.1
Introduction
The Fraser Health Authority (formerly comprised
of 3 separate health areas, including the South Fraser
Health Region), applied for and received funding
from the Workers Compensation Board of B.C.
(WCB) for a risk assessment project. The ergonomics
risk assessment component was one of four separate
risk assessments conducted at the hospital in Langley,
B.C. The other components (based on the most
common injuries to healthcare workers) included risk
assessments for chemical agents, bloodborne
pathogens, and workplace violence.
The goal of the ergonomics risk assessment project
was to determine which jobs/tasks contribute to
musculoskeletal injury (MSI), determine which
workers are likely to be affected, identify the nature
of the risks, and recommend control measures to
reduce the risk. This goal was attained through
1 For this project, a musculoskeletal injury or MSI is defined
as an injury or disorder of the muscles, tendons,
ligaments, joints, nerves, blood vessels or related soft tissue
including a sprain, strain and inflammation.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 8
musculoskeletal injury rates among its staff. The
intent is that the risk assessments methods, findings
and recom-mendations can be disseminated and
applied to similar settings province-wide.
The scope of the project was initially limited to
the acute care part of the facility but was later
broadened to include the 4 extended care units
(ECUs) which have a high proportion of the total
number of MSIs at LMH.
1.3
Project Steering Committee
The Project Steering Committee was comprised of
a multi-disciplinary team working together with
cooperation from the WCB, the Employer and
Unions. The project was initially laid out by the
steering committee consisting of representatives from
the health services area (Workplace Safety and
Wellness staff), the Hospital Employees Union
(HEU), the British Columbia Nurses Union
(BCNU), the British Columbia Government and
Service Employee Union (BCGEU), the Health
Sciences Association (HSA) and the WCB.
Throughout the duration of the project, the steering
committee continued to oversee progress with
monthly meetings and frequent communication.
The specific project activities, including
assessments, were carried out on site by an
ergonomist, with assistance as appropriate from
Health and Safety committee members and other
on-site staff (e.g. physiotherapists, occupational
therapists, department safety representatives).
1.4
Intended Outcomes of the Project
The purpose of the ergonomics risk assessment
project was to identify and minimize the risk of
musculoskeletal injury to healthcare workers. The
projects intended outcomes are outlined below,
with Section 8 of this report providing details on
final outcomes:
1.4.1
Meeting B.C. WCB Ergonomics (MSI)
Requirements
The risk assessment process was designed to review
all occupations at the facility to identify factors in
the workplace (such as force or awkward posture
required to perform a task) that may expose workers
to a risk of MSI, assess the degree of risk and
recommend controls. Consultation continued
through regular updates to Steering Committee
members, Joint Occupational Safety and Health
Committee members and senior management at the
facility. Periodic updates were also provided to LMH
Management staff for distribution to all employees.
1.4.2
Increased employee awareness of MSI
signs and symptoms, risk factors and
preventive strategies
It was intended that the project would increase
awareness of MSIs in the health care setting. The
project would determine what workers are at risk of
MSI and the activities they perform that put them at
risk. There would be increased worker awareness of
the signs, symptoms and risk factors for MSI. As well,
there would be increased awareness of the control
measures that can be put in place to reduce the risk
of MSI, including engineering and administrative
controls such as new equipment or improved design,
changes to work space and layout, and updated work
processes and practices.
The project was designed to increase awareness
through on-the-job observation, completion of
employee symptom surveys and through discussions
with employees as part of the risk factor
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
9
identification phase. Additional information
through presentations, pamphlets and newsletter
articles was used to heighten awareness of MSIs.
Identified departments received job-specific
information related to risk factors and injury
prevention strategies.
1.4.3
Establishment of tools for identifying,
assessing and controlling risk factors for
MSI
A set of tools for risk assessment has been
completed. Tools include flow charts outlining a
process for conducting a risk assessment, a method
for prioritizing based on MSI incident statistics, an
employee symptom survey, a task analysis worksheet,
a final report format documenting assessment
findings, and checklists to assist in risk factor
identification. A description and examples of the
tools used can be found in Section 3.0 of this report.
1.4.4
Reduced injury duration and costs
Injury statistics were compiled for the periods 1998-
2000 to provide baseline information, as well as for
2001 and part of 2002 (up to the projects end date).
A reduction in the number of work-related injuries
and their associated costs will positively impact
departments by resulting in less time loss and less
suffering for employees. In addition, there are
financial benefits in that there is less time to backfill
with other staff and WCB top-up costs are reduced.
1.4.5
Establishment of database of risk
assessment information
A risk assessment database was conceptualized,
designed and created to house data and information
from the risk assessments conducted. The database
features search capabilities on job tasks and variables.
Report generation capabilities include follow-up
reports on recommendations and reports on risk
factors associated with particular tasks for return
to work plans. More information on the risk
assessment database can be found in Section 4.0.
1.5
Project Timeline and Plan
From start to finish, the entire project was designed
to take 18 months, with a target completion date of
July 2002. An initial project plan and timelines were
proposed and approved by the steering committee
in early February 2001. The plan was to continue
the project steps as outlined (see Appendix A, page
iii - iv). As expected, there were some revisions and
updates to the project plan as time went on. A few
key points regarding each activity follows. Details
follow in subsequent sections of this report.
1.5.1
Fact gathering
The first undertaking was fact gathering; involving
meeting with external and internal resources,
gathering reference material including job lists and
department and contact names, and reviewing
relevant literature, web sites and other industry
guidelines. This information was used to establish
the initial project plan.
1.5.2
MSI incident analysis
The second major activity carried out was a statistical
analysis of MSI incidents at LMH. A review of 3
years of incident information was carried out using
various sources including the LMH and regional
Workplace Safety and Wellness incident database,
first aid reports, long term disability (LTD)
information, WCB claims information, and payroll
reports.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 10
1.5.5
Develop risk assessment database
A risk assessment database was developed as a means
of capturing and following-up on information
collected during the assessments, as well as providing
a valuable reference source. The database was
completed as per timeline, however there were delays
in the operation and input of reports into the
database, affecting generation of follow-up reports
using the database within the projects timeline.
These activities are in full operation as of Nov 2002.
1.5.6
Conduct risk assessments:
identification, analysis, control
The risk assessments themselves were carried out in
three steps: risk identification, assessment or analysis
of risk, and development of appropriate control
measures. Although each step is distinct and was
carried out in sequence, individual risk assessments
were conducted as mini-projects with start to finish
timelines ranging from one week to several months,
depending on the complexity of the assessment and
occupation analyzed. The target completion for all
120 risk assessments (as identified by the prioritized
list) was originally estimated at 10-12 months. In
actuality, it took closer to 14 months to complete
120 assessments and over the course of the project,
the job list grew to almost 140 jobs. The remaining
assessments (primarily single office workstations) are
to be scheduled after the project conclusion.
1.5.7
Report on outcomes and monitoring
Department-specific reports were completed as the
risk assessments were completed. There was, and will
continue to be, monitoring and follow-up on the
status of the control measures recommended. Re-
The incident analysis provided an initial focus for
the project as it effectively identified trends (what
workers were affected, what departments they
worked in, and what activities were performed that
put them at risk of MSI). This information was used
to establish a prioritized listing of departments to
assess, with target occupations identified within each
department. The prioritizing scheme chosen (based
on the findings of the incident analysis) demon-
strated that over 90% of the facilitys MSIs are
accounted for by only 20% of the department-
specific occupations. In addition, information from
the incident analysis provided a baseline for
comparison after the risk assessments had been
completed.
1.5.3
Develop risk assessment tools
The third key step involved the development of MSI
risk assessment tools, including process flowcharts,
report forms and checklists. This involved a review
of available risk assessment tools and checklists with
development of appropriate reports, worksheets and
checklists as the final goal.
1.5.4
Develop risk assessment process
A standardized approach under which each of the
risk assessments was to take place was documented.
As per the incident analysis prioritization, a risk
assessment was planned for all occupations within
each department, with priority based on those with
a demonstrated risk of MSI. As appropriate, a
team approach was used in that employees familiar
with the work tasks participated in both the
assessment phase (where risk factors were identified)
and in the development of appropriate control
measures.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
11
assessment will be performed as necessary (i.e.
when work practices change or new equipment is
installed).
1.6
Communication
It was noted early on that the key to project success
would be frequent and ongoing communication to
all stakeholders. Communication among those
directly involved in the project, those responsible for
the facility and all employees is essential.
The projects progress and activities were reviewed
monthly (either at meetings or by e-mails) with the
steering committee and Joint Occupational Safety
and Health Committee in order to provide regular
updates, get feedback and input, and obtain
suggestions and assistance in carrying out activities.
There was a concerted effort to provide ongoing
information about the project to all hospital staff
using various communication vehicles such as
presentations, hospital and regional newsletters,
e-mails, and bulletin boards.
Ongoing communication was carried out throughout
the life span of the project. Specific project initiatives
were publicized including the results of the MSI
incident analysis, the prioritized listing of jobs for
assessment, and the risk assessment process. In
addition, case study examples of completed risk
assessments were provided, including control
measures recommended. The intent was to
continually communicate with staff about the project
and keep the momentum and enthusiasm going.
1.7
Conclusion
Within the province of B.C., this comprehensive risk
assessment of patient/resident and material handling
tasks is one of the first, fully complete pictures of
risks for musculoskeletal injury associated with
working at a medium-size acute care facility. In
carrying out the project, it is intended that a
systematic approach be undertaken and that this
information is documented and available to other
healthcare employers and employees, unions,
healthcare associations, the Workers Compensation
Board and post-secondary educational institutes.
The expertise and knowledge gained from this in-
depth process will enable the Fraser Health Authority
and hopefully other stakeholders to plan and
implement MSI prevention activities.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 12
2.0
MUSCULOSKELETAL
INCIDENT ANALYSIS
2.1
Introduction
A key step in the overall project plan was the analysis
of musculoskeletal incidents. The following section
contains a summary of the methodology used and
findings of the statistical analysis of MSIs at Langley
Memorial Hospital. The analysis involved a review
of incidents over a 3-year period (1998-2000) using
various sources of data.
The original objectives of the statistical analysis
for the purposes of this project were to:
Identify departments, occupations and tasks
with a risk of MSI (based on reported incid-
ents)
Establish baseline statistics for comparison
purposes after risk assessments were compl-
eted (e.g. to do follow-up analyses and cost/
benefit analyses at the completion of the
project)
Establish a priority listing of departments and
occupations for ergonomics risk assessment
using baseline statistics information
2.2
Methodology for establishing baseline
statistics
2.2.1
Establish listing of departments and
occupations
At the beginning phases of the incident analysis, a
complete listing of departments and occupations
was compiled. In total, the final list consisted of
63 departments and 120 department-specific
occupations at LMH. As the timeline fit the ability
to complete assessments for all 120 occupations
(approximately 10 per month), the first objective
listed above was omitted. All departments and
occupations on the original list (120) would be
assessed. Department-specific assessments would be
completed as opposed to occupation-specific
assessments so that the reports and recommend-
ations could be tailored to the needs of the individual
departments with a more focussed scope and with a
single contact person (the department manager).
2.2.2
Conduct review of literature
A brief review of literature was completed to provide
an overview of injuries in the healthcare sector in
general, with emphasis on information specific to
B.C. where available. For a summary of provincial
statistics, see Appendix B, page v. In addition,
regional statistics (for South Fraser Health Service
Area) were compiled and presented. With few
exceptions, provincial and regional statistics (and
subsequently, LMH statistics) were consistent.
2.2.3
Compile data into spreadsheet format
For the incident analyses of LMH data, incident data
was compiled from the regions Workplace Health
database, first aid reports, long term disability (LTD)
information, WCB claims cost information, and
payroll reports. The most complete and accurate
information was obtained from the Workplace
Health incident database. The other sources of data
did not identify any additional departments or
occupations at risk for MSI beyond those identified
from the database, therefore the other sources were
excluded from the final analyses reports.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 13
Type of Injury (All Incidents)
MSI
55%
contusion
16%
cut
10%
needle poke
7%
other
4%
exposure/chem
4%
blood/body fluid
2%
burn
2%
Information from the incident database was queried,
downloaded into a spreadsheet, sorted, reviewed and
re-coded as necessary. Key fields were department,
occupation, type of injury (e.g. MSI, bruise, cut,
needle poke), activity/cause at time of injury (e.g.
patient transfer, material handling, slip/fall), and
body part affected. WCB data for claims costs and
days lost were subsequently added to individual
incident records.
Due to reported and noted limitations with data
prior to fall of 1999, the majority of statistical
analyses and reported findings were completed with
2000 data only, with reference to the previous 2
years for comparison purposes only. Patterns in
2000 data were similar to those in 1998 and 1999.
2.2.4
Compile and present findings
2.2.4.1
Summary of facility-wide findings
As previously mentioned, 3 years of data (1998
2000) from 5 sources (incident database, first aid
reports, LTD information, WCB claims cost
information and payroll reports) was originally
reviewed. The data showed similar trends across key
fields over the 3 years. Due to accuracy and
completeness, data from 2000 only was used in the
majority of the analysis and reporting, with
comparison to previous 2 years where appropriate.
A summary of the information is contained in
Table B-1 in Appendix B, page vi.
Highlights of findings:
Departments: Of 63 departments at LMH,
33(52%) reported at least one MSI from 1998
- 2000; while 30 departments (48%) had no
reported MSIs for this same time period. In
2000, 40% of MSIs occurred in extended
care facilities, with those facilities making
up 22% of the staff. In 1998 and 1999, 26-
27% of MSIs occurred in ECUs, so the trend
shows an increased percentage of incidents
in the ECUs.
Injury Type: In 2000, 55% of all reported
incidents were MSIs, and 77% of lost time
incidents were MSIs. Remaining injury types
include contusions, cuts, needle pokes, burns
and blood/body fluid exposure.
Occupation: 35% of MSIs are related to long
term care aides, 15% related to RNs, 13% to
food service workers, <10% each to cleaners,
LPNs and technologists.
Activity/cause at time of injury: 25% of
MSIs are related to patient transfer, 15% to
manual material handling, 12% to patient
repositioning, 10% to slips/falls, and <10%
each to awkward positioning, violent acts and
other patient care (e.g. bathing, dressing).
Body part affected: 32% of MSIs are related
to back, 26% to neck and/or shoulder, and
10% to multiple sites involving the back, neck
and/or shoulder. The remaining 32% include
wrist, elbow, hand/finger and knee.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 14
WCB information (from LMH incident
database): 89% of WCB claim costs in
2000 are related to MSIs. Over 90% of
days lost (WCB claims) are related to MSIs.
Claims costs: Based on 2000 WCB claims
at LMH, the average cost per MSI claim is
$3,020; with an average of 22.3 days lost
per MSI claim.
MSIs by Occupation
RN
15%
LPN
8%
Other
9%
Care Aide
35%
Food Serv Worker
13%
Cleaner
9%
Technologist
7%
Stores Attendant
2%
Porter
2%
MSIs by Activity
pt reposition
12%
slips/falls
10%
violent act
9%
pt care
7%
position
6%
push/pull
5%
other
4%
repetition
2%
mat handling
15%
patient transfer
25%
unknown
5%
2.2.4.2
Department specific reports
As part of the project and as an introduction to
the onset of risk assessments in the work area, a
department specific report on MSIs was provided to
each department at LMH.
The report consisted of 3 pieces of information:
Table B-1 (shown in Appendix B, page vi):
One column containing information for
LMH (2000) and another column containing
specific department information for comp-
arative purposes.
Pie charts by department for type of injury,
MSIs by occupation, MSIs by activity/cause
and MSIs by body part affected (similar to
the above pie charts).
A summary report from the injury database
containing incident identifying information
and a description of the incident.
2.3
Prioritizing By Department
2.3.1
Prioritization Scheme
In order to allow the project to schedule
departments for ergonomics risk assessment based
on need, a system of prioritizing the facilitys 63
departments and 120 occupations was used.
Incident statistics for the 3-year period 1998-2000
were used to establish a 3-category prioritization
system. Prioritizing by departments was chosen as
the best way to prioritize so that subsequent effort
focusing on risk assessment and control could be
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 15
developed around departmental input and
reporting.
The criteria for assigning priority was established
once the baseline statistics were initially reviewed
and a workable system was selected.
Priority 1 was assigned to departments that
had more than 1 reported MSI in any of the 3
years 1998-2000 (26 departments).
Priority 2 was assigned to departments that
had 1 reported MSI in any of the 3 years (7
departments).
Priority 3 was assigned to the remaining
departments that had no reported MSIs in
any of the 3 years (30 departments).
The priorities assigned provide a clear picture of
the facilitys MSIs, demonstrating where efforts for
ergonomics risk assessment should be concentrated:
For 2000 data, 98% of reported MSIs are attri-
buted to the 26 priority 1 departments, with
the remaining 2% attributed to priority 2
departments. (Note: When accounting for
unknown/uncoded departments in 1998 and
1999, the same holds true for those 2 years
as well).
Within the 26 priority 1 departments, only
34 department-specific occupations account
for 92% of the reported MSIs, with 1-3 occu-
pations per department affected.
2.3.2
Weighting Priority 1 Departments
Twenty-six departments were classified as priority
1 as these departments reported more than 1 MSI
over a 3-year period. Where to start? Priority 1
departments were then further ranked to determine
the order in which these departments should be
assessed.
The method chosen for ranking priority 1
departments was based on a method developed and
used by Simon Fraser Health Service Area (BC) and
provided by Waqar Mughal (Ergonomist, Simon
Fraser). The method provides a means of accounting
for multiple variables in prioritizing.
Six variables were chosen for consideration in the
prioritization scheme. The variables (listed
below)were each assigned a subjective rank in terms
of importance. Based on this rank, an inverse
weighted value is then assigned to the variable. A
rank of 1 would yield the highest weight of 6. Two
variables can have the same rank, the weighting is
then divided (e.g. if there are two variables ranked
as 1, each is assigned a weight of 5.5 based on the
average of 5 and 6 values). The value of each
variable in the equation is then calculated (by
dividing it by the highest value of others in the group
multiplied by its weight) and the sum of these 6
numbers becomes the final weighted score.
The following rank and weights were used:
Variable Rank Weight
Number of lost time MSIs 1 5.5
Lost time per full time
equivalent (LT/FTE)
1 5.5
Number of MSI incidents 3 3.5
MSIs per full time
equivalent (MSI/FTE)
3 3.5
% of MSIs that are lost time 5 2
% of incidents that are MSIs 6 1
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 16
P
s
y
c
h
ia
tr
y
R
e
c
T
h
e
ra
p
y
S
u
rg
ic
a
l
P
e
d
ia
tric
s
O
p
e
ra
tin
g
R
o
o
m
P
h
y
s
io
th
e
ra
p
y
A
L
C
M
a
te
r
n
ity
E
C
U
4
E
m
e
rg
e
n
c
y
D
ia
g
n
o
s
tic
Im
a
g
in
g
M
e
d
ic
a
l2
C
C
U
L
a
b
o
r
a
to
r
y
E
C
U
3
P
o
rte
rin
g
S
te
rile
P
ro
c
e
s
s
in
g
M
e
d
ic
a
l1
H
o
u
s
e
k
e
e
p
in
g
S
to
re
s
M
o
to
r
S
e
r
v
ic
e
s F
o
o
d
/N
u
t
E
C
U
2
E
C
U
1
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
10.00
11.00
12.00
13.00
14.00
15.00
16.00
17.00
18.00
19.00
20.00
This is a great method for:
Using multiple variables to determine prior-
ity (e.g. prioritizing is not only based on one
variable such as the number of incidents).
Allowing a means of prioritizing smaller de-
partments even though they may have small
staff numbers and therefore small numbers
of incidents.
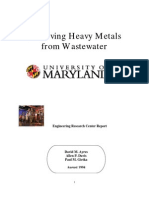
The following figure shows the results of the
weighting system for priority 1 departments.
{(Note: only 24 departments are shown since two
priority 1 departments did not have any reported
MSIs in 2000). Note that the graph can also be
used to signal a change in slope, indicating
departments above a cut-off that should undergo
intervention.}
A brief description, table and charted results of
the weighting system for a non-descriptive set of
departments are shown in Appendix B, page vii-ix.
Figure 2.4: Weighted Scores by Department, LMH 2000
Departments
W
e
i
g
h
t
e
d
S
c
o
r
e
s
2000 MSIs per Department at LMH
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 17
2.4
Conclusions
2.4.1
Challenges
Completing the incident analysis presented some
challenges. Some incident information was
incomplete or not available. There was some manual
review of the data, as well as some additional
researching, reviewing and re-coding to ensure
accuracy and consistency of statistics.
The end findings of the incident analysis though,
were well worth the efforts. The findings clearly
show those departments, occupations and tasks that
are at risk for MSIs. The information gives a focused
picture of where initial efforts need to be directed.
2.4.2
Regional Staff
Over the course of the last 3 years, the South Fraser
Health Services Area has been fortunate to have staff
dedicated to looking after the incident database and
reporting systems (Access database). This is a
valuable resource for improving access to accurate
information and has made the job of obtaining
information much faster and more efficient. Access
to information will continue to improve with a new
incident/injury form (with additional options for
coding) and tracking of individual claim costs. For
the purposes of this project, the most recent (2000)
data was easy to query, was accurate and complete,
and will provide a suitable baseline for comparisons
to be easily done in the future.
2.4.3
The Role of Prioritization
The prioritization of departments using MSI
incidents was a highly effective and essential tool
for this project. The statistics compiled using
information from the incident database largely
reflected statistics reported in both the literature
review and provincial and regional WCB statistics.
Coupled with task observations and employee
symptom surveys as components of the risk
assessment process, an accurate picture of MSIs does
unfold.
In a context outside this project, where time and
resources are not available to review all of the
occupations within the facility, prioritization is
arguably essential. The prospect of doing risk
identification and assessment for all workers that
may be exposed to a risk of MSI (as per WCB
regulations) is daunting in a large and diverse setting
such as a healthcare facility. Indeed, it is hard to
find any occupation that does not have risk factors
for MSI. It is therefore essential to establish priorities
around what specific occupations and tasks will be
reviewed in decreasing order of risk so that areas in
most need of intervention are targeted and assessed
first.
The use of incident statistics to identify target areas
is a reasonable starting point. The analysis completed
for this project showed that the identification and
prioritization of a workable number of departments
and occupations is feasible. Only 34 department-
specific occupations accounted for the majority
(>90%) of the MSIs within this facility and this may
be a suitable process to adopt in other facilities.
2.5
Recommendations for future
consideration
2.5.1
Encourage reporting of all incidents
The statistical review showed that there may be
under-reporting of incidents as evidenced by the fact
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 18
that 31% of all reported incidents in 2000 were
lost time. The incident analysis highlights the need
to encourage the use of the injury/incident form
for all incidents, including first aid reports from
Emergency, near miss incidents and incidents where
no time was lost. There should be ongoing
communication to staff to ensure all incidents are
tracked within this one reporting system.
2.5.2
Providing departmental statistics
In preliminary discussions with staff when initially
compiling the statistics, it is apparent that there is a
need for a process of providing statistics at a
department level, including frequency and severity
rates and absenteeism data. Database information
is currently provided monthly to the joint
occupational health and safety committee.
Department statistics were compiled as part of this
project at the beginning and at the end of this project.
Further initiatives within Finance and Workplace
Safety and Wellness will continue to provide ongoing
information on WCB statistics and costs per
department on a quarterly basis with the view to
expand this to absenteeism data in the future.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
19
3.0
RISK ASSESSMENT
PROCESS AND TOOLS
3.1
Introduction
The purpose of the WCBs Ergonomics (MSI)
Requirements within the Occupational Health and
Safety Regulation (see Appendix C-1. page x-xi ) is
to eliminate or minimize the risk of musculoskeletal
injury to workers. Three key steps as outlined in their
requirements and publications are risk identification,
risk assessment and risk control. As stated in the
regulation:
Risk identification: The employer must ident-
ify factors in the workplace that may expose
workers to a risk of MSI.
Risk assessment: When factors that may
expose workers to a risk of MSI have been
identified, the employer must ensure that the
risk to worker is assessed.
Risk control: The employer must eliminate or
minimize the risk of MSI to workers.
As stated in the requirements, risk factors to assess
include force, repetition, duration, work postures,
local contact stresses, working reaches, working
heights, seating, floor surfaces, load size and shape,
work-recovery cycles, work rate and task variability.
3.2
Conducting ergonomics risk assessment
3.2.1
Definitions
For the purposes of this project, the general term
risk assessment is used to describe the 3-step
process of risk factor identification, risk factor
assessment and development of risk controls.
Ergonomics (or MSI) risk assessment is defined as
the analysis of the ergonomic risks of a job. The risks
are identified and assessed or evaluated, and
appropriate controls recommended.
3.2.2
Objectives
The objective of this phase of the project is to develop
a process and tools (forms, worksheets and
checklists) for identifying and assessing risk factors
for MSI and making appropriate recommendations
to eliminate or reduce risk. The process will outline
a simplified overall process as well as the specific
process carried out within the departments for
conducting the risk assessments (i.e. what specific
steps were followed). These processes are depicted
in a flow chart format in Appendix C-2 and C-3,
page xii-xvi.
The specific forms, checklists and worksheets as
referred to in the flow chart can be found in
Appendix C-4 to C-11, page xvii - xxxi). These tools
can be used to assist with job observations, identify
risk factors, gather employee feedback, record the
findings of the assessment and report findings to the
department.
3.2.3
Assumptions
The process outlined assumes that:
the organization has designated assessor(s)
responsible for risk assessment (e.g. MSIP
Advisor, Ergonomist, Health and Safety Ad-
visor, Rehabilitation staff) as part or their job
functions, and
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
20
the assessor(s) have some basic levels of
expertise in task analysis and ergonomics risk
assessment.
3.2.4
Establishing a process
Establishment of the process involved a review of
literature where similar processes are outlined, and
INPUT/SOURCES OF INFORMATION
Injury/incident statistics
Employee symptom survey
Meetings and discussions with employees
Job observations of workers performing
tasks
Workstation and work area measurements
Review of documentation (e.g. job descrip-
tion, work procedures)
Checklists
Review of work measurements
Comparison with ergonomics guidelines
and standards
Compilation of information from surveys,
job observations, employee discussions
Review of existing controls, controls imple-
mented and those that can be implemented
Review existing controls
Document controls immediately imple-
mented
Recommend appropriate and practical
controls
STEP
1. IDENTIFICATION
C
O
N
S
U
L
T
A
T
I
O
N
applying an approach typically used for the conduct
of an ergonomics audit or assessment. The process
was reviewed by the project steering committee and
joint occupational safety and health committee, and
was communicated to staff via the newsletter,
monthly management presentations in person and
as assessments took place within individual
departments.
3.3 Overall process for risk assessment
A depiction of the overall process for risk assessment
2. ASSESSMENT
3. CONTROL
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
21
input from staff members as to body discom-
fort, problem tasks to assess and suggestions
for improvement. The Employee MSI
Symptom Survey can be found in Appendix
C-4, page xvii.
Discussions with employees: Informal
discussions with staff occurred to get feed-
back and input into tasks for assessment, and
to request information related to discomfort
and suggestions for improvement. Meetings
were also held to gather documentation such
as job descriptions, work procedures, nursing
manuals, MSIP program information and
equipment inventory for example.
Job observations of workers performing
tasks: Job observations were scheduled as
required; over various days, various shifts and
with various staff. Depending on the nature
of the occupation and tasks for assessment and
number of staff, observations typically took
anywhere from 1 - 2 hours in on shift to 16 -
20 hours over 4 - 8 shifts. Frequently performed
and problematic tasks were observed as
identified from the task analysis, employee
discussions and symptom survey.
Workstation and work area measurements:
During the job observations, measurements
were taken wherever possible in order to
quantify risk factors for MSI. A force gauge
and tape measure were the primary measure-
ment tools used. Measurements were taken for
variables such as push/pull forces, weights of
objects lifted, heights of counters and working
surfaces and sizes of objects handled.
Review of documentation: Review of
department documentation including job
3.3
Overall process for risk assessment
3.3.1
Risk factor identification
Identification of risk factors for MSI was compl-
eted using the following information:
Injury/incident statistics: Details of incid-
ents within departments (from MSI incident
analysis described in previous section)
provided information on what specific tasks
to assess as well as providing information on
potential risk factors.
Employee symptom surveys: Surveys
(anonymous and voluntary) were distributed
to employees by various means (meetings,
mail, posted on bulletin board). The survey
was intended as a mechanism for employee
feedback on potential risk factors for MSI,
to provide a means of measuring employee
perceptions of psychosocial factors (job de-
mands, job control and time pressure),
and to measure awareness of signs, symptoms
and risk factors for MSI. Key comment areas
on the survey included a body diagram for
employees to indicate location and severity of
discomfort, cause or activity that employees
attribute to their discomfort, problematic tasks
that they feel should be reviewed or undergo
assessment and their suggestions for improve-
ment. Return rates were generally higher for
smaller departments (approximately 75 - 80%),
dropping to about 20-50% for larger depart-
ments with more staff. When return rates
were lower, staff was offered further encour-
agement to fill out the surveys (e.g. by handing
them out, and having manager send an e-mail).
In addition, efforts were made to gather verbal
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
22
Examples of information in the assessment column
include:
Additional information on risk factors identi-
fied; e.g. description of work area with more
detailed measurements of workstations,
including information on magnitude, duration
and frequency.
Comparison of measured exposures with
anthropometric data and ergonomics stand-
ards, guidelines and caution zones where
available (e.g. RULA, NIOSH, Snook tables,
CSA office ergonomics).
Information from the symptom surveys (6
questions to measure job control, time pressure
and workload) to quantify psychosocial
variables that may be influencing work
performance.
Additional notes related to employee percep-
tions, comments and observations during the
job observation sessions.
Comments on control strategies that are exist-
ing or could be implemented in relation to the
identified risk factor.
Risk factor assessment should be performed by
people who understand the work processes, MSI risk
factors, and the principles of risk assessment and
control. The basic principles of risk assessment
involve looking at the extent of exposure to assess
the risk, including magnitude (how much), duration
(how long) and frequency (how often). Columns on
both the task analysis worksheet and the risk
assessment report form are structured to identify this
information. Depending on the level or expertise of
the assessor and/or the complexity of the risk factors
descriptions, work procedures, and policies
was conducted where information was
available and relevant.
Checklists: Checklists were used to assist in
the identification of risk factors. A reference
list of available checklists and identification
tools (Appendix C-12, page xxxii) and sample
checklists and worksheet are appended
(Appendix C-7 to C11, page xxvi-xxxi).
3.3.2
Risk factor assessment
Risk factor assessment is intended to be a formal
means of assessing the severity of risk. Interestingly,
the thesaurus shows synonyms for assessment
include such wide-ranging terms as estimation,
opinion, consideration, judgement and measure-
ment.
In order to capture the flavour of both measurement
and opinion/judgement, the final report form was
designed with a text-based column for assessment
labelled Assessment, Observations, Comments.
This is essentially the risk assessment. For this
project, no attempt was made to quantify or prioritize
the severity of risk, nor apply a scoring system to
the risk assessment process. The intent is that for
each risk factor identified, information in the
assessment column is compiled and interpreted to
form the basis for a decision as to whether or not
control measures are required e.g., by reviewing work
measurements and comparing them with ergonomics
guidelines and standards (where in existence),
compiling information from surveys, job
observations and employee discussions, and
reviewing controls. A listing of standards and
guidelines used can be found in Appendix C-12, page
xxxii.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
23
assessed, additional assistance and guidance may be
sought (e.g. from WCB or consultant). In other cases,
the need for controls may be obvious or the risk
factors identified can lead directly to risk control (e.g.
repositioning a monitor to correct awkward neck
posture).
3.3.3
Risk factor control
For those risk factors that the assessment determined
there was a need to address, appropriate risk controls
were devised. In some cases multiple controls were
recommended per risk factor or multiple risk factors
were addressed per control.
Possible control measures were considered using a
standard hierarchy of control model, with control
measures at the top giving better results:
Elimination (e.g. eliminate the need to perform the
task, remove or replace the hazardous tool or
equipment)
Substitution (e.g. use a different tool or
machine, use a different work method)
Engineering Control (e.g. redesign
work area or workstation, provide lifting equipment)
Administrative Control (e.g. resched-
ule work, rotate employees)
Personal Protective Equipment
(e.g. knee pads when kneeling)
An important part of the entire process was to ensure
agreement and buy-in with the recommendations.
The report with recommendations was prepared in
draft and reviewed with the department contact
person prior to issuing. Appropriate revisions were
made in order to ensure that identified risk factors
were addressed with appropriate controls.
Additional reference information on the design of
risk controls and common risk control options can
be found in Appendix C-12, page xxxii.
3.4
Department Specific Process For Risk
Assessment
It was necessary to take the simplified 3-step process
for risk assessment and develop a specific protocol
for conducting risk assessments within the facilitys
various departments. At Langley Memorial Hospital,
the final job tally was over 120 department-specific
occupations for risk assessment. A 12-month
schedule was developed, with a target of 10
completed assessments per month. Priority (1, 2 or
3) was assigned to departments as per the
prioritization scheme described in the previous
section on MSI incident analysis. Higher priority
departments were started within the first 6-8 months
with lower priority assessments scheduled
throughout to keep the project timeline intact.
The specific steps used to conduct risk assessments
within individual departments are shown in
Appendix C-3a, page xiii in a flow chart format. This
chart was provided to department managers for
communication to staff. Appendix C-3b, page xv
contains the same information with notes on
consultation added.
3.5
Final report format
The final report form is laid out to lead both the
assessor and the reader from task analysis, to the
identification of risk factors per task, to their
assessment, to their recommended controls.
Appendix C-6, page xx-xxv contains an example of
a completed risk assessment report.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
24
Challenges encountered:
Existing risk assessment tools that meet all the
above objectives were not found.
There are few examples of a risk assessment
protocol which provides a process and appro-
priate forms to take the assessor through all
stages of identification, assessment and
control and that is suitable for the wide range
of tasks encountered in the healthcare setting.
When suitable reference material was obtain-
ed, it was often deemed suitable for a certain
type of task but not another (e.g. good for
patient handling or material handling but not
both).
Many people reported taking existing tools
and modifying them to suit their own specific
purposes. It seems in anthropometric terms,
one size does not fit everyone.
Of the screening tools available, checklists
provide the most formal and orderly means
for gathering information. While widely avai-
lable and in use, many checklists have not been
scientifically validated, specifically ones with
scoring systems included.
When performing the specific step of risk
assessment where the level or risk is to be eval-
uated, the question of what level or amount
of exposure is harmful to the musculoskeletal
system is often a difficult one. Current scien-
tific knowledge is a limiting factor and there
are few validated ergonomics standards.
Guidelines for preventing MSI only give
direction, not absolute limits.
A task analysis worksheet was used to assist in
documenting a task list, an important first step when
starting individual assessments. The worksheet
provides room for job summary, a description of
tasks, their frequency/duration and reasons for
inclusion or exclusion in risk assessment. The most
frequently performed and most problematic (from
an ergonomics perspective) tasks should be assessed.
For more information on task analysis, consult A
Guide to Task Analysis (1992 Kirwan & Ainsworth)
or other reference material on the subject.
By task analyzed, risk factors for MSI were identified,
with columns for type of risk factor identified (e.g.
awkward posture, force), frequency/duration
quantities and magnitude and range (e.g. joint angles,
working heights, weights lifted and push/pull forces).
For the purposes of tracking and follow-up, each risk
control was linked to a risk factor, with a code for
type of risk control (e.g. training, new equipment,
work procedure) with status and date implemented
fields. In addition, a control priority scheme was
established to assist managers in determining the
immediacy of the recommendations.
3.6
Challenges in Creating Risk Assessment
Process and Tools
Establishment of the process for risk assessment and
tools (worksheets, checklists and report format) was
very challenging. As outlined in project committee
meetings and documentation, the tools had to
identify risk factors for MSI (as per WCB
regulations), include psychosocial factors, provide
some means of assessing or measuring risk as well
as be practical and simple for application in other
facilities by other people. In addition, the information
had to be presented in a format that was workable
for a database.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
25
3.7
Conclusions
After completing almost 120 risk assessments in a
13 month period, the following points are tabled:
There were time constraints even with an 18-
month timeline and a full-time ergonomist
(dedicated solely to the project) to effectively
complete risk assessments at one facility. When
applying this process to a broader setting, it
will be necessary to prioritize areas for risk
assessment and use the tools outlined in risk
factor identification to prioritize specific
problematic tasks for risk assessment. This
should yield the highest cost efficiency as well
as providingan efficient means for risk assess-
ment to be one component of an overall
ergonomics program.
The most effective sources of information on
risk factors for MSI were from the employees
who are performing the tasks on a daily basis.
Information from the symptom surveys and
informal discussions during job observations
were invaluable and provided an efficient and
accurate means of identifying risk factors.
A key component of the process was review-
ing the draft report with manager and other
staff. This step allowed for essential input into
the accuracy of the information and to the
effectiveness of proposed controls. It also
helped emphasize the importance of the
process and of following through with imple-
menting recommendations.
It was a very difficult task to devise a simplified
process and tools for ergonomic risk assess-
ment within the healthcare setting that has
widely different and varied complexities of
tasks. In the end, it is recommended that staff
be designated and trained to perform risk
assessment and that they have the opportunity
to perform risk assessment on a continual basis
to improve and maintain their skills. It is
beneficial if this person has some basic levels
of expertise in task analysis and/ or ergo-
nomics risk assessment prior to taking this on.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 26
4.0
RISK ASSESSMENT
DATABASE
4.1
Introduction
For this project, a risk assessment database was
conceptualized, designed and created to house data
from the risk assessments conducted. The original
idea was that the database would house data from
all four components of the risk assessment project
at LMH (ergonomics, blood and body fluids,
chemical and violence) and would have the capability
to generate reports on all risk factors associated with
a particular occupation or department.
For the ergonomics (MSI) component of the risk
assessment project, a database was designed and
created to contain all the information from the
individual risk assessments. Common descriptive
fields related to the occupations (e.g. job title,
department, site) are linked to the other databases
so that an overall profile of risk per occupation can
be generated.
The database has the capability to produce custom
queries and reports. As well, the database format
allows for search capabilities on all variables e.g.,
job tasks, and task variables such as risk factors
identified, frequency and magnitude, and body part
affected. Report generation capabilities include
summary reports of risk assessment findings, follow-
up reports on recommendations and reports on risk
factors associated with particular tasks for return to
work plans.
4.2
Development
The development of the database was contracted
to an outside consultant. The Access 2000
database was developed using the final risk
assessment report form as a guide (Appendix C-6,
page xx). All fields contained within the report are
also contained within the database.
The databases primary uses will be for generating
queries and reports and using its search capabilities
(e.g. to search on specific risk factors, body parts
affected and weights lifted). Custom queries and
reports can be designed as required.
Information required by the consultant for the
definition and design of the database was provided
in May 2001, 4 months after the start-up of the
project and after the fields and data of interest had
been finalized. The consultant spent 3 months
developing the database, and preliminary testing was
conducted in October 2001. The computer system
to run the database on site had to be upgraded with
both software and hardware components. This
created significant delays in that the database was
not ready for data input until March 2002. At this
point, due to lack of resources for data entry, only a
sample of reports was input by the project deadline
of July 2002. As of November 2002, data entry
has been completed.
4.3
Description of database
The database is designed to contain all the
information collected and compiled from the
ergonomics risk assessments. All fields contained in
the final report format are also contained within the
database as well as some additional fields related to
the recommendations for tracking, follow-up and
analyses of cost effectiveness. The intent was to have
the database generate a summary report for
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 27
managers (similar to the final report format).
However, due to the above mentioned time
constraints, all reports sent to managers were
completed via word processing software. Future risk
assessments completed and entered into the database
will have the final report generated by the database.
A sample summary report generated from the
database is contained in Appendix D, page xxxv
(page 1 of 4 is included).
In addition, the database has the capability to
generate reports for specific return to work plans that
can be sent to health care professionals. The reports
will contain information on selected fields related
to the task analysis (e.g. listing of the tasks
performed), risk factors and body parts affected to
provide an overview of task demands. Reports can
be customized (e.g. available fields selected) based
on specific needs.
The database also has the capability to generate
reports on the status of recommendations made as
a result of the risk assessments. These reports will
be generated quarterly and will serve as an easy and
effective follow-up tool for managers. As managers
provide information on the status of the
recommendations, it will be input into the database.
A sample report on status of recommendations from
the database is contained in Appendix D, page xxxvi.
The database also contains a symptom survey tool
for housing the results of the symptom surveys.
Summary information compiled from the results of
the symptom surveys can be provided back to
individual departments. In the absence of this having
been completed within the projects timeline, manual
compilations were conducted and summary reports
sent to managers on request. As the data is input,
we will have the ability to generate statistics (and
graphs) on the results for example, by occupation or
department. These baseline statistics will prove
useful for comparison purposes as follow-up surveys
are used.
Additional features of the database:
All information contained in the header is
consistent with the other risk assessment
database components and the common fields
are linked.
Many fields have pre-determined look-up
tables for entry to maintain consistency. In
addition, the look-up tables have the same
listing as other department databases (e.g.
injury/incident database) again, to ensure
consistency and continuity of data.
The database is designed to accept reports
from other facilities, so that risk assessments
from all facilities throughout the health
authority can be input.
The database contains a survey tool. Other
surveys can also be added and reported on.
The recommendations for controls are all
linked back to risk factors and their assoc-
iated tasks. This will assist in determining
what risk factors have been eliminated by the
implementation of controls.
The controls are all coded for priority, type
(e.g. training, work process, maintenance,
minor capital, major capital), status (e.g. in
place, implemented, in progress, outstand-
ing), date and person responsible. This will
allow for reporting on a variety of parameters
such as percentage of recommendations
related to training, number of capital items
recommended, type of controls recom-
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority 28
mended for RN positions and outstanding
recommendations for a particular depart-
ment or contact name. These are just
examples; the database has the capability to
report on virtually all information and fields
input.
The database also contains fields for
estimated and actual costs of recommend-
ations.This will allow for accurate and
detailed cost effectiveness analyses to be
conducted in the future e.g. average cost of
recommendations per report, average cost for
capital items etc.
4.4
Conclusion
Due to unanticipated delays with getting the
database operational, this portion of the project has
not met the original intended timeline. Although the
database was ready for input in March 2002, the risk
assessments were ongoing leaving little additional
time for data entry. As a result there has not been
the opportunity to take advantage of report
generation capabilities within the timeline of the
project.
The decision was made to input a sample of reports
within the projects timeline, and all data input was
completed by Nov. 2002. In the future, there will
also be time devoted to improving the report
generation capabilities to provide additional well
designed reports. As this is completed over the next
6 months, it is expected that the database will
become a valuable resource of risk assessment
information for the health authority.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
29
5.0
CONDUCTING RISK
ASSESSMENT
5.1
Introduction
The following section describes the application of
the risk assessment process as it was applied to the
120 assessments completed at the facility. Specific
examples of how the process was applied to the
assessment for the LPN on the medical unit are
provided. The challenges encountered are also
discussed.
To recap, for the purposes of this project, ergonomics
risk assessment is defined as the analysis of the
ergonomic risks of a job. The risks are identified and
assessed or evaluated, and appropriate controls
recommended. Specific activities are outlined below
with important steps of the risk assessment process
highlighted. The highlighted points can be summarized
into the series of general steps that reflect the overall process
for risk assessment. The overall process is depicted in flow
chart format in Appendix C-3a, page xiii-xiv.
5.2
Risk Factor Identification
The priority listing of departments for risk
assessment was established using a weighting
scheme including variables for the total number of
MSIs and percent of MSIs per staff. Incident data
from 1998, 1999 and 2000 was analyzed. Refer to
Section 2 for more detail. Based on this priority,
initial contact was made with the department to
introduce the project and discuss logistics for
carrying out the risk assessment.
In this case, a meeting was held with the Nurse
Manager of the Acute Care Medical Ward to discuss
the project and review the findings of the MSI
incident analysis. In this department, 45% of
incidents were MSIs, reflecting 80% of lost time
incidents. By occupation, 50% occurred with LPNs
and 50% with RNs. With regards to activity at the
time of the incident, 90% were related to either
patient transfers or repositioning in bed. For body
part affected, 80% were related to back, neck and/
or shoulder. These findings were typical of other
occupations in other work areas of LMH that
involved direct patient care.
The anonymous and voluntary symptom survey was
distributed to staff. An envelope of blank surveys
and one marked for completed surveys were posted
in the wards break room area. A notice was sent by
the manager to all staff to encourage them to
complete the survey. The department achieved a 50%
return rate on the survey. They cited lifting patients
in bed and lifting and pulling heavy patients as
problematic tasks. They suggested that more staff,
lower workload, more training, more equipment and
more input into equipment purchases and
renovations would make their jobs easier.
Documentation related to the job was collected
including a job description for LPN (Medical) and
listing of job duties. This information was used to
establish a preliminary task list. A worksheet was
used to assist in documenting the information
including a description of the task and its frequency/
duration. Task analysis for nursing duties tends to
be complex. Hospital documentation is very general
(e.g. task is described as provide nursing care) and
specific tasks vary widely depending on individual
patient needs. The primary tasks for risk assessment
were documented as conduct rounds for patient
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
30
care (e.g. bathing, dressing, toileting); perform
nursing procedures (e.g. changing dressings, taking
vitals); assist with patient transfers/patient
handling; assist with meals (e.g. serving, feeding);
and chart patient information. Some tasks were
further broken down into more detailed sub-tasks
(e.g. type of patient transfer such as bed
repositioning) for the purposes of the assessment.
Job observations were then scheduled over various
days, various shifts and with various LPNs. The ward
is staffed with LPNs from 0730 1930. Job
observations were conducted to cover the majority
of this time frame, over approximately 6 sessions
varying in length from about 2-6 hours. Daily
(frequent) and problematic tasks as identified from
the task analysis, through employee discussions and
the results of the symptom survey, were observed.
During the job observations, measurements were
taken wherever possible in order to quantify risk
factors for MSI. A force gauge and tape measure
were the primary measurement tools used.
Measurements were taken for variables such as push/
pull forces (e.g. when pushing a patient in mechanical
lift), weights of objects lifted (e.g. patient charts and
stock items), and heights of counters and working
surfaces (e.g. nursing station, bed heights). Notes on
risk factors and diagrams of joint postures by task
were compiled. General checklists (see Appendix C-
8 to C-11, page xxvii-xxxi, for examples) served as
reminders for potential risk factors.
5.3
Risk Factor Assessment
The information from the above risk identification
steps were compiled into a final draft risk assessment
form. By task analyzed, risk factors for MSI were
identified, with columns for type of risk factor
identified (e.g. awkward posture, force), frequency
and duration quantities and magnitude and range
quantities (e.g. joint angles, working heights,
weights lifted and push/pull forces).
Risk factor assessment involved a review of work
measurements, comparison with ergonomics
guidelines and standards and compilation of
information from surveys, job observations, and
discussions. When controls were obvious and
effective, this phase was omitted. Refer to Section 3
for more information.
For our LPN example, bed repositioning was listed
as a sub-task. MSI incident analysis information
showed that injuries occurred during this activity.
Risk factors identified during job observations
included awkward posture (of the shoulder, elbow
and back), static posture and force. It was also noted
and reported by staff that this was a difficult task
and current training on patient transfer techniques
was required, especially when completing a manual
transfer with a partner.
For the assessment phase, joint ranges were specified
using RULA (Rapid Upper Limb Assessment, see
reference list) worksheets. Forces for bed
repositioning were not measured (it was deemed not
practical to obtain valid measurements). Comments
from staff, work processes and other deficiencies
were noted.
5.4
Risk Factor Control
This final phase involved the development of risk
controls. Risk controls were proposed for those risk
factors as identified through assessment, which
presented a greater risk to the employee.
For repositioning in bed, risk factors identified were
awkward posture, static posture and force. The
proposed controls included staff training sessions
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
31
with practical demonstrations (already in place),
communication on key tips for optimizing postures
(such as adjusting bed heights, lowering the side rails,
and asking patients to assist) and conducting trials
with sliding sheets (slippery fabric to reduce friction
and reduce the forces required when moving patient
in bed).
An important part of the entire process was to
ensure agreement with the recommendations. The
report with recommendations was prepared in draft
and reviewed with the nurse manager prior to
issuing. Appropriate revisions were made in order
to ensure that identified risk factors were addressed
with appropriate controls that would be
implemented. The final report was issued and
findings communicated to staff via the nurse
manager.
5.5
Follow-up on Recommendations
For the purposes of tracking and follow-up in the
database, each recommended control is linked back
to a risk factor and task. Each control is coded as to
its type (e.g. training, capital purchase, work
procedure) with status and date fields. Continued
follow-up reports on the recommendations will be
generated by the database to determine current status
of those recommendations.
For the final LPN report, the current status of the
recommendations is as follows. Seven (7)
recommendations were made of which 6 were
related to patient handling. It was recommended
that all staff continue to be scheduled for the on-
site patient handling course, information on
stretching exercises be provided, awareness
campaigns on topics relevant to patient handling
(e.g. correct use of transfer belt, bed repositioning
tips etc.) be initiated, and trials with sliding sheets
be conducted. In addition, it was recommended
that existing commodes be either repaired or
replaced (brakes were faulty), night tables be
equipped with casters for ease of movement and
that staff continue to have input and trial sessions
with new equipment purchases such as beds (there
was a task team for new bed purchases, with staff
input).
On follow-up three months after report was issued,
the following actions had been initiated:
A short presentation on MSIs was completed
with department staff. The material was dev-
eloped as part of a site-wide awareness cam-
paign and included a pamphlet and newsletter
article. Future campaigns are planned for
various topics including stretching, using a
transfer belt, and key tips for patient
handling. In addition, the MSIP Minute
bulletin was launched by the MSIPP
Committee.
Staff are attending the 4-hour patient handling
course. Finding replacement staff is difficult
and many have to attend the course on their
days off. With 2 sessions per month, the hope
is that all staff will have completed the
training by the summer.
Two types of sliding sheets (low-friction to
assist with bed repositioning) are available
for trials on the ward with the assistance of
a physiotherapist.
New commodes are now on the unit.
Follow-up on outstanding recommendations will
continue with a written report generated from the
database approximately every 3 months.
5.6
Consultation and Communication During
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
32
Risk Assessments
As per WCB Ergonomics (MSI) Requirements and
in keeping with the participatory nature of the
project, consultation was sought at various stages
of the project, primarily from the steering
committee and joint occupational safety and health
committee (JOSH) on site. It was often stated that
project processes and tools were works in
progress, and feedback was welcomed.
Various communication vehicles and avenues for
input were provided to staff at the facility including
senior administration, managers, MSIP committee
members and workers in the departments where risk
assessments were performed. Throughout the project
there were ongoing efforts to continually consult and
communicate with staff including key steps, case
studies and progress updates.
Examples of consultation and communication with
staff:
General project information: one page sum-
mary and 4-page detailed report was reviewed
with Steering Committee and JOSH, then
distributed and posted in departments as
appropriate.
Initial project plan and timeline was reviewed
with Steering Committee andJOSH Com-
mittee and communicated to staff via a series
of presentations.
Draft and final MSI incident analysis report
including findings and weighting scheme for
prioritization was reviewed with Steering
Committee and JOSH Committee. Sum-
mary MSI incident analysis report was
presented and distributed to managers.
Format of the department specific MSI
incident report was reviewed with Steering
Committee and JOSH Committee. Sample
reports were provided. Final reports were
distributed to managers.
Process for the conduct of risk assessments
and the final report format were reviewed
with Steering Committee and JOSH
Committee. Final process was commun-
icated to staff via presentations.
Checklists developed for risk identification/
risk assessment were reviewed with Steering
Committee and JOSH Committee.
Progress reports on a monthly basis, often
with presentations, were provided to Steering
Committee and JOSH Committee.
Additional project updates and presentations
were conducted with LMH Senior Adminis-
tration Team, Management group, MSIP
committee, and regional health and safety
committees approximately every 2-3
months.
Short presentations about the project were
held at department meetings, by invitation,
including providing an overview of the
project as well as reporting on the findings
of the assessment.
An Open House was set up in June 2002
to display information including MSI
statistics, handouts and example controls,
both existing and implemented.
5.7
Challenges encountered
The following challenges were encountered in
applying the process:
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
33
Time constraints: In addition to noted time
constraints on the part of the ergonomist to
simply complete the risk assessments, there
were noted time constraints on the part of
many other staff members with whom were
encountered in completing this project. It
was sometimes difficult to meet with staff
in a timely manner, for example, to discuss
issues or concerns, to fill out a survey, or meet
to discuss the reports.
Financial considerations: In many, many
cases, the risk factors for MSI had previously
been identified, with appropriate recommen-
dations having already been made for risk
control. However, implementation was either
delayed or not completed due to lack of fund-
ing. Competing priorities for areas other than
ergonomics (such as direct patient care) are
sometimes formidable obstacles! In some
cases, having the risk assessment conducted
provided additional impetus for changes to
take place or simply provided more informa-
tion as to the nature and extent of the risks
for MSI.
Lack of resources: Somewhat related to the
above, there often seemed to be a lack of
resources to assist with the implementation
of some of the recommendations, either
human resources, equipment or funding. For
example, where training strategies had been
recommended, initiated or already imple-
mented, there was often a reported lack of
resources to develop the materials, conduct
the training, provide staff to backfill for atten-
dance at training, or provide funding for any
of the above.
Unpredictability of patient handling: With
patient handling, there are many factors
which make each situation unique and
potentially unpredictable. Mental and/or
physical illness may render the patient
uncooperative or unpredictable making the
handling situation a potential risk for injury.
Even with appropriate policies, training and
work practices in place, it sometimes seem-
ed that accidents and injuries could still
occur if the unexpected were to happen.
Workplace factors: During the course of the
project, we experienced job action due to
ongoing contract disputes with both the
unions and physicians, as well as a major
amalgamation of health regions in the
province. Although not directly affecting
outcomes and timelines, it sometimes posed
difficulties in determining appropriate times
for activities such as surveys and job
observations, as well as appropriate people
to discuss changes and recommendations
with.
5.8
Positive notes
Overall, the project implementation went very well.
All staff members were very helpful and supportive
of the process, information collection phases and
implementation of the recommendations. A special
thanks goes out to all department managers for
seeing this project to fruition within each of their
individual and unique working environments! Their
patience, assistance, professionalism and support of
this project were very much appreciated throughout.
Their ongoing efforts and dedication to making
improvements in the workplace to reduce MSIs
should be rewarded.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
34
6.0
GENERAL FINDINGS
AND RECOMMENDATIONS
6.1
Introduction
This section outlines key program elements for the
prevention of musculoskeletal injuries, as well as
general findings and recommendations within the
facility as a whole. Points listed are specific to the
ergonomics risk assessment process only.
6.2
Recommended program elements for
MSI prevention
After conducting a brief review of literature, the
following list of key program elements for MSI
prevention is provided with notes on general findings
at LMH. The WCBs 7-step process (based on the
WCBs Ergonomics (MSI) Requirements) for MSI
prevention is also contained (as bolded) within these
program elements. Appendix C-8, page xxvii
contains General Ergonomics Risk Factor
Checklist designed to assist in the identification of
these elements.
6.2.1
Policies and procedures
The employer should have in place policies and
procedures for MSI prevention. The (former) South
Fraser Health Region Workplace Health and Safety
policy can be found in Appendix E, page xxxvii.
In addition, a Memorandum of Understanding
(MOU) between the Association of Unions and
Health Employers Association of B.C. (HEABC)
was signed in March 2001. The MOU (available from
Occupational Health and Safety Agency for
Healthcare in B.C. OHSAH) states that both parties
agree to establish a goal of eliminating all unsafe
manual lifting of patients/residents through the use
of mechanical equipment. (Outside of British
Columbia, there are also other examples of policies such
as The Royal College of Nursing (UK) Code of Practice
for Patient Handling).
Patient Handling Policies and Procedures have also
been established within the (former) South Fraser
Health Region. Specific patient handling procedures
were developed over a year long process which
brought together a task force of Physiotherapists,
Occupational Therapists and Workplace Health
Advisors from the 4 main sites which made up the
former health region. Many meetings were held to
discuss, debate and develop safe patient handling
procedures based on current information and
practice. Many members of this task force that
created the procedure manual are regular trainers for
the MSIP Patient Handling sessions at their sites.
The new training program based on the policy and
procedure manual was rolled out in 2001 and is
ongoing to date. The task force still meets, and they
are able to bring employee feedback to the group for
consultation and future revisions as required to meet
the changing needs and evolving science of patient
handling.
The current health authority is moving towards a
No Manual Lift Policy, as was the former health
region with which this project was initiated (see
Appendix E, page xxxviii). Key to the establishment
of the policy is having resources in place to support
it. A no-lift policy will only work if there are also
procedures, equipment, systems of work, training
and consultation processes with employees in place.
The infrastructure is now in place to support a No
Manual Lift Policy at LMH and future
communication to staff should reflect that.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
35
6.2.2
Consultation processes
Consultative channels via workplace committees
should be in place for employees to provide input
and feedback into MSIP strategies.
Over the course of this project, the joint union-
management steering committee continued to guide
progress and process, as well as providing input and
assistance during all project phases. Regular
meetings and regular communication by e-mail were
carried out. In addition, the Regional Occupational
Safety and Health Committee (ROSH), site Joint
Occupational Safety and Health Committee (JOSH)
and LMH MSIP Program Committee were updated
regularly (monthly or bi-monthly depending on
meeting schedules) on the projects progress, as well
as being provided opportunities for input and
feedback. Communication to LMH staff through
presentations at Senior Leadership meetings,
management forums and department meetings and
e-mail updates were also completed.
An initial project overview was provided to
Workplace Safety and Wellness Advisors, WCB
Field Officers and other site JOSH committees (e.g.
Surrey Memorial Hospital, Peace Arch Hospital) as
well as to regional Executives.
The JOSH and MSIP Program Committees will
continue to provide an important avenue for MSIP
information at LMH and to address any concerns
or issues reported from staff. At the management
level, a regular monthly update meeting with
managers will continue to provide a forum for
presenting information and discussing employee
concerns after the completion of this project.
6.2.3
Education and Training strategy
It is important that an education and training
strategy be in place for MSI prevention. Time should
be allocated for both general and job-specific training
at time of orientation to the job, as well as various
refresher and in-service training on various topics
on an ongoing basis as determined necessary by the
topic.
The training plan of the (former) South Fraser Health
Region will need to be reviewed and amalgamated
as a result of health authority reorganization. The
current training strategy involves general MSIP
information (signs and symptoms, risk factors) as
well as specific MSIP components for:
Patient Handling,
Material Handling,
Office Ergonomics, and
Management of Aggressive Behaviour
Training (available through the Protection
Services department).
Separate training sessions are available regionally for
both MSIP Patient Handling and Management of
Aggressive Behaviour. Training on MSIP Non-
Patient Handling (i.e. Manual Material Handling and
Office Ergonomics) is available through the regions
orientation program and for new employees in a
session from the Occupational Therapy Department
at LMH. General information on all topics is
available in handouts, postings on intranet and by
request through the Workplace Safety and Wellness
department.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
36
6.2.3.1
Additional points specific to the patient
handling procedures and training at
LMH:
The 4-hour training sessions teach skills in a
variety of patient handling techniques. The
procedures are based on the principles of
good body mechanics to minimize force and
exertion to both the caregiver and the
patient/resident. All procedures are docu-
mented in an MSIP Program manual, which
is available in all patient care areas of LMH.
The training and procedure manual includes
information on general body mechanics.
The training and procedure manual includes
information for caregivers to pre-assess
patients abilities to assist or cooperate prior
to the handling process.
The training emphasizes an approach where
the caregiver can determine before each transfer
whether to proceed and feel comfortable in
not doing so if they determine it is unsafe.
The training reviews the process for initial
patient/resident mobility assessments, and
the process for requesting an initial
assessment or reassessment.
The training includes opportunities for
demonstration and practice in a classroom
setting, including hands on practice using
mechanical aids and assist devices including
transfer belts.
Key point tipping is provided by the instruc-
tors as they observe participants.
The training includes sign-off of demostrated
competency of participants.
6.2.3.2
Additional points specific to training for
management of aggressive behaviour:
Evidence of MSIs due to violent, aggressive acts by
patients and residents was found in incident reports,
employee surveys and in discussions with staff.
Injuries often are the result of unpredictable and/or
aggressive behaviours on the part of the patient/
resident. Training on Management of Aggressive
Behaviour (MOAB) is available at LMH through a
regional training program and staff members are
being scheduled for attendance. The MOAB training
sessions are available for moderate risk groups, high
risk departments (sessions include a clinical portion)
as well as a session for violence code (code white)
team members.
6.2.3.3
Additional points specific to training for
manual material handling and office
ergonomics:
General information on material handling and
office ergonomics, including correct lifting
techniques, use of lifting equipment and computer
workstation set-up is available to employees at the
time of orientation. In addition at LMH, new
employees can be scheduled to attend a 2-hour job
specific training session presented by the
Occupational Therapy department. Additional
information on both topics can be found in various
handout materials, in training sessions as requested
and on the intranet site.
There will be a policy and procedure manual
developed for non-patient handling areas to address
risk factors for MSI in the other areas of healthcare
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
37
Staff should continue to be educated in the correct
form to use for the purpose of reporting incidents
and injuries, how and what to document, who
should be involved in the investigation and what
happens to the information that is provided on the
form. This will ensure the early and accurate
completion of incident information.
Risk assessment
Workplace Health Advisors currently conduct risk
assessment on site as required, with some formal
processes in place including analysis of incident data
and a standard form for reporting findings. Based
on the findings of and tools developed for this project
and using statistics generated from the incident
database, there will be a component of risk
assessment built into the overall ergonomics program
for the health authority. High risk areas will be
prioritized for risk assessment, and information and
education relative to MSI prevention to all areas will
be provided on an ongoing basis.
Risk control
The development of risk controls is dependent on
the process by which the risk factors have been
identified. Risk controls for MSI prevention will
include education and training; equipment, tools and
work area design and redesign, job redesign/change
in work processes; and documentation and
communication of safe work practices.
6.2.5
Evaluation, promotion, monitoring and
review of programs
Key to any program is the continuous monitoring
and evaluation of measures taken to address MSI
to ensure that they are effective.
Section 8 of this report describes outcomes of this
project based on the evaluation of some parameters,
that do not involve direct patient care such as
housekeeping, laundry, stores and food/nutrition,
as well as material handling in all areas including
patient care areas.
6.2.4
Hazard identification and risk control
strategies
Hazard identification strategies should include
incident reporting, risk identification and risk
assessment, accident investigation and analysis of
injury statistics. It is important to have a system in
place to encourage reporting and documenting of
injuries and incidents, including near misses and early
signs and symptoms. The reporting system in place
should encourage staff to report incidents, ranging
from near misses to lost time; involve some level of
evaluation as to the causes; provide means for
investigation of root causes so that appropriate
controls that can be implemented; and provide means
for the information to go into a database for
establishing trends and calculating statistics.
Injury/incident reporting system
The injury/incident reporting system in place at
LMH uses a form 590 which allows the
documentation of an investigation process from
the reporting of incident details to hazard
identification and recommendation of controls. All
information is coded and entered into a regional
database. The employee or manager initiates the
form and it is recommended that the investigation
be conducted with the employees input and
involvement as much as possible. The Workplace
Health Advisors conduct follow-up on the
investigation strategies and implementation of
controls. Some departments are also having staff
conduct reviews and follow-ups of the reports, to
ensure appropriate recommendations are being made
and implemented to prevent recurrence.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
38
as well as future direction based on the findings
and recommendations of this project.
Monitoring and evaluation of the risk assessment
process and program should continue through
analysis of incident/injury statistics, channels for
staff feedback, and evaluation of controls
implemented including cost/benefit analysis.
Promotion of prevention information can be
conducted through regular staff bulletins or
newsletters, intranet postings, presentations,
announcements at meetings or other communication
vehicles.
6.3
Facility-wide Findings of the Risk
Assessments
The following outlines general findings from the
risk assessment project that are relevant to the
facility as a whole:
Management support and involvement,
accountability and commitment are
important for all aspects of work, including
occupational safety and health programs. It
is important that support be spoken about
and acted on by example, promotion (e.g.
highlighted on meeting agendas), as well as
through funding (e.g. for training and for
purchasing appropriate and sufficient
equipment for safe work practices). Without
the support, guidance and assistance provided
from the various levels of administration at
LMH, this project would not have achieved
any of its successes.
Effective communication is indeed a two way
street and can also be a highly effective inter-
vention tool! It was often demonstrated how
open lines of communication can lead to
improvements to work systems and the work
environment often with little or no money
being spent. Many minute changes were
accomplished right on-the-spot during the job
observations (e.g., getting an appropriate cart,
moving a piece of equipment, raising a
monitor, finding out how equipment works)
through appropriate communication.
Allowing staff a forum for identifying
concerns and issues and working together to
solve them in the most efficient and effective
manner has benefits not only for health and
safety but other areas such as performance,
job satisfaction and morale.
Workload and its impact on an aging work-
force were often cited by front line staff as
contributors to MSI. Staff often expressed
that they feel rushed and stressed to complete
their tasks. They stated that they are aware
of the correct and safe procedures and
equipment to use, but often dont feel that
they have the time to do it the right way (e.g.
retrieve mechanical equipment, find a
transfer belt, ask for assistance from other
staff, adjust the bed height, lower the side
rails). Widely accepted guidelines in the
healthcare industry for the measurement of
workload are not available and it was very
difficult in context of this project to
objectively measure workload. It is hoped
that the future will provide more information
relevant to workload including patient/staff
ratios and measures of patient acuity. In
addition, it is hoped that other ongoing
changes that are taking place will have a
positive impact on workload (e.g. installation
of ceiling lifts).
Equipment that is in good working order
is essential. Poorly functioning equipment or
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
39
equipment that is out of order requires more
manual effort, which may increase the risk
of injury to caregivers and patients. Regular
preventive maintenance checks as well as on
going repair of equipment, specifically rolling
stock or wheeled equipment such as
mechanical lifts for patients and residents,
beds, trolleys, carts and wheelchairs are an
important part of an MSI prevention strategy.
Regular equipment maintenance may also
prolong the life of the equipment and save
on subsequent repair bills. It is important to
have a good system in place for the reporting
of equipment that is in need of repair and it
is important to ensure that all staff are aware
of the procedure and complete maintenance
requisitions when required.
Appropriate and adequate equipment
with features that are usable and used by staff
members is essential, e.g. beds, carts and
trolleys, wheelchairs and geri-chairs, medica-
tion carts, furniture with casters that is easy
to move. It is important that managers are
up-to-date on equipment that is currently
marketed and that appropriate funds are
allocated to allow for the purchase and main-
tenance of equipment. Having preferred
products and purchasing standards is benefi-
cial for reducing staff time to find appropriate
items, as well as potentially reducing costs.
Trialling equipment prior to purchasing (to
ensure that the item is suitable for the specific
setting in which it will be used) is beneficial
for gaining staff input and ensuring maximum
benefit from dollars spent. Involving all
stakeholders in the purchasing decision such
as Maintenance, Workplace Safety, House-
keeping and Purchasing is also important.
Building design and layout with adequate
space to move, use and store equipment
are important elements for MSI prevention.
In many cases, building design was cited as a
risk factor for MSI, especially in patient
rooms but in many other areas throughout
the hospital as well. Problems frequently
cited included lack of space to work (e.g.
areas under desks being used for storage, not
enough space to use patient handling
equipment at the bedside, having computers
on counters with little room for keyboarding),
general clutter due to amount of items in
room (e.g. chair, bed table, night table,
garbage can) or in hall (e.g. mechanical lifts,
laundry bins, wheelchairs), lack of space for
storage, problems due to bathroom doors
being too narrow for walkers or wheelchairs,
cluttered or non-direct routes for transporting
patients, or inappropriate flooring. Building
design should be conducive to safe work
practices. Recently renovated or newer areas
of the facility do go through a process
including design review and staff input to
ensure more user-friendly aspects. It is im-
portant to ensure that staff and patient
needs and uses continue to be considered in
all designs and that the end users continue
to be involved to ensure facilities will meet
their needs and minimize the risk of MSI.
6.4
Facility-wide recommendations for MSI
prevention based on general findings
from the risk assessments
Based on the above key elements and general
points, the following recommendations are made
for consideration facility-wide.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
40
The site administrator will be responsible for
ensuring that appropriate personnel within the
organization address these recommendations.
6.4.1
Communicate the no manual lift policy
to staff at LMH
The current health authority has a No Manual Lift
Policy documented (from the former health region
with which this project was initiated, see Appendix
E, page xxxviii).
The infrastructure (e.g. MSIP patient handling
procedures, MSIP patient handling training,
mechanical equipment, consultative processes with
staff) is now in place to support a No Manual Lift
Policy at LMH.
Recommendation: It is recommended that future
communication take place at the facility to promote
and enforce the No Manual Lift policy.
Responsible: Director of Workplace Safety and
Wellness
6.4.2
Staff should continue to be educated in
the correct form to use for the purpose
of reporting and investigating incidents
and injuries
The health region has established that all reported
incidents and injuries including near miss, first aid,
medical aid, lost time or no lost time should be
reported using the Form 590. This is an important
hazard identification strategy for the region as a
whole as well as individual facilities. As much as
feasible, it is recommended that employees involved
in the incident are included in the investigation
process.
Recommendation: There should be ongoing
communication and promotion around the use of
the incident/injury (590) form. Staff should
continue to be educated in the correct form to use
for the purpose of reporting incidents and injuries,
how and what to document, who should be
involved in the investigation and what happens to
the information that is provided on the form.
Responsible: Director of Workplace Safety and
Wellness
6.4.3
Consider area(s) designed specifically
for storage
As in many healthcare facilities, storage space at
LMH is at a premium. Lack of storage space may
contribute to clutter and storage of equipment in
inappropriate places such as hallways, shower rooms
or any empty spaces.
Recommendation: Consider areas within the facility
to serve as safe and secure storage areas for
equipment such as mechanical lifts, pumps, IV poles,
chairs, and wheelchairs.
Responsible: Site Administrator, LMH
6.4.4
Formalize preventive maintenance
program for rolling stock
Individual departments within LMH have an annual
budget amount designated for maintenance of
equipment, including repairs and preventive
maintenance. Priorities for preventive maintenance
and repair of wheeled equipment may be hard to set
due to ongoing requirements and requests for other
maintenance work, availability of manpower to do
the repairs and checks, department budgeting
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
41
concerns (who will pay if the budget has run out?)
and lack of replacement equipment. A maintenance
program for rolling stock has been proposed in the
past, with an inventory listing and associated costs
having been submitted for approval.
Recommendation: Consider formalizing a repair and
preventive maintenance program for rolling stock
using an inventory listing of rolling stock on site
including patient handling equipment, determining
specifically the rolling stock that it is critical to
maintain, and establishing a budget, including
manpower, to develop and maintain the program.
Responsible: Director of Engineering and
Maintenance
6.4.5
Continue to consider staff health and
safety needs in the capital equipment
selection process
During the capital equipment selection process, one
of the criteria that is used in prioritizing is staff health
and safety needs. This is important both at the stage
where funds are allocated as well as when the specific
items are selected.
Recommendation: During the capital equipment
selection process, ensure that one of the criteria used
in the selection process is for staff health and safety
needs.
Responsible: Site Administrator, LMH
6.4.6
Establish purchasing standards for
ergonomic equipment and encourage
trials with new equipment
Equipment with features that are usable and used is
essential. Having preferred products and purchasing
standards is beneficial for reducing staff time to find
appropriate items by providing various options with
preferred pricing and vendor information. Involving
all stakeholders in the purchasing decision such as
Maintenance, Workplace Safety, Housekeeping and
Purchasing is also important for ensuring items are
safe and effective and all budgeted requirements have
been accounted for. Having equipment trials prior
to purchase will help to ensure the item will be
suitable in the specific setting in which it will be
used.
Recommendation: Workplace Safety and Wellness
Department to work with Purchasing Department
to establish a preferred/suggested listing of items
and/or vendors as per ergonomics guidelines e.g.
computer workstation equipment, headsets, pill
crushers, medication carts etc.
Responsible: Director of Workplace Safety and
Wellness
6.4.7
Maintain effective communication
channels
The importance of communication was quite
apparent throughout this project. In many cases,
ergonomic recommendations were not required; only
appropriate communication! At times, employees
were not always aware of the positive changes that
were in the process of being implemented, instead
they reacted to change. Relaying to staff about
appropriate processes or procedures, outlining who
they need to talk to, or relaying information about
positive changes taking place in other areas of the
facility would be beneficial.
Recommendation: Continue to look for ways of
frequently and effectively communicating with staff
about positive changes at LMH to help promote a
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
42
continued positive attitude in the workplace. This
may be through a bulletin being circulated or e-
mailed to staff or through a newsletter. Changes
could be related to topics beyond health and safety.
Responsible: Site Administrator, LMH to consider
appropriate options
6.4.8
Provide MSIP prevention information
on an ongoing basis and through various commun-
ication vehicles, including safe work procedures
and newsletters. MSIP prevention strategies,
specific to job tasks or issues, may be beneficial as
a means of communicating safe work practices to
staff and continuing to find ways to remind
employees about how to avoid injury.
Recommendation: Provide MSIP prevention
information and safe work procedures on an ongoing
basis through staff bulletins and newsletters, intranet
postings and e-mails. Communicate to appropriate
departments based on the topic. The MSIP Minute
MSI prevention bulletin has already been launched
by the MSIP committee. The bulletin will cover a
variety of MSIP topics and will be issued
approximately every 2 months.
Responsible: Director of Workplace Safety and
Wellness
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
43
7.0
DEPARTMENT-SPECIFIC
FINDINGS AND
RECOMMENDATIONS
7.1
Introduction
An overview of department-specific findings and
recommendations is provided below, including points
on controls that were already in place prior to the
risk assessments being conducted. The intent is to
summarize the major findings by work area to
provide information and ideas on potential controls
that can be implemented for MSI prevention.
Example worksheets and checklists used can be
found in Appendix C-7 to C-11, page xxvi-xxxi. For
communication and follow-up within LMH, the
managers received a risk assessment report (format
as Appendix C-6, page xx-xxv) for each occupation
within their departments that underwent assessment.
For more information on the occupation-specific risk
assessments reports completed (120 reports), please
contact the Workplace Safety and Wellness
Department of the Fraser Health Authority.
When documenting the recommendations for the
individual assessments, there was an attempt to
provide a holistic approach to prevention in that
typically each report has a variety of
recommendations including training and
information, safe work procedures and processes and
recommended purchases of capital items. The intent
is that training/information that is not yet in place
will be developed, job specific techniques and work
practices will be documented and distributed to staff
and capital items (tools, equipment, redesign) will
be considered for subsequent budgets.
For many work areas, it was recommended that
information on job specific stretching exercises and
safe work practices be provided. This will be
developed as part of the ergonomics program
initiatives in the future for distribution across the
health authority. During the course of the project,
LMH staff members were provided with general
information on MSI signs and symptoms, risk
factors, and general strategies for preventing injury
via pamphlets, posters, displays, intranet postings and
presentations.
7.2
Admitting including Bed Control and
Switchboard
Seating, layout and set up of computer workstations
Computer workstations are equipped with
adjustable chairs and adjustable keyboard
p l a t f o r ms .
Identified risk
factors for MSI
i n c l u d e d
a w k w a r d
postures and
static postures
associated with
computer work
(e.g. not adjusting chair or adjusting keyboard to
incorrect height; monitor at improper height, lack
of stretch pauses, and not alternating duties in order
to incorporate a change in posture). Additional
findings included incorrect placement of the mouse
(was placed on the desktop instead of on the
platform beside the keyboard). Recommendations
included on-site changes and tips as well as
providing written information on correct set-up of
the computer workstation as per ergonomics
guidelines. Correct arm positioning and placement
of the mouse and stretching exercises were
emphasized.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
44
Using phone and computer
Cradling the phone between the ear and shoulder
was observed as a risk factor for MSI due to awkward
neck and shoulder positioning. The existing headsets
which were not used due to problems with static and
comfort were replaced with cordless headsets which
received positive feedback from staff and are used.
7.3
Critical Care Unit
Monitoring and assessing patients, including moving
equipment and beds
Identified risk factors for MSI included awkward
postures, static postures and forces associated with
general duties for monitoring and assessing patients
(e.g. taking
vitals, visual
assessment ).
M S I
p r e v e n t i o n
i nf or mat i on
specific to
CCU is to be
p r o v i d e d .
Additional risk factors were identified due to
requirements to move monitors at the bedside or
within the unit, as well as beds (primarily from bay
to bay but sometimes to other areas of the facility)
and other equipment. The bedside monitors were
already mounted on articulating arms and the
operating mechanism was adjusted to reduce the
forces required to move the monitors in the vertical
direction. New beds that are lighter and easier to
move have been on the capital funding list, as is a
newer, more compact portable cardiac monitor.
Staff was requested to use proper work techniques
when moving beds (e.g. unlock wheels, check wheel
orientation, adjust height for appropriate handhold,
ask for assistance) and ensure wheels are in proper
working order, or request maintenance on them if
needed. Carts for handling the small oxygen tanks
are provided to eliminate the requirement to carry
the tanks.
Patient handling incl-uding repositioning in bed
For patient handling, transfer (slider) boards and
transfer belts are available for use. Additional
mechanical lift equipment is also available as
required from nearby units. It was recommended
that staff continue to be scheduled for MSIP
patient handling training (ongoing), special beds
continue to be ordered and used as necessary, and
trials with sliding sheets (for reducing forces when
repositioning patients in bed) be coordinated
through Physiotherapy department.
7.4
Diagnostic Imaging
Clerical workstations including storage and handling of
films
Clerical workstations for booking appointments are
equipped with adjustable workstations including
chairs, keyboard platforms and footrests.
Information on how to adjust, including example
stretching exercises was provided to staff. Anti-
fatigue matting was trialed at the film desk where
films are labelled and packaged. The cabinets
housing the films are periodically reorganized (with
archiving) so that the films are spread out amongst
available shelves. This ensures films are not packed
too tightly on one shelf and helps to reduce forces
when taking films in and out. Staff was also
reminded to minimize the number of films carried
at once and the number of cabinets moved at once.
Step stools are provided for accessing higher shelves
and to use as a seat when accessing lower shelves.
Completing diagnostic procedures
When completing diagnostic procedures such as
mammography, ultrasound and radiology exams,
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
45
risk factors
of awkward
p o s t u r e ,
s t a t i c
posture and
force were
i dent i f i ed.
Adjustments
can be made
throughout
the procedure so that the technologist remains as
close to a balanced, upright position with neutral
joint postures as much as possible for example, by
asking the patient to move closer, adjusting the
stretcher the patient is on, adjusting the position
of the diagnostic equipment, adjusting the chair,
changing from a seated to a standing position,
moving to the other side of the patient, alternating
hands used, changing the position of the patient or
changing the room (may be best suited to one side
or the other). Staff is to be provided with
information on the importance of muscle mini-
pauses, as well as appropriate job specific stretches
to do. Newer equipment (LMH has a new
Ma mmog r a p hy
machine and a new
CT Scan) has more
a d j u s t a b i l i t y
features that are
easier to operate
(small range of
motion and
minimal forces
required to make
adjustments). It is
hoped that newer
equipment will provide better quality images (to
reduce forces required) and better ergonomic
design for the users to allow for maximum
adjustability and flexibility in positioning.
Handling and storage of cassettes
Risk factors of awkward posture and forces were
identified when handling cassettes. Muscular effort
when handling cassettes can be minimized by
selecting the smallest size possible, keeping
frequently used cassettes in storage shelves at the
optimal height (to minimize bending and reaching),
and always handling and carrying cassettes with 2
hands to spread out effort to both arms.
Above shoulder positioning when setting up equipment
Information on stretching and strengthening
exercises relevant to job specific tasks is to be
provided. Staff was encouraged to keep tasks below
shoulder level as much as possible e.g. work
method when setting up the X-ray machine can be
altered so that the machine is lowered and moved
laterally into position then set back up to the
appropriate height.
Wearing lead aprons
Aprons with waist
belts (to transfer some
of the load) are
available and should
be used as much as
possible. Suggested
method for putting on
lead apron is to shrug
shoulders prior to
fastening on hips to
reduce direct loading
on the shoulders. In addition, it was suggested that
the aprons be removed in between exams as much
as possible to minimize muscular effort.
Patient handling including pre-transfer assessment
To minimize risk factors associated with patient
handling, various patient handling devices
including a mechanical lift, transfer boards and
transfer belts are available. Staff are requested to
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
46
previously scheduled. Input was provided to
improve identified risk factors for MSI. The counter
width was reduced so the RN had easier access
and less reaching to the patient for the conduct of
physical assessment. Consideration was made to
the overall layout to improve visibility, accessibility
for wheelchairs and stretchers, and ease of
movement behind the triage desk. In addition, the
setup of computer work-stations was improved
using adjustable keyboard trays and flat screen
monitors for ease and flexibility of adjustment.
7.6
Extended Care Units
General tasks
Identified risk factors for MSI included awkward
posture, static posture and force associated with
various tasks. General information on correct body
mechanics, stretching and job specific work
procedures (e.g. dressing resident, handling laundry
bags, making beds, handling stock) is to be
developed. Pre-shift stretching posters are already
posted on the units.
Resident handling process and procedure
Staff will continue to be
scheduled on MSIP
patient handling train-
ing. This training
reviews tips for resident
assessment prior to
handling. The training
also includes demon-
strations and practice
on various techniques
including the use of
mechanical equipment. Competency measures for
attendees are included in the training. It was
recommended that staff be reminded of the
process for resident mobility in that residents are
ask the patients to move themselves and assist as
much as possible and to ask for assistance from
other staff members if required. Information on
pre-transfer assessment was provided as a means
of reducing incidents associated with patients
unexpectedly falling or fainting.
7.5
Emergency
Patient handling including transferring patients out of
cars
Patient handling equipment including transfer
boards and transfer belts are available for use. Staff
will continue to be scheduled for MSIP training. In
addition, information on specific devices available
for transfer out of cars will be provided.
Moving equipment and material handling
Identified risk factors for MSI included awkward
postures and force associated with moving
equipment in tight or cluttered spaces, accessing
files and accessing bedside monitors. Future design
considerations suggesting more space and layout
for patient
movement
w e r e
provided. A
new, more
c o mp a c t
p o r t a b l e
c a r d i a c
m o n i t o r
was purchased. Recommendations were also made
for improving access to cardiac monitors at the
bedside and accessing files (relocating the drawer
to reduce bending).
ER Triage
During the risk assessment project, the ER Triage
area underwent renovations that had been
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
47
assessed for mobility by Physiotherapy upon intake,
the designated transfer is documented with
appropriate logo and information on ADL at
bedside, and more detailed care plan is accessible
to staff at nursing station. Requests for residents
to be reassessed for mobility can be recorded in
the Rehab Communication Log in ECUs
(clipboard with form sheet that is reviewed and
acted on daily by Rehab staff members).
Resident handling equipment
Electrical mechanical
resident handling
equipment is avai-
lable in each of the
extended care units.
Trials with various
types of sliding sheets
to determine appro-
priate uses by task
and by resident are
u n d e r w a y .
Consideration for more resident handling
equipment including mechanical lifts, slings and
ceiling lifts was recommended. As part of a
provincial government funding initiative, ceiling
lifts have been installed at one of the units. Three
new mechanical lifts were also recently purchased
through the capital funding program.
Requests for maintenance and repair of equipment
It was recommended that staff be reminded of the
process for requesting repairs to Maintenance
department to ensure all staff are aware of and use
the procedure.
Dispensing medications
Risk factors such as awkward posture and force
were identified with pill crushing, popping pills from
blister packs, moving medication carts and reaching
and bending to access residents. MSI prevention
information on dispensing medications is to be
provided including suggestions for storage (most
frequently used items should be placed in best
storage positions), adjusting resident in bed to
improve positioning, using a blunt object such as
an eraser to pop pills from blister pack or alternate
fingers used, and dispensing in bottle or liquid where
possible. In addition, recommendations for new
medication carts were made pending outcomes of
a project at BCIT (British Columbia Institute of
Technology in Burnaby B.C.).
Pill crushing
Pill crushing is another industry wide problem with
no simple solution. A study on pill crushing
prototypes is currently underway at BCIT, of which
the outcomes will be anticipated. For now, various
types of pill crushers were recommended for use
based on staff preferences. Cushioning was
suggested to reduce impact forces. Working heights
close to elbow level were recommended. Work
method suggestions such as minimizing forces
when banging, alternating hands used, only
crushing to level required (may not have to always
crush to a fine powder) and spooning with pudding
were also provided.
Workload
Due to staff concerns with workload, it was
suggested that considerations for minimizing MSIs
and possibly alleviating workload be tied to new
programs for resident assignments (e.g. reexamine
current routines and times for tasks such as bathing
and dressing before breakfast, having staff work in
closer proximity to one another for better access to
each other for assistance as well as mechanical
equipment, equalizing resident assignments by
moving across building wings).
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
48
7.7
Food and Nutrition Services
Working at trayline and dishline
Trayline and dishline positions are rotated at least
daily (some hourly) so that workers are not at the
same station all the time. Consideration is given to
rotation from one side of the line to the other also to
provide for variety of tasks. Anti-fatigue matting is
available at each station. Wagons have dual swiveling
wheels under the handle for ease of turning. Menu
choices are considered to reduce hand actions
associated with portioning (e.g. cutting, spooning,
peeling). Tips for MSI prevention will be developed,
including job specific stretching exercises, notes on
avoiding pushing or holding multiple trays while the
line is moving, setting up station to minimize
awkward postures, and reducing number of items
handled at once. Recommendations were made to
lower the upper shelves (minimize clearance) to
reduce reaching heights.
The dish room had recently undergone renovations
including improvements for MSI prevention. The
height of the carts and work counter are the same
so items can be slid
instead of lifted.
Lowerators (spring
loaded carts)
are avai l abl e t o
minimize bending
and reaching. To
minimize the risk
of slip hazards in
both the kitchen
area and dish room,
absorbents are
used as necessary
and maintenance is
contacted as re-
quired to ensure that drains and sealant are working
effectively. Cotton and paper booties are
mandatory in the dish room. It was recommended
that the hose be supported on a swing arm to allow
the weight to not have to be supported by the
worker.
Food preparation
Identified risk factors for MSI included awkward
posture, static posture and force associated with
preparation of food items such as sandwiches,
nourishments, entrees and frozen food inventory.
Working counter heights are appropriate. Anti-
fatigue matting is available that can be easily moved
for cleaning purposes. An automatic can opener for
opening large cans of fruit and pudding was
recommended.
Receiving, rotating and handling stock
General information on correct body mechanics and
tips for material handling will be provided. Tasks
are rotated so that not all material handling activities
are performed at once and work is self-paced. Storage
shelving has been arranged so that the heaviest, most
awkward and most frequently accessed items are on
middle shelves. Various sizes and types of carts are
available to minimize carry distances. Staff members
have flexibility as to how much to handle, how to
handle it and when to handle it in order to minimize
forces. Additional staff can be called on to assist. A
mechanical minilift is available and frequently
used in the kitchen. The method of delivery of food
to the wards (done daily) was modified so that the
weight of the cart, and therefore forces to push/pull
it, were greatly reduced.
Menu planning and preparation of daily food orders
For office paper work associated with menu planning
and orders, working heights, seating and layout were
reviewed. Information on correct set up of the
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
49
computer workstation and example stretches were
provided. A desk slant for angling reading and
writing material was trialed. As recommended,
offices were equipped with new chairs and
keyboard wrist rests. A new filing cabinet replaced
one with stiff drawers that were hard to open,
especially at the lower levels. It was suggested that
storage and shelving requirements be carefully
considered to ensure that necessary items are easily
accessed.
7.8
Health Records
Seating and set up of computer workstations
Computer workstations are equipped with
adjustable chairs and keyboard platforms.
Identified risk factors
for MSI included
awkward postures and
static postures assoc-
iated with computer
work or having a
combination of paper
and computer work
(e.g. not adjusting or
adjusting incorrectly;
lack of stretch pauses,
and not alternating duties). Various styles of desk
slants are already in use. Recommendations
included onsite changes and work tips including
switching to left-handed mousing (to alleviate
workload to the dominant side). As well, handout
information and a presentation on correct setup of
the computer workstation as per ergonomics
guidelines were provided to staff members.
Storing, retrieving and delivering patient files
For file handling, it was recommended that storage
continue to be reorganized so that shelves are not
overstuffed, the number of cabinets moved at one
time be minimized, and that the carts provided be
utilized for delivery of charts. Step stools are
provided for accessing higher shelves and to use as
a seat when accessing lower shelves. It was
recommended that the practice of having each
employee file and retrieve their own charts continue
to provide a break and change of posture to
minimize static muscle loading.
7.9
Housekeeping
Work organization and planning of tasks
Daily work will continue to be planned and
conducted to minimize risk factors for
mus c ul os ke l e t a l
injury as much as
possible, e.g. staff are
assigned a work area
instead of specific
work tasks, a variety
of tasks are
completed to incor-
porate a change in
posture and musc-
ular effort, shorter
periods of mopping
and buffing are interspersed with other tasks, heavier
tasks are performed closer to the beginning of the
day.
Job specific work procedures
Job specific work procedures with emphasis on
MSI prevention will be developed with staff input.
Procedures will include stretches and tips on correct
body mechanics for tasks such as making beds,
cleaning floors, cleaning bathrooms, handling
laundry bags and emptying garbage.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
50
Moving equipment, furniture and supplies
Information on material handing, correct lifting
techniques and correct body mechanics is to be
provided. New equipment purchased is standard
housekeeping equipment that is trialed with staff
prior to implementation. Items are stored in various
work areas throughout the facility such that those
that are most frequently accessed or heaviest are in
the best positions for ease of handling. When moving
furniture, various types of assistive equipment such
as carts and dollies are available. Additional staff
can be called on for assistance. Large biohazardous
bins have now been replaced with smaller boxes with
a weight limit. Modifications to a ramp used to move
bins to the garbage hopper were recommended
(make the ramp longer with less of a slope).
7.10
Laboratory
Operating laboratory testing equipment
Various types of equipment including computers
are used in laboratory analyses. Time at any one
workstation is limited through staff rotation and
the need to perform other duties in the laboratory.
Examples of MSI prevention strategies already in
place in the laboratory include anti-fatigue matting
at some of the testing equipment; workstations
with the option to sit or stand (task chair with foot
ring available at counter set for standing); and
automatic pipettes.
General laboratory ergonomics information
including correct positioning at the computer, the
importance of mini-pauses and stretching,
making frequent adjustments to equipment,
keeping materials in close, and other tips for
specific tasks (e.g. working at microscope, working
at biological safety cabinet, drawing blood from
infants in incubators) will be provided at a staff
meeting.
Computer workstations
Computer workstations are present throughout the
laboratory, with different set ups and varying
adjustability features. Workstations are designed
for either seated or standing postures. Computer
set-ups were reviewed to ensure working heights
for keyboards and monitors and seating were
appropriate. It was recommended that at least one
seated and one standing computer workstation per
area be equipped with adjustability features for
multi-users e.g. adjustable chair with foot ring,
adjustable keyboard tray that accommodates the
mouse.
Microscope work
Staff members per-
form a variety of
tasks. Microscope
work makes up a
small portion of the
daily activities and
the work can be
interspersed with
other tasks. Adjust-
able chairs are
provided at the
workstation to allow
for optimal positioning. Microscope forearm
supports were installed to eliminate contact stress
from forearms resting on the counter edge while
looking in the microscope.
Working space and layout, including storage
Lack of space was identified as a risk factor for
MSI due to difficulties with positioning (e.g. lack
of leg space, being in an aisle way) and moving
equipment and supplies in and out of the work area.
Much of the newer equipment is quite expansive
and lack of space around the machines, on working
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
51
surfaces and for storage was noted. It was
recommended that consideration be given to
relocating some workstations (e.g. box area,
pipette cleaning station) to allow for additional
working space and improved working postures.
In-patient testing and sampling
Identified risk factors for MSI included awkward
posture, static posture and forces associated with
such tasks as taking blood samples and placing
electrodes. Staff can optimize working postures by
asking the patient to move as close as possible,
adjusting the bed or stretcher height, lowering the
side rails, using bedside chairs and using adjustable
bedside tables for writing. Portable stools for blood
collection were trialed. The carts that hold
l a b o r a t o r y
supplies for
t r a n s p o r t
within the
facility have
m o d i f i e d
handles that
are raised and
extended to
allow for
better posture
when pushing (before the handle was too low and
too close to the cart to allow for foot clearance).
Recently the schedule for extended care units has
changed so that there are more frequent trips for
fewer residents. In addition, the need to perform
specific procedures per resident was reviewed to
maintain only necessary lab work and the schedule
will be revisited on an ongoing basis.
Outpatient laboratory
The out patient lab areas are equipped with height
adjustable chairs and stools for optimal positioning
while working with the patient. Adjustable patient
chairs are also available for use (the arm rests can
be raised to allow for a seated or standing posture).
If the patient is to be in a lying position, adjustable
stretchers are available for use.
7.11
Laundry and Linen Services
Handling laundry bags
Soiled linen is housed in cloth bags that are
supported on framed carts. On the units, they can
be wheeled close to the deposit area to minimize
manual handling. The bags are removed
downwards and therefore do not need to be lifted
up over the carts. Staff over filling bags can present
problems with manual handling. Unit staff are
encouraged to change bags often and not overfill
through continued facility-wide communication
and signage on individual units. In addition,
recommendations for cart design were made to
reduce the amount of laundry that can fit in each
bag.
Washing and drying laundry
Both dirty and clean laundry can be emptied in
false-bottom bins which helps to minimize the
amount of bend-
ing and reaching.
In addition, the
bin heights are
close to the
heights of both
the washing mach-
ines and dryers.
Anti-fatigue matting is provided at the folding table.
Recommendations were made to slightly lower the
bar on the carts for hanging personal laundry to
bring reaching below shoulder level.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
52
Stocking and delivering linen carts
As staff rotate between various duties, there is both
variety of tasks and postures provided. Information
on correct body mechanics is to be provided e.g.,
maintaining neutral positions, avoiding twisting of
trunk, alternating arms and minimizing push/pull
forces. It was recommended that staff continue to
consider placement of linen on the individual unit
carts so that the heaviest and most awkward items
are on middle shelves and lighter items are on upper
and lower shelves.
Sewing table
For spot repairs at the sewing machine, working
heights are appropriate with an adjustable chair
provided. Recommendations included improved
lighting with a task light and padded edging to
reduce compression of the forearms on the desk
edge.
7.12
Maintenance
Performing preventive and demand maintenance
Identified risk factors for MSI included awkward
posture, static posture and force associated with
repair and replacement of equipment, furniture, and
building systems. Available material handling
equipment includes hoists, dollies and carts.
Specialized handling equipment is rented if required.
Recommendations included providing general
material handling information to staff members, as
well as improvements to computer workstations
that are more frequently used.
7.13
Maternity and Pediatrics
Assisting with deliveries
Awkward posture, static posture and force
associated with holding patients legs during delivery
were identified as risk factors for MSI. Leg supports
are available if the birthing bed is broken (bottom
portion of the bed is removed for easier access to
patient during delivery) however, in some cases
they may still not place the legs in a suitable position
for delivery. Recommendations included having
discussions and documentation for all staff and
families on other alternatives to staff members
holding legs during delivery. Information on other
leg supports for maternity beds will be sought.
Assisting with breast feeding
Awkward and static postures while assisting with
breast feeding were also identified. Options
available to staff
include adjusting
the bed height to
the most appro-
priate position,
lowering the bed
height and using
available stools,
or having the patient seated on the couch or rocker
(available in each room). Options for positioning
the baby relative to the mother are also available
to staff. A chair designed for this purpose was
recommended for the nursery to be used when it is
a particularly awkward or difficult situation.
Moving equipment including beds
Forces and awkward postures were identified with
moving equipment such as incubators, baby
warmers, scales, monitors, case carts, cribs and beds.
It was recommended that general material handling
information be provided, wheeled equipment be
checked and repaired as appropriate by
Maintenance (in place), and that a door holder be
installed in one particular location so that the door
does not need to be held when wheeling equipment
in and out of a particular room.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
53
Caring for infants
The incubator height and bedding angle can be
adjusted to optimize arm positioning while providing
care for infants in incubators. It was suggested that
towels be placed over port-holes for support and
cushioning particularly with longer duration tasks
such as with feeding, and that frequent adjustments
be made to minimize static positioning. A cart for
transporting portable bath tubs filled with water,
and tubs with plugs (to eliminate requirement to
lift for draining) were recommended.
Patient handling
Although not as frequently used as in other units,
patient handling equipment including roller board
and transfer board are available to assist if required.
In addition, staff members have been provided with
information on assessing patients for weight bearing
prior to assisting them with mobility. Additional staff
can be called on to assist as appropriate.
7.14
Medical Unit
Providing nursing care
Identified risk factors for MSI included awkward
posture and static posture associated with various
nursing procedures (e.g. reaching and bending while
bathing, washing, changing dressings, starting IVs,
assisting with feeding). Information on stretches
to perform in between tasks and to counter the
effects of awkward and static positioning will be
developed. A site-wide MSIP bulletin (The MSIP
Minute) has been launched via the MSIP
committee and will be published bi-monthly
covering various MSIP topics for example, what
to do when a patient falls, moving beds, tips when
repositioning patients, using a transfer belt).
Dispensing medications and pill crushing
Risk factors such as awkward posture, force and
contact stress were identified with pushing
medication carts and crushing pills. MSI prevention
information on dispensing medications is to be
provided including suggestions for storage,
dispensing, and positioning. Various types of pill
crushers were recommended for use based on staff
preferences. Cushioning to reduce impact forces and
working heights close to elbow level were
suggested. In addition, work method suggestions
such as minimizing downward forces when
crushing the pills (only use the amount of force
necessary to crush), alternating hands used, only
crushing to level required (may not have to always
crush to a fine powder) and spooning with pudding.
It was also recommended that new medication carts
be purchased and this was implemented.
Patient handling and transfers
Risk factors of awkward posture, static posture and
force while doing patient transfers and repositioning
were identified, primarily with repositioning in bed,
dealing with patients who had fallen on the floor
and transferring to
commodes (brakes
sometimes not work-
ing). The type and
nature of transfers
varies from shift to
shift and from patient
to patient. Patient
conditions may be
constantly changing.
Assessments are con-
ducted by RNs or Rehabilitation staff. Patient
mobility is discussed at report at the beginning of
the shift. The importance of reassessing patients
before every transfer has been stressed with staff
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
54
Collecting and distributing supplies and equipment
Various postures and forces are associated with
loading, unloading, and delivering materials,
including food carts, laundry and linen supplies and
stock items. The truck tailgate and the facilitys
main loading bays
are equipped with
adjustable lifts.
Recommendations
included a non-slip
walkway in the
truck and in-
creased facility
wide awareness about the importance of not
overfilling laundry bags (as drivers have to handle
the bags also). In addition, there will be
consideration to modifying the laundry carts so that
the bags cannot be overfilled.
7.16
Operating Room including recovery
room
Set up before and after surgery
Identified risk factors for MSI included awkward
posture and force associated with setting up
equipment, supplies and instruments before and
after surgery. Bending and reaching may be required
to access items from shelving. Care has been taken
to ensure heaviest and most frequently used items
are on middle shelves. Alternating hands used and
using hand tools such as scissors to assist with
opening packaging can help to reduce forces,
primarily to hands. Flooring may be slippery;
proper footwear is emphasized and housekeeping
was reminded to use appropriate signage and dry
mop areas after wet mopping.
Assisting during surgery
Awkward and static postures may be assumed
while assisting with surgery e.g. prolonged standing,
in MSIP training sessions and through a staff
bulletin (MSIP Minute).
Staff can optimize working postures by asking the
patient to assist and instructing them how to assist
as much as possible, adjusting the bed height, using
Trendelenberg position (head down), lowering side
rails and ensuring a coordinated count is completed
when transferring with a partner. Additional
assistance can be sought from other staff on the
unit or Rehabilitation staff. Available patient
handling equipment includes mechanical lifts and
standing assists,
transfer (slider)
boards and transfer
belts. Some beds
are also equipped
with monkey bars.
Trials with sliding
sheets (for reducing
forces when repo-
sitioning patients in
bed) can be arranged through Physiotherapy
department. Staff will continue to be scheduled to
attend the MSIP patient handling training available
on site. In addition, it was recommended that
existing commodes be repaired or replaced due to
concerns with brakes not working.
7.15
Motor Services
Transporting supplies and equipment
The truck is equipped with an adjustable, cushioned
seat. Time spent seated is limited due to short
driving distances and frequent stops for deliveries
and pick-ups.Information including job specific
stretches and tips for correct adjustments for driving
(e.g. seat, mirrors) is to be provided.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
55
while positioning limbs or doing prep work, or
holding instruments and retracting during surgery.
Staff members do rotate positions within the OR
and during surgery to provide task variety. Stools
are available for sitting during surgery (when
possible, even for short periods of time). The OR
tables are height adjustable, with step stools
available for nursing staff if required. Power cords
can be plugged into either IV poles or wall sockets
to minimize tripping hazards.
Patient handling
Patient handling including moving patients on
stretcher and on and off operating table is required.
Stretcher and OR table heights can be adjusted to
improve posture (e.g. adjust height to minimize
trunk flexion). When possible, the patient is asked
to assist (e.g. move self as much as possible).
Assistive devices such as roller boards, transfer
(slider) boards and mechanical lift are used as
appropriate. Additional staff is available to provide
assistance if necessary. In-service training on key
points for patient transfers was completed by
Physiotherapy department.
Post-operation recovery area
Identified risk factors for MSI included awkward
posture and force associated with patient handling
and providing nursing care. When possible, 2 staff
members admit patients to minimize awkward
postures such as reaching (e.g. so that there is someone
on each side to hook up equipment, put blankets on,
position IV bags etc.). Equipment plugs are wall
mounted to minimize bending and reaching.
Adjustable chairs with foot ring are available at each
of the bays for monitoring the patient at bedside.
Storage shelves have been arranged to minimize
awkward positioning (heavier items on middle
shelves). The position of the bedside monitors
requires awkward postures to view the screens and
access controls. Flat-screen multi-purpose monitors
that can be height adjusted have been requested
through capital funding program. In addition, it was
recommended that storage of items in the work
area be carefully considered to minimize excess
equipment and improve access to required items.
OR Booking
Identified risk factors for MSI included awkward
posture and static postures associated with computer
and desktop paper work, as well as phone use.
During the assessment, changes were made to the
set up of the computer workstation to improve
positioning (e.g. chair adjusted, monitor angled
down). A headset is available for use to eliminate
the requirement to cradle the handset between the
ear and shoulder. As the existing keyboard drawer
did not accommodate the mouse (not wide
enough), it was recommended that the drawer be
replaced with an articulating keyboard platform that
is wide enough to fit the mouse and has a cushioned
wrist rest. Information on correct positioning at the
computer workstation and stretching exercises was
provided.
7.17
Pharmacy
Entering, checking and reviewing orders
There is a rotation
schedule set up in
which Pharmacists
and Technicians
rotate through
various posts in the
d e p a r t m e n t
including order
entry, order reviewing, dispensary and clinical
duties. Staff input as to rotation was sought. Floors
are carpeted and anti-fatigue mats are available to
minimize the effects of static positioning. The work
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
56
Receiving, unpacking and restocking
Identified risk factors for MSI included awkward
posture and force associated with receiving materials
from delivery area, unpacking and restocking
shelves in work area. Shelving is adjustable, with
slide out bins for easier access. Some reaching and
bending is required to access shelving. Step stools
are provided for accessing higher shelves and to
use as a seat when accessing lower shelves. Care
has been taken to ensure heaviest and most
frequently used items are on middle shelves.
Various carts and dollies are available to assist with
material handling. Work is self-paced, with
flexibility as to when certain tasks are performed.
There is task variety with movement and varying
postures to minimize static postures and provide a
natural break in between handling stock. Staff
members have flexibility as to how much to
handle, how to handle it and when to handle it in
order to minimize forces (e.g. boxes can be opened
and individual items handled). Additional staff can
be called on to assist if required. Staff members
have attended material handling training, general
handout information was also provided.
7.18
Portering
Transporting patients
Identified risk factors for MSI included awkward
posture and force associated with transporting
patients including moving beds. Beds and stretchers
are height adjustable and can be adjusted to
improve positioning. Concerns with transporting
in smaller areas (twisting and turning in tight
corners), in and out of elevators, maneuvering
around clutter in hallways and in and out of patient
rooms were noted. MSI prevention information
including job specific techniques for moving beds
is to be provided. Staff was reminded to report any
area is set up with several computer workstations,
some seated and some for standing. Workstations
include adjustable chairs, document holders, wrist
rests and monitor stands. Information on correct
positioning at the computer workstation and
stretching exercises was provided. Staff members
are encouraged to intersperse non-computer tasks
(such as visual checks) to provide for task variety
and a change in posture. Corner makers at L-
shaped workstations were trialed and subsequently
installed to allow for better placement of the
keyboard closer to the desk edge.
Dispensing orders including picking, filling and delivering
A kangaroo apron with pouches for items to rest
is available for use to eliminate the requirement to
hold various items. Items are typically lightweight,
not in excess of 1 kg. Some reaching and bending
is required to access shelving. Step stools are
provided for accessing higher shelves and to use as
a seat when accessing lower shelves. Various carts
and baskets are available to use for deliveries. It
was recommended that the cart handles be raised
and extended (to improve posture while pushing)
and that the wheels be repositioned so that the
rotating wheels are under the handle (to allow for
better control).
Batching and assembling IVs
This task involves the preparation of IVs at a laminar
flow hood as part of the CIVA program.
Technicians are rotated through this station, working
2-4 shifts over a 6-week rotation. An adjustable task
chair is available, with casters and foot ring. Staff
members are encouraged to take frequent posture
breaks (information on stretching exercises to be
provided). An automatic vial shaker is available and
used. Syringes can be loosened by initially pulling
out the plunger to release air. Trials with cushioned
edging or forearm supports were recommended.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
57
Charting
Initial patient assessments and charting for current
patients may mean long periods of writing. Nursing
station working heights are appropriate, with
adjustable seating available. Larger diameter pens
with rubber grips were recommended to reduce
pinch grip forces associated with writing.
7.20
Rehabilitation Services, including
Occupational Therapy, Physiotherapy
and Recreation Therapy
Conducting patient assessments and pro-gramming
Identified risk factors for MSI included awkward
postures, static postures and forces associated with
various duties for assessing patients and
implementing therapy programs. Required duties
vary daily depending on the therapeutic
interventions and patient characteristics.
Suggestions for reducing risk factors for MSI
included making appropriate adjustments to
equipment and furniture as available to improve
positioning (e.g. adjust bed height, adjust table
height) and varying tasks as appropriate.
Patient handling
Risk factors of awkward posture, static posture and
force while doing patient transfers and repositioning
were identified, primarily when assisting with
mobility and activities of daily living.
Rehabilitation staff may be perceived to be at
higher risk for unexpected patient responses (e.g.
falling and fainting) as they are often the first ones
to mobilize. Assistive devices (e.g. mechanical lifts,
transfer belts) are used as appropriate and additional
staff is available to provide assistance if necessary.
Department staff members are aware of correct
body mechanics and correct transfer techniques,
have attended MSIP training courses and act as
problems with transporting and/or equipment to
supervision such as mechanical problems with
stretchers and wheelchairs and cluttered hallways.
Patient handling
It was recommended that new porters or those that
have not attended training be scheduled for the
MSIP patient handling sessions currently ongoing
at LMH.
7.19
Psychiatry
Dealing with aggressive patients and patient handling
The majority of patients are ambulatory. If
required, a mechanical lift and transfer belts are
available for use. Unpredictable situations arise as
patients either unexpectedly fall or are prone to
aggression creating situations with risk factors for
injury. Pre-transfer assessment information has
been provided to staff members. It was
recommended that staff continue to be scheduled
for attendance at regional Management of
Aggressive Behaviour sessions. (For more
information on the violence risk assessment conducted,
contact the Fraser Health Authority.)
Moving beds
Bed were reportedly moved on a daily basis in order
to accommodate
room groupings.
During the risk
a s s e s s m e n t
project, new
Psychiatric beds
arrived as had
been requested
on the capital
funding list. The newer beds are lighter and con-
siderably easier to move, thus reducing the risk of
MSI.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
58
7.21
Social Work
Computer and phone work
Identified risk factors for MSI included awkward
postures, static postures and contact stress
associated with computer and phone work (e.g.
incorrect positioning at computer, lack of stretch
pauses, forearms resting on desk edge, crooking the
phones handset between ear and shoulder). During
individual site visits, various adjustments were made
to the set up of the computer workstations as per
ergonomics guidelines e.g. adjusting chair height
and backrest, improving mouse placement (putting
it beside keyboard), aligning monitor with
keyboard and adjusting monitor height.
Information on correct set up of the computer
workstation was provided, as well as information
on correct positioning of the phone and stretching
exercises. It was recommended that specific offices
be equipped with new chairs, footrests and
keyboard wrist rests.
Meeting and consulting with clients
Awkward postures may be assumed when meeting
and consulting with clients (e.g. leaning forwards,
sitting on edge of bed). Staff was reminded to use
proper body positioning when meeting with clients
for example, using chairs for sitting and bedside
tables (often adjustable) for writing as appropriate.
7.22
Sterile Processing
Rotation of staff
Staff members are all trained and perform duties
in all areas of Sterile Processing, including the
Operating Room. Currently rotation is done on a
daily basis, it was recommended that consideration
be given to more frequent rotation (every 4 hours),
especially through work areas requiring static
resources and trainers for on-site musculoskeletal
injury prevention programs for staff.
Accessing equipment
Identified risk factors for MSI included awkward
postures and forces associated with accessing
required equipment from storage areas. Often cited
was a lack of storage space, inadequate shelving,
or inappropriate access to items. Recommendations
included reorganizing current storage areas, and
determining additional storage requirements with
consideration to additional shelving and cupboards
for easier storage and access.
Working on wheelchairs
Awkward postures and forces were identified when
working on wheelchairs. Power tools (with
adjustable handle) and low chairs and step stools
for sitting have been provided. Work on wheelchairs
is primarily conducted in conjunction with other
required duties so postures vary. It was
recommended that knee pads be considered for the
wheelchair repair room.
Taking residents on outings
Risk factors for MSI included awkward postures and
forces associated with strapping wheelchairs into the
bus when taking extended care residents to and from
recreational and social functions. A new vehicle was
recently purchased. The vehicle is equipped with a
hydraulic lift for getting the wheelchairs on and off.
Recommendations included strapping the biggest
wheelchairs in first, using tubes on wheelchair brake
handles for easier access by staff, ensuring all staff
assist with strapping and alternate the side they are
strapping into. Additional recommendations
included provision of door stops (to hold doors open
while wheelchairs are coming in and out of the
building) and non-slip grating on the hydraulic lift
platform for improved footing.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
59
7.23
Stores and Shipping/Receiving
Receiving and putting away stock
Identified risk factors for MSI included awkward
posture and force associated with material handling
including lifting and carrying stock items.Various
handling assists are available such as carts, pallet
jacks (manual and motorized) and dollies. Postures
can be improved when unpacking by setting boxes
off the floor onto cart or pallet and cutting out the
sides. Work is self-paced, with flexibility as to when
certain tasks are performed. There is task variety
with movement and varying postures to minimize
static postures
and provide a
natural break in
between hand-
ling stock. Staff
members have
flexibility as to
how much to
handle, how to
handle it and
when to handle it in order to minimize forces.
Additional staff can be called on to assist if
required. Ergonomics tips for correct body
mechanics and storage of items and training
sessions with demonstrations and handouts on
manual material handling were also recommended.
Filling and delivering orders
Smaller items on the carousel as well as stock items
have been organized so that the heaviest and most
frequently accessed items are on middle shelves.
Shelf heights can be adjusted as required. Step
stools are available. Anti-fatigue matting is available
at the carousel counter. Various sizes and shapes
of carts are used for deliveries. New carts were
purchased as recommended, so that more are
available for use.
postures and fine
movements of the
upper extremities. In
addition, general
information on body
mechanics, correct
lifting techniques and
job specific stretching
exercises is to be
provided via handouts
or a presentation.
Disassembling and sorting
Identified risk factors for MSI included awkward
posture, static posture and force associated with
receiving instruments, handling carts and trays and
sorting. Counter heights are appropriate as per
guidelines. Anti-fatigue matting is available. It was
recommended that maintenance be contacted if
the wheels on the carts make them difficult to move.
Cleaning and decontaminating instruments
Working counter heights are appropriate. Deep
sinks are equipped with false bottoms (an upside
down bin) to minimize bending. Decontamination
is completed with automated equipment. Loading
of instruments is done so that heavier items are on
middle racks.
Assembling and wrapping instruments
Fine motor movements of the hands and fingers
are required for assembling and wrapping
instruments and instrument sets. Anti-fatigue
matting is available. More frequent rotation of staff
was recommended. Due to effort required to open
and close wooden drawers (they get stuck), it was
recommended that drawer guides be installed to
reduce forces.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
60
Computer inventory input and tracking
Set up of computer workstations was reviewed.
Minor changes were completed to improve
alignment of the monitor with the keyboard to
reduce twisting and lower monitor height. Low file
drawer (requiring bending to access) was replaced
with a larger, upright file cabinet. Information on
set up and stretching exercises was provided.
7.24
Surgical Unit including Surgical Day
Care
Providing nursing care, including personal hygiene
Identified risk factors for MSI included awkward
posture, static posture and force associated with
providing general nursing care (including taking
vitals, changing dressings, washing and feeding).
Information on stretches to perform in between
tasks and to counter the effects of awkward and
static positioning will be developed. It was
recommended that existing commodes be repaired
or replaced due to concerns with brakes not
working. These are already on the Capital Budget
list for this year as a top priority. For charting, both
seated and standing areas are available. Working
heights are appropriate. Adjustable chairs are
provided.
Handling laundry bags
Laundry bags are on
wheeled carts. When
full, the bag is
wheeled to utility
room, removed from
frame and placed in
linen cart. Freq-
uently changing both
the bags and the linen
carts will help to
minimize awkward
postures and forces associated with handling. Site-
wide communication to reflect these ideas will be
undertaken. Signage about not overfilling bags is
also posted at various locations throughout the unit.
Equipment use, movement and storage
Adequate equipment
and equipment in
good working order is
important. Due to
frequency of use on
this unit, it was
recommended that
additional automatic
blood pressure mon-
itors be purchased.
These had already
been on the capital funding list, and were recently
purchased and provided to the surgical unit.
Existing Geri-chairs may require awkward postures
to adjust and position the trays. Repair or
replacement of Geri-chairs was recommended and
this is also already on the capital funding list. Lack
of storage space may lead to items being stored in
hallways or in utility rooms creating clutter and
making it difficult to quickly access needed items.
It was recommended that all equipment stored on
the unit be reviewed to see if items not used can
be moved or stored elsewhere. Where required, it
was recommended that maintenance be contacted
to repair rolling stock (e.g. IV poles that are difficult
to adjust, Geri-chairs that are difficult to adjust).
In surgical day care, the small oxygen tanks stored
under the stretcher stick out creating a bumping
(contact stress) hazard for staff. The holders were
subsequently modified so that the tanks can be slid
farther in and do not stick out beyond the frame
of the stretcher.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
61
Dispensing medications
Dispensing medication involves opening packets and
bottles, measuring, crushing, mixing and pouring.
Awkward postures were identified from reaching
and bending to retrieve medications from cupboards
and drawers. Existing medication carts were
deemed to be appropriate. Suggestions for pill
crushing included placing a cushion underneath and
on the handle to reduce impact forces, technique
tips (e.g. to not bang, determine appropriate level
to crush). Alternatives to crushing include pill
cutting (cutter available) and dispensing in liquid.
Patient handling and transfers
The type and nature of transfers varies from shift to
shift and from patient to patient. Staff can optimize
working postures by asking the patient to assist and
instructing them how to assist as much as possible,
adjusting the bed height and lowering side rails and
ensuring a coordinated count is completed when
transferring with a partner. Additional assistance
can be sought from other staff on the unit or
Rehabilitation staff. Available patient handling
equipment includes mechanical lift and standing
assist, transfer (slider) board and transfer belts.
Some beds are also equipped with monkey bars.
Trials with sliding sheets (for reducing forces when
repositioning patients in bed) can be arranged
through Physiotherapy department. Staff will
continue to be scheduled to attend the MSIP patient
handling training available on site.
Pre-admission interviewing
The pre-admission office is set up for staff to
interview and input client information into the
computer. During the site assessment, changes were
made to the set-up of the computer workstation
as per ergonomics guidelines (e.g. monitor
repositioned, chair adjusted). In addition,
information on correct set-up and adjustments and
example stretching exercises were provided. An
adjustable keyboard platform that fits the mouse
and keyboard wrist rest were recommended and
purchased. A desk slant was also trialed. It was
recommended that the admission office be
rearranged: the desk was rotated so that the client
now sits parallel to the desk reducing awkward
postures and twisting on the part of the staff
member doing the interview and inputting
information into the computer at the same time. The
filing cabinet was also moved to provide more room
for additional seated guests.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
62
8.0
PROJECT OUTCOMES
8.1
Introduction
The goal of the ergonomics risk assessment project
was to determine which jobs/tasks contribute to
musculoskeletal injury, which workers are likely to
be affected, identify nature of the risks, and
recommend control measures to reduce the risk. This
was accomplished through the completion of 120
risk assessment reports covering all areas of the
facility. Statistical information from the risk
assessments completed and a discussion on the
projects final outcomes as outlined in Section 1.0
of this report are presented.
8.2
Risk Assessments Reports Completed
Targets established at the onset of the project with
regards to completion of the risk assessments were
met. 120 department-specific occupations had a risk
assessment completed, using the standardized
process and tools outlined in Section 3.0 of this
report. The entire project was completed within the
18-month timeframe (the final report was completed
one month later).
The following points and charts provide information
on the risk assessment reports and their
recommendations. The table of data can be found
in Appended F-1, page xxxix.
8.2.1
Classifying risk assessments completed
according to type of work conducted
The individual occupation-specific risk assessments
completed were classified based on the type of
work that is conducted the majority of time.
Categories used were single computer workstation,
multi-user computer workstation, patient handling
require-ments, or material handling requirements.A
breakdown of the classification of 120 reports at the
facility is as follows (depicted in Figure 8.1):
20% of the risk assessments were conducted
on single user computer workstations (e.g.
single office with desk and computer work-
station). Primary risk factors were associated
with computer work.
20% of the risk assessments were conducted
on multi-user computer workstations (e.g. unit
clerks, admitting desks). Primary risk factors
were associated with computer work and
having the ability to adjust for different
operators.
35% of the risk assessments were conducted
with occupations that have at least some duties
related to patient or resident handling (e.g.
RNs, Care Aides, LPNs, Porters, Diagnostic
Imaging Technologists). Many risk factors
identified were associated with patient/
resident handling.
25% of the risk assessments were conducted
with occupations that have at least some
duties related to material handling and not
patient handling (e.g. Cleaners, Food Service
Workers, Stores Attendants, Laboratory
Technologists). Many risk factors identified
were associated with material handling.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
63
Individual computer
20%
Material Handling
25%
Patient Handling
35%
Multi-user computer
20%
Figure 8.1 - Categorization of Completed Risk
Assessment Reports
8.3
Recommendations from Risk Assess-
ment Reports Completed
The following statistics on recommendations from
the risk assessments were compiled in July 2002 using
a sample of 100 reports: 20% or 20 single user
computer workstation reports, 20% or 20 multi-user
computer workstations, 35% or 35 patient handling
reports and 25% or 25 material handling reports.
8.3.1
Type of Recommendations
Recommendations were coded as training/
information, work process, maintenance, minor
capital expenditure (< $2000) or major capital
expenditure (>$2000). See Figure 8.2.
Overall: For all reports, 31% of the recommend-
ations were related to providing training and/or
written materials; 33% were related to work processes
or work technique suggestions; 8% were related to
maintenance issues; 24% were related to minor
capital expenses (< $2000); and 4% were related to
major capital expenses (> $2000).
Individual and multi-user computer workstations:
For both individual and multi-user computer
workstations approximately 60-70% of the
recommendations were associated with providing
training and/or written materials or suggesting work
process and technique changes. Approximately 25-
30% of the recommendations were related to minor
capital expenditures (e.g. office chair, adjustable
keyboard tray, keyboard wrist rest, footrest). There
was only one report with capital expenditures
suggested for future consideration (office
renovations).
Material handling: For reports classified as material
handling, 26% of the recommendations were related
to providing training and information, 38% were
related to suggestions for changes in work processes
or work techniques, 8% were related to maintenance
and 26% were related to minor capital expenditures
(e.g. equipment such as chairs, lighting). Only 2%
were related to major capital expenditures (e.g.
material handling carts, changes to layout and
counters).
Patient handling: For reports classified as patient
handling, 36% of the recommendations were related
to providing training and information, 28% were
related to suggestions for changes in work processes
or work techniques, 8% were related to maintenance
and 16% were related to minor capital expenditures
(e.g. equipment such as chairs, matting). 12% were
related to major capital expenditures (e.g. beds,
mechanical lifts, and other equipment such as
monitors).
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
64
Figure 8.2 - Type of Recommendation by Category of Report Completed
8.3.2
Status of recommendations
At the end of the project timeline, almost half of
the recommendations made (45%) have been
implemented or are in progress. This is a significant
number considering many of the risk assessment
reports were only completed in the final 6-month
period. As shown in figure 8.3, a higher percentage
of recommendations have been implemented for
computer workstation reports. This is likely due to
the fact that recommended controls for computer
workstations typically involve relatively easy and
inexpensive changes and involve fewer number of
staff (e.g. suggested changes and training are easier
to implement with fewer staff numbers). A lower
percentage of recommendations have been
implemented for patient handling and material
handling work areas likely due to higher staffing
numbers (e.g. more people to train), higher cost of
some capital items and a more in-depth process for
obtaining funding approvals. Interim measures such
as changes to work processes and provision of
education/information are in place or underway. As
outlined in this reports conclusion, after this project
there will be resources within the health authority
dedicated to creating and disseminating job specific
information as recommended in the risk assessment
reports.
As previously mentioned, there will be continued
follow-up and tracking on the status of the reports
recommendations via the database. As the reports
are input into the database, there will be additional
information readily available regarding the
recommendations (e.g. status by recommendation
type).
0%
20%
40%
60%
80%
100%
Total Ind computer Mult-user
computer
Mat. Handling Pt. Handling
Category of Risk Assessment Report
P
e
r
c
e
n
t
Major capital (> $2000)
Minor Capital (<$2000)
Maintenance
Work Process
Training/Information
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
65
8.3.3
Cost of recommendations for capital
items per risk assessment report
completed
Overall, one quarter of the reports completed (26%)
had no capital items associated with the
recommendations. Approximately half (46%) of the
reports had their capital items add up to less than
$500. Reports associated with computer works-
tations (with one exception) all contained
recommendations with capital items costing less than
$500. This is reflective of efforts to make at least a
portion of the recommendations relatively easy and
inexpensive to implement. As shown in figure 8.4,
a higher percentage of reports in material handling
and patient handling areas (12% and 46%
respectively) had capital items adding up to be
more than $2000.
0%
20%
40%
60%
80%
100%
Tot al Ind
comput er
Mul t - user
c omput er
Mat .
Handl i ng
Pt .
Handl i ng
Cat egor y of Ri sk Assessment Repor t
P
e
r
c
e
n
t
Not compl et e
On capi t al l i st
Compl et e/ i n pr ogr ess
0%
20%
40%
60%
80%
100%
Total Ind computer Mult-user
computer
Mat. Handling Pt. Handling
Category of Risk Assessment Report
P
e
r
c
e
n
t
Costs of > $2000
Costs of $500-2000
Costs of < $500
Costs of $0
Figure 8.4 - Total Cost of Recommendations Per Report Category
Figure 8.3 - Status of Recommendation by Category of Report Completed
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
66
8.4
Intended outcomes
A discussion on the projects final outcomes
compared with its intended outcomes (as outlined
in Section 1 of this report) follows:
8.4.1
Meeting WCB Ergonomics (MSI)
Requirements
The risk assessment process was designed to review
all occupations at the facility to identify factors in
the workplace that may expose workers to a risk of
MSI, assess the degree of risk and recommend
controls as per WCB Ergonomics (MSI) Require-
ments. Consultation continued through regular
updates to Steering Committee members, JOSH
Committee members and LMH staff, including
senior administration. Periodic updates were
provided to LMH Management staff for distribution
to all employees.
The project meets the intent of the requirements:
With few exceptions (Biomedical Engineer-
ing and Respiratory Therapy were not
completed within the projects timeline), all
occupations were reviewed to identify and
assess risk factors associated with MSIs. In
total, 120 reports for risk assessment were
completed. This exceeds the requirements of
the Occupational Health and Safety
Regulation for risk identification and risk
assessment. However, this was completed in
order to carry out the requirements as defined
in the projects description.
Consultation: Feedback and consultation
from workers regarding MSIs and specific job
duties was carried out through distribution
of the symptom survey, and discussions at
meetings and during job observations.
Risk Identification and Assessment: Risk
factors for MSI that were considered in the
risk identification phases included those
outlined in the WCB Ergonomics Require-
ments, including those associated with 1)
physical demands of work, 2) workplace
layout and condition, 3) objects handled, and
4) work organization.
Risk Control: Recommended risk controls
were provided for each assessment. Recom-
mendations included engineering and
administrative controls. There were few
recommendations for personal protective
equipment.
Education: General information on MSIs (e.g.
signs and symptoms, risk factors) was
provided to all employees. In addition,
information related to patient handling,
material handling and office ergonomics was
developed and distributed as appropriate.
There will be ongoing efforts to continue to
provide job specific information based on the
findings of the risk assessments.
Future risk assessments are planned within the
health authority using a prioritization scheme such
as the one outlined in Section 2.0 of this report,
and using the processes and tools outlined in Section
3.0 of this report.
8.4.2
Increased awareness of MSI signs and
symptoms, risk factors and preventive
strategies
It was intended that the project would increase
awareness of MSIs in the health care setting. There
would be increased worker awareness of the signs,
symptoms and risk factors for MSI. As well, there
would be increased awareness of the control
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
67
measures that can be put in place to reduce the
risk of MSI, including engineering and
administrative controls such as new equipment or
improved design, changes to work space and
layout, and updated work processes and practices.
The project was designed to increase awareness
through on-the-job observations, distribution of
employee symptom surveys and through discussions
with employees as part of the risk factor
identification phase. Additional information through
presentations, pamphlets and newsletter articles was
used to heighten awareness of MSIs. Some
departments received job-specific information related
to risk factors and injury prevention strategies and
this will continue after the projects completion.
At this point in the project, we have been unable to
quantitatively measure awareness. Verbal reports
from staff, supervisors and committee indicate that
there has been increased awareness. Future initiatives
including a follow-up survey for staff are planned in
order to better quantify this variable.
8.4.3
Establishment of tools for identifying,
assessing and controlling risk factors for
MSI
A set of tools for risk assessment has been
developed. Tools include flow charts outlining a
processes for conducting risk assessment, a method
for prioritizing based on MSI incident statistics, an
employee symptom survey, a task analysis worksheet,
a final report format documenting assessment
findings, and checklists to assist in risk factor
identification. A description and examples of the
tools used can be found in Section 3.0 of this report.
8.4.4
Establishment of database of risk
assessment information
A risk assessment database was conceptualized,
designed and created to house data and information
from the risk assessments conducted. The database
features search capabilities on job tasks and variables.
Report generation capabilities include follow-up
reports on recommendations and reports on risk
factors associated with particular tasks for return to
work plans. More information on the risk assessment
database can be found in Section 4.0.
8.5
MSI incident statistics: comparisons at
the projects conclusion
The following points and charts provide information
on the change in MSI incident statistics at the end
of the project. The table of data can be found in
Appended F-2, page xl.
8.5.1
Expectations
On completion of the project, it was expected that
the rate of MSI incidents would remain the same or
increase (increased reporting due to increased
awareness) but that there would be a reduction in
the duration (severity) of work-related injuries and
their associated costs. These expectations were met.
The reductions positively impact departments
financially by resulting in less time loss, less time to
backfill with other staff and reduced WCB top-up
costs (top-up costs are the costs directly attributed
to departments for top-up of salaries of employees
who are receiving WCB benefits). There are also
additional employee benefits such as less suffering,
increased job satisfaction and increased morale.
An analysis of LMHs injury statistics at the
conclusion of the 18-month project was completed
in order to provide comparisons with before and after
the onset of the project.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
68
Pre-Proj ect Post-Proj ect
S
e
v
e
r
i
t
y
R
a
t
e
Severity rate all incidents Severi ty rate MSIs onl y
Pre-Project Post-Project
F
r
e
q
u
e
n
c
y
r
a
t
e
Frequency rate all incidents Frequency rate MSIs only
Figure 8.5 Change in Frequency Rate
Severity rate/duration of injury: There has been
a decrease in the number of lost days per lost time
incident. For all incident types, the severity rate
decreased 28%. For MSI incidents only, the severity
rate dropped 43%.
Figure 8.6 Change in Severity Rate
8.5.2
Methodology for comparison
Incident data from 2000 that was previously
compiled in the initial phases of the project was used
as baseline data. The 12 months of baseline data was
normalized for an 18-month timeframe by
multiplying values by 1.5. This data (based on an
18-month timeframe prior to the onset of the project)
was labelled as the pre-project data.
Actual values from the 18-month timeframe after
project onset (January 01, 2001 up to June 30, 2002)
were then compiled and are used to represent the
post-project values. The post-project values were
then compared with the pre-project values (based
on data from the year 2000), to determine changes
that have taken place over the course of the project.
8.5.3
Comparing pre-project with post-
project statistics
When comparing pre-project statistics with post-
project statistics, the following summarizes the
findings:
Frequency rate of reported incidents: There has
been an increase in the rate of lost time incidents
and in the rate of reporting. Compared with baseline
levels, the frequency rate (lost time incidents) has
increased 10%. The frequency rate for MSI incidents
only (lost time) has increased 2%. This is an indicator
of an increased rate of injury, but may also indicate
more reporting due to increased awareness. When
accounting for the frequency of reporting based on
staff numbers, report only incidents increased 17%
for all incident types; and 6% for MSIs only.
} +10%
} + 2%
Pre-Project Post-Project
W
C
B
C
o
s
t
s
WCB costs all incidents WCB costs MSIs only
WCB costs: WCB claims costs for all incidents have
decreased 34%. When looking at MSI incidents only,
WCB costs have decreased 44%. In terms of WCB
costs, the 44% decrease has meant savings of
$180,000 in direct claims costs (compensation and
medical costs) over 18 months.
Figure 8.7 Change in WCB Costs
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
69
$140,000 total: including salaries and benefits,
database development and expenses (travel, office
supplies).
WCB funding for the project was provided so that
ergonomics risk assessments for all occupations
within the facility could be completed. The intent
(as accomplished) was that all the occupations within
the facility would undergo assessment and that each
assessment conducted would provide the manager
with recommendations for reducing the risk of MSI.
The project costs do not include the cost of
implementation of the recommendations. Individual
departments covered those costs either within their
operating budgets or through the capital funding
program.
As reported in a previous section of this report, 45%
of the recommendations have been implemented
with 55% outstanding. On preliminary review, it was
difficult to determine when the recommendations
from the risk assessment reports were the primary
motivator of the change having taken place. Many
of the recommendations for improvements via the
capital funding program were already on the list
(managers had already identified the problems) and
the reports provided additional emphasis. In other
cases, there were multiple benefits (including
ergonomics) for implementing the recommendations
and these were all taken into consideration. For
example, some equipment that needed to be
upgraded for patient care requirements had
additional ergonomic features that made it easier
for staff to use. These changes were justified for other
reasons in addition to ergonomics. Further follow-
up and cost/benefit analyses per department are
planned at a later date.
Percent of MSIs is down: 51% of all reported
incidents were MSIs (compared with 55% pre-
project), and 72% of lost time incidents were MSIs
(down from 77% pre-project). Other injury types
remain contusions, cuts, needle pokes, blood/body
fluid exposure and burns. 75% of WCB claim costs
and days lost (WCB claims) were related to MSIs.
In 2000, 90% of WCB claim costs and days lost were
attributed to MSIs.
Fewer MSIs in ECUs: 20% of MSIs occurred in
extended care facilities, down from pre-project levels
of 40%.
Fewer MSIs with Care Aides, more with RNs:
24% of MSIs are related to long term care aides
(down from 35% pre-project), 27% related to RNs
(up from 15%), 11% to food service workers (down
13%), 7% to cleaners (down from 9%), 7% to LPNs
(down from 8%).
Patient handling and material handling remain
activities with highest incidents: 13% of MSIs are
related to patient transfers (down from 25%), 21%
to manual material handling (up from 15%), 13% to
patient repositioning (same), 12% to slips/falls (up
from 10%), and 8% to violent acts (same).
Back, neck and shoulder remain most likely
affected: 19% of MSIs are related to back (down
from 32%), 18% to neck and/or shoulder (down from
26%), and 19%% to multiple sites involving the back,
neck and/or shoulder (up from 10%).
8.6
Project costs and savings
8.6.1
Project costs
The following costs are attributed to the project, over
the 18-month timeline:
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
70
not been estimated and therefore have not been
included in the evaluation.
Over the course of the project (18-months):
WCB direct claims costs decreased
$180,000
WCB top-up costs decreased $34,000
The average cost per MSI claim decreased
$1,200, and average days lost per MSI claim
decreased 10.2 days.
Project savings are reflected as the sum of the
decrease in WCB direct claims costs and WCB top-
up costs: $180,000 + $34,000 = $214,000 in savings
over the 18-month period of the project.
Savings in employee benefit costs, case management
costs, and other indirect costs have not been included
in this evaluation.
8.6.3
Net Benefit of project
Total savings of $214,000 on injury costs
minus project costs of $140,000 yields a net
benefit to the organization of $74,000.
Additional savings (can be estimated at 4
times direct savings, see above WSIB
reference) would be expected when factoring
in additional savings in benefits and indirect
costs.
Much of the initial groundwork has been
done. As risk assessment continues within
the health authority, program costs and
expenditures will be reduced and it is likely
that there will be continued savings in WCB
claims costs.
8.6.2
Estimated project savings
Project savings are estimated in terms of the
difference in WCB injury costs for MSIs only when
incident data before project onset (18-month
timeframe) is compared with data after the project
onset (18-month timeframe).
When reviewing injury costs for the purposes of
comparison before and after the project onset, the
following variables were evaluated:
WCB direct claims costs, including comp-
ensation (wage replacement) and medical
costs. These costs are paid by the WCB and
are used, in part, in the calculation of the
premium that the organization is charged by
the WCB. Higher claims costs will be
reflected in higher premium costs.
WCB top-up costs, which are 25% of the WCB
compensation (wage replacement) costs
1
.
These costs are paid by the individual
departments to top-up the injured
employees salary to levels as per collective
agreements.
There are also the costs of benefits paid to injured
workers. In addition, there are case management
costs, including administrative costs, accident
investigation and record keeping costs, training and
replacement costs, overtime, etc. These costs can also
be referred to as indirect costs and are estimated at
4 times the direct costs (Reference: Workplace Safety
and Insurance Board {WSIB}, Business Results
Through Health and Safety). Benefits, case
management costs and other indirect costs have
1 WCB compensation costs were calculated to be 75% of
the WCB direct claims costs (compensation + medical)
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
71
8.7
Whats happening at LMH to affect
change?
In addition to the ergonomics risk assessment
project, there were a number of initiatives ongoing
at LMH, which may have contributed to these
positive trends seen in both WCB costs and days
lost. Although not intended as an exhaustive list,
the following examples are provided:
During the project timeframe, there were
various projects on the go at LMH that may
have contributed to overall awareness of
employees about injuries and their related
causes. Other initiatives included the other
risk assessment projects (e.g. violence,
blood/body fluids and chemical risk
assessment), ceiling lift installations, Caring
for the Caregiver project, and early return
to work pilot project.
MSIP training by Rehabilitation Services
staff was ongoing with revised patient
handling training conducted twice monthly
for new staff orientation and for existing staff
starting in the spring of 2001. Manual
material handling training was also ongoing
for new staff.
There was continuing emphasis on incident
investigation and follow-up, and increased
awareness as attention and resources
focussed on reducing injuries.
There was increased awareness about MSIs
due to project processes such as the symptom
survey and job observations, in addition to
continuing employee handouts, newsletter
articles, Intranet postings, posters and
displays.
Improvements were made as managers had
previously budgeted for and received funding
for changes in the workplace such as new
equipment, new furniture and renovations.
8.8
Project feedback from managers and
steering committee members
In June 2002, a short one-page survey was sent
out to managers to get feedback on the project.
The survey is attached in Appendix F-3, page xli.
As well, a short set of questions similar to those in
the survey was sent out to Steering Committee
members.
The survey asked whether respondents were aware
of the project and changes made to theirs or other
departments; whether they felt it was a worthwhile
project for LMH and their staff; as well as what they
liked about the project and any suggestions for
change.
Of the 25 surveys sent out, 14 were returned (56%
return rate). A summary of the survey findings
follows:
100% of respondents were aware that the ergo-
nomics risk assessment project had taken
place on site.
83% of respondents were aware of changes
made as a result of the project in their own
department, dropping to 36% who were aware
of changes made in other departments.
100% of respondents felt that the project was
worthwhile for the facility and 100% of
respondents felt that the project was worth-
while for individual departments/staff.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority
72
The most commonly cited features of the project:
Good communication with staff. Respon-
dents felt that they were kept informed as to
what was happening both with the project
overall and when assessments were being
conducted in their departments.
Good one on one interaction, contact and
consultation with staff.
As far as process, there were comments that
the strategy for gathering information was
well done.
The project was inclusive by focussing on
critical areas first but also incorporating less
critical areas for assessment.
There were comments from respondents that
they felt the project brought awareness of
ergonomics issues to staffs attention.
Respondents cited having simple, cost
effective recommendations and solutions as
a positive feature.
Respondents stated that it was helpful to have
problem areas identified by staff other than
those within the department itself.
Suggestions for improvement included better
access to incident information prior to 1999 (this
would have reduced the time spent initially
compiling statistical information) and comments
that there should have been a separate source of
funding provided via the project to assist individual
departments with implementing the recom-
mendations.
8.9
Conclusions
Funding for this project from the WCB is gratefully
acknowledged. There was great cooperation and
commitment from union and management groups
to both get the project started and in providing input
and guidance throughout the entire timeline.
Overall, the project is to be judged a success. It
was completed on time and on budget. It met its
intended outcomes, including the establishment of
a process and tools for conducting risk assessments
in healthcare. The facility was able to realize
decreases in both the cost of WCB claims and time
loss over the course of the project. In addition, there
was positive feedback from participants (as
measured from completed surveys). It is hoped that
the projects findings will provide information that
is of value to other healthcare facilities as far as
risk factors and strategies for prevention of MSIs.
Ergonomics (Musculoskeletal) Risk Assessment Project
South Fraser Health Authority 73
9.0
CONCLUSIONS
9.1
What worked?
The ergonomics risk assessment project was
successfully completed. The project proceeded
through job action and contract re-negotiations as
well as through amalgamation and re-organizational
activities of the health authorities.
At the conclusion of the project, the following points
are offered as potential elements that were keys to
success:
Communication:
Good communication was repeatedly cited as a
positive feature of this project. Staff cited that there
was good communication throughout the project
both with the overall progress of the project and
within individual departments as assessments were
taking place.
At the projects outset, a communication plan was
mapped out as to the various communication
vehicles that could be used to inform staff about the
project (e.g. e-mails, management meetings,
newsletter, joint occupational safety and health
committee reports). In addition, the most appropriate
phases to plan communication were identified (e.g.
at the onset, after analysis of MSI incidents was
complete, case studies of some risk assessments
completed). As the project unfolded, it was obvious
that this was a worthwhile endeavour and kept staff
informed and increased awareness about the project.
Increased awareness through one on one time
with staff:
This project demonstrated the value of taking time
to observe and talk with staff about issues related to
MSIs. From both the assessors perspective and from
staff comments informally and on the project follow-
up survey, one of the most important elements of
the risk identification phase was the hands-on
approach with staff. This phase helped to increase
awareness about the project, helped increase
awareness with staff about MSIs, provided a needed
avenue for the identification of risk factors, and
allowed ideas and suggestions for improvements
(including hints on individual techniques) to be
informally presented and openly discussed.
Asking for staff feedback and talking with staff
through the course of the job observations, and
listening and recording what staff had to say was a
crucial part of the process. It was also one of the
most time-consuming components but essential in
terms of getting feedback, input and ideas from staff
(the experts). Many times staff members alluded to
the fact that it was just good to be able to relay
problems to someone and that it was nice to have
the opportunity to have input. Conducting job
observations after having distributed the symptom
surveys worked well to allow staff that did not fill
out the survey to have their say, as well as promoting
further surveys to be filled out.
As the project progressed, the intent was to spend
less time doing job observations as the assessor
gained more familiarity with the tasks and risk
factors. In reality, the time spent on job observations
did not decrease much due to the perceived
importance of this phase and the ability to get such
great staff input and feedback through this phase.
The process developed works:
The process and tools for risk assessment developed
over the course of this project underwent some
revisions but for the most part remained similar to
the original formats. It was much easier to document
the process and tools after actually starting to do the
Ergonomics (Musculoskeletal) Risk Assessment Project
South Fraser Health Authority
74
risk assessments and be able to test it out, as
opposed to reading and reviewing about how it
should be done on paper. We conclude that the
process developed worked as risk factors were
successfully identified, assessed and controls
recommended using the tools developed.
The process also confirmed many things we already
knew about risk factors and many things that
managers were already aware of so there were no
real surprises. Although some may conclude that we
were stating the obvious and a that formal risk
assessment was not required, there is a counter
argument that having another vehicle for
identification and documentation of recommended
controls was important for the process of
implementation. In addition, as demonstrated in the
previous section on project outcomes, there was a
positive impact on both WCB costs and days lost
translating into cost savings for the facility as a whole.
Risk identification is already in place, a formal
process is helpful:
Similar to the above points, many times the risk
assessment process confirmed what facility personnel
were already aware of. There was little startling
evidence of risk factors that was presented. This
bodes well for the validity of the process developed
but also shows that facility managers are already
aware of and making changes to reduce injuries in
the workplace. There were many items recom-
mended that were already on the list for capital
funding (and had been for more than a year) or were
already in the process of having changes made.
Simply having a more formal process from outside
the department of documenting risk factors and
recommending changes allowed managers to
reference the reports when requesting changes. In
addition, the recommendations and process used
helped to heighten awareness and bring issues about
musculoskeletal injuries to the forefront.
Recommending a variety of approaches to risk
control is effective:
This project was not undertaken as a research project
in a controlled environment with the objective to
determine what factors affect change. Instead, the
projects intent was to complete risk assessments
throughout the facility as per the WCB Ergonomics
Requirements, with intended outcomes including
increased awareness, establishment of a process and
database for risk assessment, and reduced injury
duration and costs. These intended outcomes were
met and discussed in the previous section. The
positive outcomes in terms of reduced days lost and
costs cannot be attributed to any one or two
initiatives either as a result of this project or outside
it. Instead what has been demonstrated is that a risk
control strategy including risk assessment, worker
consultation, recommendations for short term and
longer-term changes, training and education,
maintenance, work processes, and new or improved
equipment can be highly effective.
A more streamlined process is required:
This project was completed under the terms of the
contract, which required complete risk assessments
on all the occupations within the facility. This created
a need to develop and refine data collection tools,
an electronic database, education materials, and a
process for data collection and communication. The
knowledge and experience gained from this project
can be used by other facilities to significantly
streamline the process, enabling others to achieve
similar results with a reduced investment of time and
resources. The tools and methodology outlined in
this report can be adopted as is, or modified to suit
Ergonomics (Musculoskeletal) Risk Assessment Project
South Fraser Health Authority 75
the needs of another facility. In addition, using a set
of completed risk assessments for a variety of
positions as a starting point instead of a blank page,
can significantly reduce the work associated with
conducting risk assessments for similar jobs by
avoiding the tendency to reinvent the wheel. This
enables more emphasis to be placed on choosing and
implementing appropriate controls as well as the
ability to apply at least some of the findings to other
areas as appropriate.
9.2
What would we change?
At the conclusion of the project, the following points
are offered as potential elements for change:
Communication:
As evidenced from the follow-up surveys and in
discussions with staff, there was little awareness of
positive changes being made at the facility outside
of ones own department. This point was raised in
the section on facility wide recommendations, where
it was proposed that there be more communication
to staff about positive changes either through a
newsletter, e-mails, staff bulletins or other means.
In hindsight, it may have been effective to present
more frequent examples of changes taking place as
a result of the project through more means than just
presentations.
Separate funding?
Also noted on the follow-up survey was the comment
that there should have been funding provided by the
project to assist with the implementation of
recommendations. This is a valid point in terms of
providing the financial means to realize some of the
recommended changes; everyone is aware of how
tight funding is in the healthcare industry. There are
so many competing requirements for patient care that
health and safety issues are often perceived to be
lower in priority. It is however, our opinion, that
simply having a one-time fund for changes as a result
of this project will not lead to lasting change in the
workplace and is therefore not something that would
be recommended for future projects. Funding for this
projects recommendations could not be provided
externally (obviously so as not to show favouritism),
but the comment was made that there be a source
internally. This could have been accomplished within
each facility or through the Workplace Safety and
Wellness department but the questions around
competing priorities and sorting out who should get
what and when will always exist. It is concluded that
for lasting change to be sustained, and for health and
safety priorities to continue to compete successfully
with other priorities, that individual department
requirements continue to be funded through the same
channels as other requirements.
Clerical support:
Additional clerical support, primarily for assistance
with database entry would have been beneficial for
meeting the timeline for input and being able to more
effectively use the database during the timeframe of
the project. This will now be accomplished after the
project deadline.
9.3
Whats next?
As the project is winding down, the following items
are planned for the future of risk assessment within
the health authority:
Risk assessment as a component of the
authority-wide ergonomics program: Risk
assessment will be an important component
of the ergonomics program authority-wide.
Using elements of the process and tools dev-
Ergonomics (Musculoskeletal) Risk Assessment Project
South Fraser Health Authority
76
eloped for this project, departments within
the authority will be prioritized for risk
assessment. Efforts will be made to provide
risk assessment services through the
Workplace Safety and Wellness Department
and to cover as many areas as possible within
the health authority on a continuing basis as
per identified priorities.
Utilizing information and experiences gained
from this project: This project has created a
wealth of information about risk factors
associated with specific occupations within
the acute care setting. Report findings and
recommendations will be further com-
municated within the authority. As the
recommendations from the individual
assessments are implemented, any that can
be transferred to other facilities (such as
training and information and work process
changes developed) will be communicated
and disseminated authority-wide, for example
by e-mail to division Directors and by posting
on department specific intranet pages.
Continued evaluation: There will be
continued evaluation and follow-up of the
recommendations made, recommendations
implemented, and cost/benefit analyses. The
database developed for the project will be
invaluable for these analyses. In addition, the
Workplace Safety and Wellness incident
database will continue to be a complete and
efficient resource for evaluating current
strategies and planning future ones.
In addition, there are plans for presentations and
further communication of project findings and
evaluations outside the health authority.
9.4
Acknowledgements
In closing, we would like to acknowledge the
following people and organizations for their
invaluable resources, assistance and guidance with
this project:
Workers Compensation Board of British
Columbia,
Project Steering Committee members, with
representatives from Workers Compensation
Board of British Columbia, Fraser Health
Authority (Workplace Safety and Wellness
staff), the Hospital Employees Union
(HEU), the British Columbia Nurses Union
(BCNU), the Health Sciences Association
(HSA), the British Columbia Government
and Service Employees Union (BCGEU),
Joint Occupational Safety and Health
Committee members at LMH,
the entire staff of Langley Memorial
Hospital in Langley, British Columbia,
and many, many ergonomics colleagues who
have provided expertise, assistance and input
into the process, tools and final report.
Appendix
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority iii
Table 1: Ergonomics Risk Assessment Project Plan and Timeline
ACTIVITY DETAILS
ESTIMATED
TIMELINE
ACTUAL
TIMELINE
1 Fact Gathering
Meet with internal and external
resources; review literature and
web sites; establish job list; finalize
project plan; communicate project
information to staff
Feb. 2001
Mar. 2001
as stated
2
MSI incident
analysis
Review 3 years of data to establish
prioritized listing of job/tasks for risk
assessment and to establish
baseline statistics for comparison
purposes
Feb. 2001
Mar. 2001
Feb. 2001
July 2001
3
Develop risk
assessment
forms
Review existing tools and
symptom surveys; gather input
from committees; develop risk
assessment forms; conduct trials
with forms
Apr. 2001
May 2001
July 2001
4
Develop risk
assessment
process
Document process for conduct of
risk assessments; gather input from
committee members
Apr. 2001
May 2001
Sept. 2001
5
Develop risk
assessment
database
Determine inputs and outputs;
provide information to database
developer
May 2001
June 2001
May 2001-
Sept. 2001
6
Conduct risk
assessments
Conduct job observations for
identification of risks; document
findings; document controls
immediately implemented (120
assessments)
May 2001
May 2002
May 2001
July 2002
7
Perform analysis
of risk
Conduct assessment of risk factors
identified
May 2001
May 2002
May 2001
July 2002
8
Establish
recommendations
Develop recommendations with
input from department
May 2001
May 2002
May 2001
July 2002
9
Report on
outcomes
Finalize risk assessment reports
and project report
May 2001
July 2002
as stated
10
Continued
monitoring
Continued follow-up on status;
perform re-assessments as
required
ongoing as stated
11
Communicate
results
Communicate project initiatives and
results to LMH staff
ongoing as stated
Appendix A
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority iv
Figure 1:
Ergonomics Risk Assessment Project Plan and Timeline (Estimated vs. Actual)
PROJECT
ACTIVITY
Feb-
Mar
01
Apr-
May
01
Jun-
Jul
01
Aug-
Sep
01
Oct-
Nov
01
Dec-
Jan
02
Feb-
Mar
02
Apr
May
02
Jun-
Jul
02
Legend:
Estimated
Actual
1 Fact gathering
2
MSI statistical
analysis
3
Develop risk
assessment forms
4
Develop risk
assessment process
5 Develop database
6
Conduct risk
assessments
7
Perform risk
analyses
8
Establish
recommendations
9 Report on outcomes
10 Continued monitoring
11 Communicate results
Appendix A
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority v
Overexertion -
material handling
17%
Fall on same level
9%
Other body motion
8%
Violence
7%
Struck by
6%
Strike against
3%
Other
12%
Overexertion - patient
handling
38%
Strain other than
back
37%
Back strain
36%
Crush, bruise
10%
Cut
4%
Other
7%
Tendonitis
6%
Brief Review of MSI Statistics in the
Healthcare Sector
The high risk of MSIs among health care workers
is well documented (OHSAH, 2001). Hospitals
and other health care facilities such as nursing
homes and psychiatric facilities, have more reported
incidences of MSIs than any other type of industry
(Evanoff et al., 1999; OHSAH, 2001; Orr, 1997;
WCB, 2000). Nursing and nursing assistant
occupations represent the majority of health care
industry claims. Other jobs within the health care
industry that have been associated with soft tissue
injuries include data entry, laundry work,
maintenance, dietary work, pharmacy work (Orr,
1997), physiotherapy (Holder et al., 1999) and
sonography (Pike et al., 1997). Patient handling has
been identified as a significant risk factor for MSIs
among health care personnel. Among types of
patient handling tasks, lifting/ transferring patients
and repositioning patients in bed are generally
perceived as the most stressful or are the most
common causes of patient-handling related injuries
(OHSAH, 2001; WCB, 2000). Back injuries and
back pain have long been acknowledged as
common MSI problems of health care
professionals along with the neck and shoulder
regions (OHSAH, 2001; J osephson et al., 1997).
In British Columbia, the health care sector accounts
for more injuries to workers than any other industry.
In 1998, the overall injury rate for health care
workers in BC was higher than the provincial
average for all industries combined (WCB, 2000).
In 1998, the WCB accepted 7,600 lost time claims
from health care workers, accounting for 376,500
days lost. The cost of these claims paid by the
WCB to health care workers totalled approximately
$39.3 million (WCB, 2000).
Appendix B
Figures B1-3 illustrate these points (charts are from
the Workers Compensation Board of BC, Health
Care Industry Focus Report on Occupational Injury
and Disease, 2000). Overexertion due to patient
handling (38%) and material handling (17%)
account for 55% of all claims. Other accident types
include fall on same level (9%), other body motion
(8%), violence (7%), struck-by (6%) and struck
against (3%).
Figure B-1: Accident types in BC health care
industry, 1994-1998
The most common injury types are strain other
than back (37%), back strain (36%), crush or bruise
(10%), tendonitis (6%), and cut (4%).
Figure B-2: Injury types in BC healthcare industry,
1994-1998
Nursing and nursing assistant occupations represent
the majority of all health care industry claims
(WCB, 2000). By occupation, the percentage of
claims is as follows: nurse aide, care aide and LPN
(34%); registered nurse (25%); food preparation
worker and kitchen worker (12%); cleaner and
housekeeper (12%); clerical job (5%).
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority vi
Appendix B
Table B-1. General MSI Statistical Findings for LMH, 1998-2000
All data is from Workplace Health and Safety database unless otherwise indicated.
Note from Table:
1 Source: WCB Claims Statistics report for LMH, 1995-1999, 5 year average for overexertion
Variable 1998 1999 2000
Incidents and musculoskeletal injuries (MSIs)
% reported incidents that are MSIs 55% 51% 55%
% lost time that are MSIs 82% 67% 77%
Cost of MSI WCB claims
% of costs that are MSI, year of incident only NA NA 89%
% of days lost that are MSI, year of incident only NA NA 91%
Avg cost per MSI WCB claim (lost time only) NA $4403
1
$3020
Avg days lost per MSI WCB claim
NA NA 22.3
Extended/Acute Facility
% of MSI incidents at extended care facilities 27% 26% 40%
% of MSI incidents at acute care facility 73% 74% 60%
Activity at time of MSI
% of MSI incidents related to patient transfer 37% 26% 25%
% of MSI incidents related to patient repositioning 10% 12% 12%
% of MSI incidents related to material handling 9% 11% 15%
% of MSI incidents related to other activities 44% 51% 48%
Occupation
% of MSI incidents for long term care aides 25% 30% 35%
% of MSI incidents for registered nurses (RNs) 26% 24% 15%
% of MSI incidents for food service workers 1% 5% 13%
% of MSI incidents for cleaners 3% 9% 9%
% of MSI incidents for licensed practical nurses (LPNs) 10% 10% 8%
% of MSI incidents related to other occupations 35% 22% 20%
Body Part Affected
% of MSI incidents to back, neck and/or shoulder 66% 64% 68%
% of MSI incidents to back only 39% 39% 32%
% of MSI incidents to neck and/or shoulder only 20% 20% 26%
% of MSI incidents to multiple sites, including back, neck or
shoulder
7% 5% 10%
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority vii
Methodology for Priorization Based on
Incident Statistics
Note: Numbers provided are for demonstration
purposes only and do not reflect actual data from
the hospital.
1. Determine the specific variables for consider-
ation in the prioritization scheme. For this
project, 6 variables were chosen as listed below.
A weighted score will be determined for each
department.
The number of variables chosen will reflect the
numbers for ranking and weighting. If there are
6 variables, they will be ranked 1-6 with the most
important variable receiving a ranking of 1 and the
least important variable receiving a ranking of 6.
2. Assign each variable a rank in terms of its
perceived importance. The most important
variable(s) will be ranked 1. The least important
variables will receive the lowest numbers
(e.g. a rank of 6 if there are 6 variables). More
than one variable may have the same rank
(if you feel they are equally important).
3. Assign each variable a weight based on its rank.
The weight is the inverse value of the rank.
4. For this example with 6 variables, the most
important variable with a rank of 1 will
receive the highest weight of 6. The least
important variable with a rank of 6 will
receive the lowest weight of 1. If two
variables have the same rank, the weighting
is divided (e.g. if there are two variables ranked
as 1, each is assigned a weight of 5.5 based
on the average of 5 and 6 values). The
following rank and weights were used for this
project:
5. Final weighted scores are calculated for each
department. Calculate the value of each var-
iable in the equation by dividing it by the
highest value of others in the group multiplied
by its weight) and the sum of these 6 numbers
becomes the final weighted score.Information
on FTE (full-time equivalents) is required by
department in order to complete the spread-
sheet.
To calculate the weighted total, which is the sum of
the 6 variables, the following equation is used.
Using Department B as our example, the weighted
total =
( ( MS I s / MA X ( MS I s ) ) * 3 . 5 ( ( L T A /
MAX(LTAs))*5.5)+((%MSI/MAX(%MSIs))*1)
+((%LTA / MAX(%LTA))*2)+((MSIperFTE/
MAX(MSIperFTE))*3.5)+( (LTAperFTE/
MAX(LTAperFTE))*5.5)
= (32/32)*3.5 + (18/18)*5.5 + (78/100)*1 + (56/
71)*2 + (.76/1.0)*3.5 + (.43/.50)*5.5
= 3.50 + 5.50 + .78 + 1.58 + 2.66 + 4.72= 18.74
Appendix B
Rank Weight
1 6
2 5
3 4
4 3
5 2
6 1
Variable Rank Weight
Number of lost time MSIs (LTA) 1 5.5
Lost time per FTE (LTA/FTE) 1 5.5
Number of MSI incidents (MSI) 3 3.5
MSI per FTE (MSI/FTE) 3 3.5
% of MSIs that are lost time
(% LTA)
5 2
% of incidents that are MSIs
(% MSI)
6 1
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority viii
Below, results are shown for our example for all departments using the above equation.
MSI LTA %MSI %LTA MSI/FTE LTA/FTE
rank 3 1 6 5 3 1
weight 3.5 5.5 1 2 3.5 5.5
Department All
reports
MSIs LTA % MSI % LTA FTEs MSI/FTE LTA/FTE
Weighted
Total
Dept B 41 32 18 78% 56% 42.20 0.76 0.43 18.74
Dept A 24 17 12 71% 71% 24.10 0.71 0.50 16.20
Dept I 7 7 3 100% 43% 7.00 1.00 0.43 12.13
Dept C 50 26 10 52% 38% 45.50 0.57 0.22 11.94
Dept E 7 5 3 71% 60% 7.20 0.69 0.42 10.91
Dept G 28 7 4 25% 57% 23.60 0.30 0.17 6.77
Dept H 5 5 1 100% 20% 9.10 0.55 0.11 5.56
Dept F 25 18 2 72% 11% 50.30 0.36 0.04 5.31
Dept J 13 10 0 77% 0% 13.00 0.77 0.00 4.56
Dept D 3 3 0 100% 0% 5.30 0.57 0.00 3.31
Appendix B
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority ix
The graphed results for the 10 departments are shown below.
Appendix B
Weighted Scores by Department
D
e
p
t
D
D
e
p
t
J
D
e
p
t
F
D
e
p
t
H
D
e
p
t
G
D
e
p
t
E
D
e
p
t
C
D
e
p
t
I
D
e
p
t
A
D
e
p
t
B
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
10.00
11.00
12.00
13.00
14.00
15.00
16.00
17.00
18.00
19.00
20.00
Department
W
e
i
g
h
t
e
d
S
c
o
r
e
sModerate Priority
Low Priority
High Priority
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority x
Workers Compensation Board of British
Columbia Occupational Health and Safety
Regulation; Ergonomics (MSI) Require-
ments.
The purpose of sections 4.46 to 4.53 is to eliminate
or, if that is not practicable, minimize the risk of
musculoskeletal injury to workers.
Note: The WCB provides publications to assist with
implementing the Ergonomics (MSI) Requirements:
Preventing Musculoskeletal Injury (MSI): A Guide
for Employers and Joint Committees provides a
seven-step process to assist with the application of
the ergonomics requirements along with procedures
to investigate incidents of MSI and a table of
common control measures.
Understanding the Risks of Musculoskeletal
Injury (MSI) is intended to help employers with the
requirements of section 4.51 to educate workers in
risk identification, signs and symptoms of MSI, and
their potential health effects.
4.46
Definition
In sections 4.47 to 4.53 (the Ergonomics (MSI)
Requirements) musculoskeletal injury or MSI
means an injury or disorder of the muscles, tendons,
ligaments, joints, nerves, blood vessels or related soft
tissue including a sprain, strain and inflammation,
that may be caused or aggravated by work.
4.47
Risk identification
The employer must identify factors in the workplace
that may expose workers to a risk of musculoskeletal
injury (MSI).
4.48
Risk assessment
When factors that may expose workers to a riskof
MSI have been identified, the employer must ensure
that the risk to workers is assessed.
4.49
Risk factors
The following factors must be considered, where
applicable, in the identification and assessment of
the risk of MSI:
(a) the physical demands of work activities, including
(i) force required,
(ii) repetition,
(iii) duration,
(iv) work postures, and
(v) local contact stresses;
(b) aspects of the layout and condition of the work-
place or workstation, including
(i) working reaches,
(ii) working heights,
(iii) seating, and
(iv) floor surfaces;
(c) the characteristics of objects handled, including
(i) size and shape,
(ii) load condition and weight
distribution, and
(iii) container, tool and equipment
handles;
(d) the environmental conditions, including cold
temperature;
Appendix C - 1
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xi
(e) the following characteristics of the organization
of work:
(i) work-recovery cycles;
(ii) task variability;
(iii) work rate.
4.50
Risk control
(1) The employer must eliminate or, if that is not
practicable, minimize the risk of MSI to work-
ers.
(2) Personal protective equipment may only be
used as a substitute for engineering or administ-
rative controls if it is used in circumstances in
which those controls are not practicable.
(3) The employer must, without delay, implement
interim control measures when the introduction
of permanent control measures will be
delayed.
4.51
Education and training
(1) The employer must ensure that a worker who
may be exposed to a risk of MSI is educated
in risk identification related to the work, includ-
ing the recognition of early signs and symptoms
of MSIs and their potential health effects.
(2) The employer must ensure that a worker to be
assigned to work which requires specific mea-
sures to control the risk of MSI is trained in
the use of those measures, including, where
applicable, work procedures, mechanical aids
and personal protective equipment.
4.52
Evaluation
(1) The employer must monitor the effectiveness
of the measures taken to comply with the
Ergonomics (MSI) Requirements and ensure
they are reviewed at least annually.
(2) When the monitoring required by subsection
identifies deficiencies, they must be corrected
without undue delay.
4.53
Consultation
(1) The employer must consult with the joint
committee or the worker health and safety
representative, as applicable, with respect to the
following when they are required by the
Ergonomics (MSI) Requirements:
(a) risk identification, assessment and control;
(b) the content and provision of worker
education and training;
(c) the evaluation of the compliance measures
taken.
(2) The employer must, when performing a risk
assessment, consult with
(a) workers with signs or symptoms of MSI,
and
(b) a representative sample of the workers who
are required to carry out the work being
assessed.
Appendix C - 1
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xii
Appendix C - 2
Overall Risk Assessment Process
STEP
INPUT/SOURCES OF INFORMATION
1. IDENTIFICATION
Injury/incident statistics
Employee symptom survey
Meetings and discussions with
employees
Job observations of workers performing
tasks
Workstation and work area
measurements
Review of documentation (e.g. job
description, work procedures)
Checklists
2. ASSESSMENT
Review of work measurements
Comparison with ergonomics guidelines
and standards
Compilation of information from surveys,
job observations, employee discussions
Review of existing controls, controls
implemented and those that can be
implemented
3. CONTROL
C
O
N
S
U
L
T
A
T
I
O
N
Review existing controls
Document controls immediately
implemented
Recommend appropriate and practical
controls
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xiii
Identify department or work area to contact
for risk assessment.
Priority for ergonomics (MSI) risk assessment has
been assigned using a weighting scheme from a 3-year
review of incidents at LMH (See Section 2.0).
1
Contact designated person for department to
introduce the project and determine
appropriate time and duration for job
observations.
Designated contact list has been pre-established.
Ask contact person to identify all occupations
and/or work areas for review (if appropriate).
Describe participatory nature of the project,
employees and other resources (e.g. Rehab,
supervisors, JOSH Committee members) may
assist with the assessment.
2
Send memo explaining the project to the
contact person and ask that this information
be communicated to staff prior to the
assessments taking place.
Include a copy of the MSI Employee Symptom Survey
(Appendix C-4) for information. Surveys may be
completed prior to the risk assessments.
3
Send department-specific MSI incident
analysis report to the contact person.
Department-specific MSI incident analysis report (see
Section 2.2.4.2) will provide an overview of where MSI
injuries are occurring in the department, as well as
providing a comparison with LMH statistics.
4
If appropriate, meet with department
contact name and employee representatives
prior to the onset of risk assessments.
Meeting can be conducted to review Risk Assessment
Process (Flow Chart, Appendix C-3a) and forms,
review symptom survey, establish employee team to
assist and/or determine specific tasks to be reviewed.
This step is likely to occur with larger departments
and/or more complex tasks.
5
Collect and review background information
on department and occupations.
For example, job descriptions and/or list of duties,
work processes and procedures, research studies,
nursing manuals, MSIP program information,
equipment inventory etc. Establish preliminary task
list using Task Analysis Worksheet (Appendix C-5).
6
Distribute employee symptom survey to staff.
Collect completed forms and compile results.
Employee Symptom Survey (Appendix C-4) contains
questions related to MSI awareness, psychosocial
factors, body discomfort and severity, identification of
problem tasks and suggestions for improvement.
7
Appendix C - 3a
Ergonomics (MSI) Risk Assessment Process Flow Chart
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xiv
Appendix C - 3a
Repeat from Step 8. Revised December 4, 2001
Conduct job observations: observe
(shadow) a minimum of two employees
conducting the job tasks, if available.
Measure and record information as
appropriate (e.g. written notes,
measurements, photos, video).
Use worksheets (See Appendices C-7 to C-11) and
measurement/observation equipment (e.g. force
gauge, camera, tape measure).
Introduce and explain project to employees. Ask if
they have any questions.
Request that symptom survey forms be completed.
If possible, review symptom surveys during the
observation period. Determine if workers have
indicated signs/symptoms and if there are additional
tasks for review.
8
Compile findings and document risk
identification and assessment in draft in final
report format.
9
Review, document and recommend
appropriate control measures.
Identify and assess risk factors using checklists and
worksheets (Appendices C-7 Ergonomic Risk Factor
Identification Worksheet, C-8 General Ergonomics
Risk Checklist, C-9 Office Ergonomics Checklist, C-10
Manual Material Handling Checklist, C-11 Patient
Handling Checklist.
10
Review findings of the risk assessment (in
draft), including recommendations with
contact person and others as appropriate.
Review completed Sample Final Report form
(Appendix C-6):
Agree on proposed risk controls, including control
of immediate hazards.
Assign responsible person for each recommended
control.
11
.
Revise and issue final risk assessment report
to department contact person.
Ask contact name and/or team members to assist
in the communication as appropriate (e.g. e-mail
summaries, short report, posters etc).
Information is entered into database.
12
After pre-determined time frame, request
update from contact person and/or team
members regarding the status and
effectiveness of recommended controls.
Request specific information on status of controls and
if not implemented, indicate reasons why.
13
Re-evaluate to determine if controls have
been effective.
Suggestions: Review incident statistics, absenteeism
reports, WCB costs, re-issue symptom survey.
14
Re-assess as necessary.
For example, if incidents or WCB reports indicate
review is necessary, if job tasks change, if new
equipment is introduced.
15
Using Sample Final Report form (Appendix C-6):
Review existing controls.
Document controls immediately implemented.
Recommend appropriate and practical controls.
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xv
Appendix C - 3b
Department Specific Risk Assessment Process with Consultation
STEP Description of Step Consultation
1
Identify department or work area to
contact based on prioritization.
The weighting scheme for prioritization
(based on a 3-year review of MSI
incidents) was reviewed for input with
Steering Committee and JOSH.
I
D
E
N
T
I
F
I
C
A
T
I
O
N
2
Contact designated person (to
describe project, establish job
observation times, identify
occupations and/or work areas).
Department list and contact names
were finalized with assistance from
Senior Leadership Team.
3
Send memo explaining the project to
contact person. Request that this
information be communicated to staff.
Employees were invited to direct
questions or comments on the project
to Steering Committee or JOSH
Committee members (names provided).
I
D
E
N
T
I
F
I
C
A
T
I
O
N
4
Send department specific MSI
incident analysis information to
contact person to provide an
overview of MSI injuries (e.g.
occupations, tasks, type of injury,
body part injured).
Final MSI incident report and sample
department specific reports were
reviewed for input and finalized with
Steering Committee and JOSH via e-
mails and monthly meetings.
Department specific reports are
available on request.
5
If appropriate, meet with department
prior to the onset of risk
assessments.
Department employees were provided
with an overview of the project, and
their participation was encouraged.
6
Collect and review background
information (e.g. job descriptions, list
of duties, work processes and
procedures etc.) Use information to
establish a preliminary task list.
Draft task analysis worksheets or task
lists were reviewed for input with
department employees.
I
D
E
N
T
I
F
I
C
A
T
I
O
N
7
Distribute employee symptom survey
to staff. Collect completed forms and
compile results.
Survey content was reviewed for input
and finalized with Steering Committee
and JOSH.
All employees were encouraged to fill
out survey (various communication
vehicles were used).
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xvi
Appendix C - 3b
A
S
S
E
S
S
M
E
N
T
9
Compile findings of the risk
identification steps and document in
final draft format describing risk
factors identified, and including an
assessment/evaluation of their
severity.
10
Review existing controls, document
controls immediately implemented
and recommend appropriate and
practical controls.
C
O
N
T
R
O
L
11
Review findings of the risk
assessment report including
recommendations with contact
person and others as appropriate.
Process for risk assessment and
development of controls was reviewed
for input with Steering Committee and
JOSH.
A listing of occupations to assess and
their status (e.g. complete, draft, not
started) was provided to Steering
Committee and JOSH.
It was communicated that specific
assessments are available on request.
Suggested controls were reviewed with
department staff as appropriate.
Draft final report was reviewed with
contact person and input from staff was
encouraged.
12
Revise and issue final risk
assessment report. Ask contact
person to communicate report to staff
(e.g. post report, discuss at group
meetings etc.).
Steering Committee and JOSH were
updated as to recently completed
reports.
Contact person was requested to
communicate findings to staff.
13
After pre-determined time frame,
request update from contact person
and/or team member regarding status
and effectiveness of recommended
controls.
Steering Committee and JOSH were
provided with progress reports as to
status of controls, including monthly
review of implemented controls.
E
V
A
L
U
A
T
I
O
N
14
Re-evaluate to determine if controls
have been effective (e.g. look at
incident statistics, absenteeism
reports, WCB costs, re-issue
symptom survey).
Process (means) for re-evaluation and
findings of re-evaluation to be reviewed
with Steering Committee and JOSH.
15
Re-assess as necessary (e.g. if
incident or WCB reports indicate
further review is necessary, if job
tasks change, if new equipment is
introduced).
Repeat from Step 8.
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xvii
Appendix C - 4
Employee MSI Symptom Survey
This survey is anonymous. Please do not include your name. The information will be used to determine potential ergonomics
(MSI) risk factors in your work setting and provide an opportunity for you to indicate problem areas and make suggestions for
improvements.
1. Date: ____________________________________________________________________
2. Department or Work Area: ___________________________________________________
3. Occupation: _______________________________________________________________
4. Hours worked on average: Per week: ___________________ Per shift: _______________
5. How often do you work overtime?
Never Seldom Sometimes Always
6. Experience in THIS occupation:
Less than 3 months 3 months to 1 year Greater than 1 year to 5 years
Greater than 5 years to 10 years Greater than 10 years
7. Have you received any training on musculoskeletal injuries (MSIs or strains/sprains) with this employer?
YES NO
8. What are the signs and symptoms of musculoskeletal injury (e.g. strains/sprains)?
_____________________________________________________________________________________
_____________________________________________________________________________________
9. What should you do if you experience any signs or symptoms of musculoskeletal injury (e.g. strain/sprain)?
_____________________________________________________________________________________
_____________________________________________________________________________________
10. Are you aware of risk factors in your workplace that may put you at risk of musculoskeletal injury (e.g. strain/sprain)? If yes,
please describe.
_____________________________________________________________________________________
_____________________________________________________________________________________
11. Please circle the appropriate number for each statement. Consider both mental and physical aspects of your job.
strongly
disagree disagree undecided agree strongly agree
a. I have freedom to decide how I do my work. 1 2 3 4 5
b. I have a lot to say about what happens on my job. 1 2 3 4 5
c. My job is very hectic. 1 2 3 4 5
d. I have enough time to get the job done. 1 2 3 4 5
e. It is very hard to keep up with my workload. 1 2 3 4 5
f . There are always deadlines to meet. 1 2 3 4 5
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xviii
Appendix C - 4
12. Have you had any recurring pain or discomfort during the last year?
YES NO
13. If yes, place an X on the drawing in the area(s) that you feel discomfort. For any area that you mark, rank the level of discomfort on
a scale from 1 to 5. Place the numbers on the drawing beside the corresponding X.
1 = slight discomfort 2 3 4 5 = severe pain
14. For each area marked, what do you think causes the pain or discomfort?
____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
15. What job task or tasks that you perform are the most difficult or most in need of changing, and why?
____________________________________________________________________________________
____________________________________________________________________________________
b. What do you suggest can be done?
____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
16. What other suggestions or ideas do you have for improving your workstation or work area?
____________________________________________________________________________________
____________________________________________________________________________________
If you have additional comments, please provide them on the back of this sheet.
Thank you for filling in this survey!
Return to LMH Workplace Health and Safety
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xix
Appendix C - 5
Ergonomic (MSI) Risk Factor Identification and Assessment
Ergonomics Risk Assessment Project
Department/Work Area: Occupation:
Specific Location: Contact Name:
Assessed By: Assessment Date:
Task Analysis Worksheet
Job Summary:
Where possible, transfer list of job tasks from job description onto this sheet. Determine whether ergonomics
(MSI) risk assessment is required, if no, provide rationale.
Tasks and Description of Activities Frequency/Duration
Risk Assessment
Required?
TOTAL
100%
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xx
Appendix C - 6
Ergonomic (MSI) Risk Factor Identification and Assessment
Sample final report
Ergonomic (MSI) Risk Factor Identification and Assessment
Ergonomics Risk Assessment Project
Department/Work Area: Medical Unit Occupation: LPN Medical Unit
Specific Location: 4
th
floor, South Tower LMH Contact Name: Department Manager
Assessed By: Assessor Assessment Date: December 2001
Task Analysis Worksheet
Job Summary: Performs nursing procedures such as sterile dressings in addition to patient care duties relating
to feeding, personal hygiene and transporting patients.
Where possible, transfer list of job tasks from job description onto this sheet.Determine whether ergonomics
(MSI) risk assessment is required, if no, provide rationale.
Tasks and Description of Activities Frequency/Duration
Risk Assessment
Required?
1. Report: sit and discuss patient information,
current happenings, changes, family information
hour 45 min.
No
Discussion only
2. Conduct rounds for personal care: bathing,
dressing, getting patients up or back to bed,
getting patients ready to send to appointments,
assisting with toileting needs
Takes approximately 1-2 hours
each, typically done 2-3 times
per shift
Yes
3. Perform nursing procedures such as changing
dressings, catheterizations, taking/recording blood
pressure, temperature and pulse.
As required per shift; 9-10
patients per LPN
Yes
4. Assist with patient handling; repositioning in bed
reported to be problematic
As required; number per shift
varies
Yes
5. Assist patients with meals such as serving and
collecting meal trays and feeding designated
patients.
Takes approximately 1.0 hours,
typically done 2 times per shift
Yes
6. Chart patient information.
15-30 minutes per shift; may be
sporadic or completed all at
once
Yes
TOTAL 100%
E
r
g
o
n
o
m
i
c
s
(
M
u
s
c
u
l
o
s
k
e
l
e
t
a
l
)
R
i
s
k
A
s
s
e
s
s
m
e
n
t
F
r
a
s
e
r
H
e
a
l
t
h
A
u
t
h
o
r
i
t
y
x
x
i
Department/Work Area: Medical Unit Occupation: LPN Medical Unit
Specific Location: 4
th
floor, South Tower LMH Contact Name: Department Manager
Assessed By: Assessor Assessment Date: December 2001
Description of workstation: Medical unit with nursing station. Patients in single or 4-bed rooms, with 3 isolation rooms, 3 designated palliative care rooms.
Hours of Work/Shift Schedule: 4 South is currently staffed 0730 - 1930 with LPNs. Shifts are 6.5 or 10.5 hours.
Discomfort noted on surveys: neck, shoulder, elbow, lower back, leg/knee, foot
Tasks for Ergonomics Risk Assessment (from Task Analysis worksheet): Frequency of Task:
1. Conduct rounds for personal care.
2. Perform nursing procedures such as changing dressings and checking vital signs.
3. Assist with patient handling, including repositioning in bed.
4. Assist patients with meals.
5. Chart patient information.
2-4 hours per shift
as required
as required
2 hours per shift
hour per shift
25-35%%
varies
varies
20-25%
10%
Task Risk Factors Freq/Dur Mag/Range Assessment / Observations / Comments
Awkward
posture
(reaching,
bending,
twisting)
Total time
per round is
1-2 hours,
about 15-
30
min/patient
Neck >20
0
Shoulder 20-90
0
Elbow 0-60
0
and >100
0
Wrist >15
0
Trunk 20-60
0
+
Various hygiene-related duties with patients including
bathing, dressing and toileting.
Awkward postures including reaching, bending, and
twisting to access, adjust and position patient and to see.
Problems reported with commodes (broken, brakes not
working)
Patient can be asked to assist as possible. Bed height
should be adjusted, side rails down to improve posture.
Awkward
posture
Force
Up to 2
baths/shift
As above Tub does not adjust in height. Tub chair is crank-style.
I
D
E
N
T
I
F
I
C
A
T
I
O
N
Conduct
rounds for
personal
care
Force As above Varies
depending on
weight of the
limb
A
S
S
E
S
S
M
E
N
T
Force required when supporting limbs, amount varies
depending on patient characteristics.
Pillows can be used as additional supports.
Night tables are difficult to move as they have only 2
wheels with casters.
Risk Factors to consider:
q Joint posture: wrist,
elbow, shoulder, neck,
back, knees
q Awkward posture:
reach, twist, bend,
stoop, squat, climb,
static
q Force: lift, lower, carry,
push/pull, pinch or
power grip, surface
q Repetition, frequency,
duration, exposure
q Object weight, location,
size, shape, handles,
stability
q Work height, layout,
seating, space
q Tool/equipment use
q Contact Stress
q Environment: layout,
flooring, temp., noise,
light, glare, vibration
q Work Organization:
recovery, schedule,
workload, task
variability, pace, PPE
use, interruptions
q Psychosocial variables
q Other
Ergonomic (MSI) Risk Factor Identification and Assessment
A
p
p
e
n
d
i
x
C
-
6
E
r
g
o
n
o
m
i
c
s
(
M
u
s
c
u
l
o
s
k
e
l
e
t
a
l
)
R
i
s
k
A
s
s
e
s
s
m
e
n
t
F
r
a
s
e
r
H
e
a
l
t
h
A
u
t
h
o
r
i
t
y
x
x
i
i
A
p
p
e
n
d
i
x
C
-
6
Department/Work Area: Medical Unit Occupation: LPN Medical Unit
Specific Location: 4
th
floor, South Tower LMH Contact Name: Department Manager
Assessed By: Assessor Assessment Date: December 2001
Task Risk Factors Freq/Dur Mag/Range Assessment / Observations / Comments
Rounds
(continued)
Static posture As above Typically 1-2
minutes
Static posture required when supporting limbs.
Quick stretches to relieve static positioning are recommended.
Awkward
posture
(reaching,
bending,
twisting)
As required Neck >20
0
Shoulder 20-
90
0
Elbow 0-60
0
and >100
0
Wrist >15
0
Trunk 20-60
0
+
Including changing dressings and checking vital signs.
Optimize postures by adjusting bed height and lowering side rails to reduce
reaching, asking patients to reposition themselves to assist.
Force As required Not measured Amount of force will vary depending on task and patient characteristics.
Perform
nursing
procedures
Static posture As required Up to 1 minute Depending on nature of task, static positioning may be required.
Quick stretches after tasks are recommended.
I
D
E
N
T
I
F
I
C
A
T
I
O
N
Patient
handling
including
repositioning
in bed
Awkward
posture
(shoulder,
elbow, trunk)
As required Trunk 20-60
0
Shoulder 45-
90
0
Elbow 0->100
0
A
S
S
E
S
S
M
E
N
T
The number and type of transfers varies from shift to shift.
Key points: staff can optimize posture by adjusting bed height to appropriate
position (and use Trendelenberg position), lowering bed rails and getting
help from other staff. Instruct patient to ensure they are aware of the transfer
and count so that the move is done at the same time by both (or all) staff
involved.
Deficiencies with some transfers observed; primarily with repositioning in bed
(e.g. count not synchronized, incorrect body mechanics, reliance on upper
body muscles).
Comments on beds (from 2 staff): brakes are hard to access, dont know if
the brakes are on, rails are hard to put up. Prior to bed purchase, there was
a review of various models and input from various hospital staff.
Patient assessments are conducted by RNs or Rehab, can be re-assessed
by Rehab at the request of the RNs or LPNs. Staff should be reminded of
this, as well as provided with tips for patient assessment.
Ergonomic (MSI) Risk Factor Identification and Assessment
E
r
g
o
n
o
m
i
c
s
(
M
u
s
c
u
l
o
s
k
e
l
e
t
a
l
)
R
i
s
k
A
s
s
e
s
s
m
e
n
t
F
r
a
s
e
r
H
e
a
l
t
h
A
u
t
h
o
r
i
t
y
x
x
i
i
i
Ergonomic (MSI) Risk Factor Identification and Assessment
Department/Work Area: Medical Unit Occupation: LPN Medical Unit
Specific Location: 4
th
floor, South Tower LMH Contact Name: Department Manager
Assessed By: Assessor Assessment Date: December 2001
Task Risk Factors Freq/Dur Mag/Range Assessment / Observations / Comments
Patient
handling
including
repositioning
in bed
(continued)
Force As required No measured Forces vary depending on nature of transfer or reposition, patient
characteristics, staff available.
Equipment available reported by staff to be adequate: some beds are
equipped with monkey bars; 1 Arjo Maxi lift with 3 slings (one each size), and
2 Saras.
Assist patients
with meals
Awkward
posture
Static posture
- 1 hour
per shift
Neck 0-20
0
Shoulder 20-
45
0
, >90
0
Elbow 60-
>100
0
Trunk 20 -
60
0
+
Static postures may be assumed when feeding.
Working postures can be optimized by possibly alternating between sitting
and standing or choosing the best posture relative to the patient, getting as
close as possible to the patient to reduce joint angles associated with
reaching, and adjusting bed position.
Additional various upper extremity work required to serve and collect trays,
and prepare food (e.g. open beverages, put jam on toast, peel eggs etc).
I
D
E
N
T
I
F
I
C
A
T
I
O
N
Chart patient
information
Awkward
posture
15-30
minutes per
shift
Individual
charts < 2 kg
Neutral
postures,
seated
A
S
S
E
S
S
M
E
N
T
Charting can be done at various times throughout the shift or completed all at
once.
Patient charts (binders) are filed in a circular storage, above shoulder reach
to access if seated (charts sit in slots, middle is 113 cm high).
Nursing station: adjustable chairs available (adjustable height and backrest)
to allow for adjusting working postures. Seated counter height is 77 cm,
standing counter height is 116 cm. No concerns noted.
A
p
p
e
n
d
i
x
C
-
6
E
r
g
o
n
o
m
i
c
s
(
M
u
s
c
u
l
o
s
k
e
l
e
t
a
l
)
R
i
s
k
A
s
s
e
s
s
m
e
n
t
F
r
a
s
e
r
H
e
a
l
t
h
A
u
t
h
o
r
i
t
y
x
x
i
v
Ergonomic (MSI) Risk Factor Identification and Assessment
Department/Work Area: Medical Unit Occupation: LPN Medical Unit
Specific Location: 4
th
floor, South Tower LMH Contact Name: Department Manager
Assessed By: Assessor Assessment Date: December 2001
*Control Priority Note: 1 = recommended for implementation to reduce risk factors; 2 = optional, for consideration as a means of reducing risk factors; 3 = not
for immediate action but for future consideration as appropriate.
Risk Factor Potential Cause Recommended Controls Control
Priority*
Responsible
Person
Status
(May 2002)
Static
posture
Rounds,
nursing
procedures
1. Sample stretching exercises will be provided. 1 Name Not complete
2. MSIP training (4-hour sessions) are available and all staff should be
encouraged to attend. New staff are scheduled to attend, and
sessions are available for existing staff. Sessions provide practical
demonstrations and hands-on opportunities for various transfers.
1 Name Ongoing
3. Schedule awareness campaigns on a regular basis (bi-monthly).
Include topics as identified from the risk assessment. Posters,
handouts and statistical information to be provided.
What to do when patient has fallen
Initial patient assessment tips (e.g. ongoing determination of what
type of transfer is appropriate) and when and how to request
reassessment
Key tips for optimizing posture (e.g. adjusting bed height, lowering
side rails, asking patient to assist, neutral postures)
Correct use of transfer belts
Bed repositioning tips: e.g. adjust bed height, lower rails,
Trendelenberg position, ask for assistance, coordinated counting
1 Name Implemented
May 2002;
first MSIP
Minute was
on initial
patient
assessment
Awkward
posture
Static
posture
Force
Patient
transfers and
repositioning,
nursing
procedures,
rounds
Emphasis on
repositioning in
bed
4. Specific to bed repositioning: Trial slide sheet and request employee
feedback on their use.
1 Name Trials started
5. Check on existing commodes and request maintenance (reported that
some are broken and the brakes do not work) or investigate purchase
of new ones.
1 Name Complete;
new
commodes
purchased
Awkward
posture
Force
Rounds,
toileting,
washing
6. Consider replacing the legs on the night tables with casters (check
with Maintenance). This would make it easier to move the tables
around within the working area.
2 Name Not complete
C
O
N
T
R
O
L
S
Awkward
posture
Force
Patient
handling
7. For purchases, continue to ensure that staff have input (as was done
with the new beds) and request possible trials with the equipment to
ensure it will meet the needs of the unit.
1 Name Ongoing
A
p
p
e
n
d
i
x
C
-
6
E
r
g
o
n
o
m
i
c
s
(
M
u
s
c
u
l
o
s
k
e
l
e
t
a
l
)
R
i
s
k
A
s
s
e
s
s
m
e
n
t
F
r
a
s
e
r
H
e
a
l
t
h
A
u
t
h
o
r
i
t
y
x
x
v
Ergonomic (MSI) Risk Factor Identification and Assessment
Department/Work Area: Medical Unit Occupation: LPN Medical Unit
Specific Location: 4
th
floor, South Tower LMH Contact Name: Department Manager
Assessed By: Assessor Assessment Date: December 2001
Additional Comments:
For long term planning, consider a tub that is height adjustable with a pneumatic chair for patient handling. This will reduce awkward postures and forces
associated with bathing patients. Consider ceiling lifts for future budgets. Vendor information to be provided.
Thank you for the opportunity to review the work area. If you have any questions regarding this report, please contact the assessor (contact information
provided).
A
p
p
e
n
d
i
x
C
-
6
E
r
g
o
n
o
m
i
c
s
(
M
u
s
c
u
l
o
s
k
e
l
e
t
a
l
)
R
i
s
k
A
s
s
e
s
s
m
e
n
t
F
r
a
s
e
r
H
e
a
l
t
h
A
u
t
h
o
r
i
t
y
x
x
v
i
A
p
p
e
n
d
i
x
C
-
7
Ergonomic (MSI) Risk Factor Identification and Assessment
Department/Work Area: Occupation:
Specific Location: Contact Name:
Checklist Completed By: Date:
Force Awkward Posture ACTIVITY Frequency
L
i
f
t
i
n
g
P
u
s
h
/
P
u
l
l
O
t
h
e
r
B
e
n
d
i
n
g
T
w
i
s
t
i
n
g
R
e
a
c
h
i
n
g
O
t
h
e
r
O
t
h
e
r
Static
Positions
(>30 sec)
Other Risks
(e.g. contact
stress,
repetition,
layout,
environment)
Causes / Comments
Risk factors to consider: object awkward? stable? bending or twisting? adequate space to move? beds adjustable? adjusted?
heavy lifting? appropriate handles? stooping or squatting? slippery floors? handling aids available?
forceful pushing or pulling? pinch/power grip required? reaching out or up? brakes work? accessible? clutter in aisle ways?
long carry distance? working height appropriate? prolonged (static) posture? rails adjust? accessible? doorways wide enough?
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xxvii
Appendix C - 8
Department/Work Area: Occupation:
Specific Location: Contact Name:
Checklist Completed By: Date:
Use this sheet as a prompter. A no response indicates a potential risk factor/problem that may require investigation.
General Ergonomics Risk Factor Checklist Yes No Comments
Policies and Procedures
Are MSIP policies and procedures in place?
Is incident reporting and investigation in place?
Do staff members know how to report an injury or unsafe
condition?
Is management supportive and involved in health and
safety program initiatives?
Consultation Processes
Is communication with employees conducted by e.g.
meetings, bulletin boards, in-service sessions?
Are consultative channels available through workplace
committees?
Education and Training
Is there an education and training strategy for MSIP in
place?
Is MSI awareness information/training available to all
employees?
Is MSIP training available on orientation?
Is MSIP job-specific training available?
Is MSIP refresher and in-service training available?
Hazard Identification and Risk Control Strategies
Is incident information captured in a database?
Are incident statistics analyzed to identify trends?
Are follow-up activities conducted to ensure implementation
and evaluate effectiveness of controls?
Are risk assessments conducted based on priority needs
including risk factor identification, assessment and
recommendation of controls?
Equipment and Building Design
Is there adequate mechanical equipment available for use?
Is equipment in good working order?
Is there a process for equipment repair in place and is it
effective, including identifying and tracking?
Are staff aware of process for equipment repair?
Is there a process for routine equipment maintenance?
Is there adequate space to store equipment?
Do purchases include stakeholder feedback prior to
purchase? e.g. maintenance, housekeeping
Are design changes reviewed prior to implementation?
Evaluation, Review and Promotion
Is MSIP information regularly promoted (e.g. newsletters,
staff bulletins, intranet postings and presentations)?
Are ergonomics program initiatives regularly reviewed to
evaluate effectiveness?
Are risk controls implemented regularly reviewed to
evaluate effectiveness?
General Ergonomics Risk Factor Checklist
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xxviii
Department/Work Area: Occupation:
Specific Location: Contact Name:
Checklist Completed By: Date:
Use this sheet as a prompter. A no response indicates a potential risk factor/problem that may require investigation.
Office Ergonomics Checklist Yes No Comments
Awkward Posture
Are feet supported by the floor or a footrest?
Is the lower back supported by the backrest?
Are chair adjustment features functioning and does the
employee know how to adjust them?
Are the keyboard and monitor in front and aligned?
Are the keyboard and mouse at seated elbow height?
Does the keyboard angle allow for neutral wrist posture?
Are the keyboard supports or feet down?
Is the mouse at the same height and beside the keyboard?
Is the monitor about arms length away?
Is the top line of print about seated eye level?
If using bifocals, is neutral neck positioning maintained?
Is a document holder or desk slant used if necessary?
Is cradling the handset between ear and shoulder avoided?
Is a headset used if necessary?
Force
Is minimal force used on keyboard and mouse?
Is the mouse moved with the whole arm, with the
movement initiated at the shoulder?
Are the muscles relaxed and in a neutral position?
Repetition and Static Posture
Are adequate pauses taken?
Is the work self-paced?
Is there flexibility around the performance of tasks?
Are tasks completed using both hands?
Contact Stress
Is the seat pan cushioned with a rounded edge?
Is there clearance between the front edge of the seat pan
and the back of the legs?
Are the arm rests positioned slightly below elbow level and
used for periods of non-activity only?
Is a wrist rest available and used appropriately?
Are the forearms not resting on the desk edge?
Environment
Are lighting levels appropriate?
Is the screen free of reflected glare? (e.g. angled down
slightly, curtains used, controls adjusted)
Is additional task lighting used if necessary?
Are other environmental aspects appropriate (e.g. noise,
temperature)?
Work Layout and Work Organization
Are frequently used resource materials and equipment
within easy reach and easy to access?
Is the underside of the desk free of clutter?
Are desk top materials organized to maximize space and
minimize clutter?
Are changes in posture made throughout the day?
Is sitting for long periods of time avoided by varying tasks?
Are stretching exercises conducted?
Office Ergonomics Checklist
Appendix C - 9
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xxix
Manual Material Handling Checklist
Department/Work Area: Occupation:
Specific Location: Contact Name:
Checklist Completed By: Date:
Use this sheet as a prompter. A no response indicates a potential risk factor/problem area that may require further
investigation.
Manual Material Handling Checklist Yes No Comments
Object/Load Characteristics
Have excessive weights been reduced?
Have excessive push/pull forces been reduced?
Can the load be made smaller or lighter?
Are objects easy to grasp?
Are the objects stable?
Are handholds or handles available?
Handling Characteristics
Are objects handled infrequently/short duration?
Is repetition avoided by job rotation or task variety?
Are there sufficient rest pauses?
Are materials moved over minimum distances?
Are ramps designed appropriately?
Can the objects remain close to the body?
Are working heights appropriate or adjustable?
Are movements between knee and shoulder height?
Is handling from a seated position avoided?
Are static positions avoided?
Are twisting motions avoided?
Are bending or stooped motions avoided?
Is excessive forward, backward or side reaching
avoided?
Is help available for heavy or awkward lifts?
Equipment
Are lifting devices including carts and trolleys
available and used whenever possible?
Is equipment in good working condition?
Is there a preventive maintenance program for
equipment?
Is faulty equipment tagged and reported?
Environment
Are the floors clean, dry, even and well lit?
Is the work area uncluttered and free of obstacles?
Is there enough room to maneuver?
Administration/Organization
Do staff wear appropriate clothing and footwear?
Are staff trained in the use of available equipment?
Are staff trained in correct material handling
procedures?
Do staff follow correct procedures?
Do staff know how to report an injury or unsafe
condition?
Are difficult lifts discussed with supervisor and co-
workers?
Other:
Other:
Other:
Appendix C - 10
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xxx
Department/Work Area: Occupation:
Specific Location: Contact Name:
Checklist Completed By: Date:
ACTIVITY CHECKLIST Freq? Difficult? Comments
Repositioning in bed side to side
Repositioning up in bed
Repositioning in chair
Holding/supporting whole body
Holding/supporting extremities
Transfer bed to chair
Transfer bed to stretcher
Transfer bed to walker
Transfer bed to commode
Transfer bed to bath
Transfer chair to stretcher
Transfer chair to walker
Transfer chair to commode
Transfer chair to toilet
Other transfer:
Other transfer:
Other transfer:
Transport in stretcher
Transport in wheelchair
Transport in bed
Assisting with ambulation
Bathing in bed
Bathing in bath room
Feeding
Changing clothing
Changing in bed
Picking patients up from floor
Weighing a patient
Moving patient with mechanical lift
Moving mechanical lift only
Moving carts (e.g. linen, food)
Moving equipment (e.g. monitors)
Moving furniture (e.g. tables)
Making occupied bed
Making unoccupied bed
Handling laundry bags
Handling food trays
Restocking supplies
Replacing O2 tanks on stretchers
Changing IV bags
Wound care/changing dressings
Dispensing medications
Taking vitals
Other:
Risk factors to consider heavy lifting? appropriate handles? rails adjust? accessible?
bending or twisting? forceful pushing or pulling? working height appropriate? beds adjustable? adjusted?
stooping or squatting? long carry distance? adequate space to move? handling aids available?
reaching out or up? pinch/power grip required? slippery floors? clutter in aisle ways?
prolonged (static) posture? object awkward? stable? brakes work? accessible? doorways wide enough?
Patient Handling Checklist
Appendix C - 11
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xxxi
Patient Handling ChecklistCont.
ADMINISTRATIVE/ORGANIZATION CHECKLIST Yes No Comments
MSIP Policies and Procedures
Is incident reporting and investigation in place?
Is MSI awareness information/training available?
Are MSIP policies and procedures in place?
Is MSIP patient handling training in place?
Is MSIP patient handling training comprehensive?
Does MSIP patient handling training include hands-on
practice and competency measures?
Have staff attended MSIP patient handling training in the
last 2 years?
Have staff been shown how to use mechanical
equipment?
Can Physiotherapy staff can be called upon to provide
additional guidance on ward?
Mobility Assessment
Is initial mobility assessment conducted on admission?
Is there a process for mobility re-assessment in place
and effective?
Are staff aware of process for re -assessment?
Is mobility information written on ADL card and/or patient
care plan?
Is appropriate mobility logo posted at bedside?
Patient/Resident Handling
Are patient/resident assessments immediately prior to
the transfer conducted?
Are patients/residents encouraged to assist?
Are recommended handling procedures and techniques
used by staff?
Is the bed height adjusted and side rails lowered?
Do staff use a standard starting sign for transfers?
Are difficult transfers discussed with supervisors and co-
workers?
Equipment
Is there adequate mechanical equipment and slings
(supplementary checklist available)?
Is equipment in good working order (e.g. brakes, wheels,
adjustable beds)?
Is there a process for equipment repair in place and is it
effective, including identifying and tracking?
Are staff aware of process for equipment repair?
Is there a process for routine equipment maintenance in
place?
Is there adequate space to store equipment?
Do equipment purchases include user feedback prior to
purchase?
Environment
Are hallways and rooms uncluttered and free of
obstacles?
Is there enough room to maneuver?
Other
Is workload distributed equally among employees or
shifts?
Do staff know how to report an injury or unsafe
condition?
Is communication with employees conducted by
meetings, bulletin boards, in-service sessions?
Appendix C - 11
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xxxii
RISK ASSESSMENT STANDARDS AND
GUIDELINES
The following is a listing of available standards and
guidelines for ergonomics risk assessment.
Risk Identification and Assessment
ACGIH threshold limit values for physical
hazards The American Conference of
Governmental Industrial Hygienists (ACGIH),
Thresholds Limit Values for Chemical Substances
and Physical Agents in the Work Environment, and
Biological Exposure Indices (TLVs and BEIs),
including Hand Activity Level (HAL) tool for
measuring upper extremity activity. Available for
purchase at the ACGIH web site at www.acgih.org.
ANSI S3.34-1986 (R1997) Hand Arm Vibration
Standards American National Standard Guide
for the Measurement and Evaluation of Human
Exposure to Vibration Transmitted to the Hand.
ANSI S3.34-1986 (R1997). Available for purchase
at the ANSI web site at www.web.ansi.org/
default.htm.
ANSI Draft Ergonomics Checklist ANSI
(1996). American national standard: control of
work-related cumulative trauma disorders. Part I:
upper extremities. New York, NY: American
National Standards I nstitute, Z-365-1996.
Unpublished draft.
CSA Office Ergonomics CSA Z412 Guideline
on Office Ergonomics, 2000, available from CSA
International www.csa-international.org
Caution zone jobs J obs where an employees
typical work activities include any of the specific
physical risk factors identified in Washington State
WAC 296-62-05105 Appendix B. These jobs have
a sufficient degree of risk to require ergonomics
awareness education and job hazard analysis.
Available from www.1ni.wa.gov/ wisha.
ErgoWeb Fitting the J ob to the Worker: An
ergonomics program guideline http:/ / ergoweb.com
/ resources/ reference/ guidelines/ fittingjob.cfm
US Department of Energy ErgoEASER
Ergonomics Education, Awareness, System
Evaluation and Recording (ErgoEASER) software
package. US Department of Energy, Office of
Environment, Safety, and Health (1995). Can be
downloaded from the Department of Energy web
site at www.tis.eh.doe.gov/ others/ ergoeaser/
download.htm.
GM UAW Risk Factor Checklist UAW GM
Ergonomics Risk Factor Checklist RFC2, United
Auto Workers General Motors Centre for
Human Resources, Health and Safety Centre, 1998.
Copies available from UAW GM Centre for
Human Resources, Health and Safety Centre, 1030
Doris Road, Auburn Hills, MI 48326.
Job Strain Index The Strain Index: A proposed
method to analyze jobs for risk of distal upper
extremity disorder, Moore, J .S. and A. Garg, (1995).
Published in American I ndustrial Hygiene
Association J ournal, volume 56, pages 443-458.
Web site at http:/ / sg-www.satx.disa.mil/ hscoemo/
tools/ strain.htm for a web-based version of this
tool.
NIOSH Lifting Equation, 1991 Waters, T.R.,
Putz-Anderson, V., Garg, A., and Fine, L.J . (1993).
Revised NI OSH equation for the design and
evaluation of manual lifting tasks. Published in
Ergonomics, volume 36 (7), pages 749-776. For a
manual on using the lifting equation see:
Application Manual for Revised Lifting Equation,
Appendix C - 12
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xxxiii
Waters, T., Putz-Anderson, V., Garg, A. (1994).
Available from the National Technical Information
Centre (NTIS), Springfield, VA 22161.
Calculator available from Healthcare Benefit
Trust, Vancouver BC.
Calculator web site at :
www.industrialhygiene.com/calc/lift.htm.
Application guideline web site at
www.cdc.gov/niosh/94-110.html
NIOSH Elements of Ergonomics Programs, 1997
US Department of Health and Human Services,
Public Health Service, Centres for Disease Control
and Prevention, National Institute for Occupational
Safety and Health. Publication No. 97-117.
Available at www.cdc.gov/niosh/homepage.html.
Ovako Working Posture Analysis System (OWAS)
OWAS provides a method for evaluating postural
load during work. OWAS assigns the evaluated
posture a rating that indicates the urgency of taking
corrective measures to reduce the postures potential
to expose workers to injury. For more information
on OWAS, visit the Tampere University of
Technology web site at http://turva.me.tut.fi/owas/
.
Rapid Entire Body Assessment tool (REBA)
Hignett, S. and McAtamney, L. (2000) Rapid entire
body assessment (REBA). Published in Applied
Ergonomics volume 31, pages 201-205.
Copies available from Elsevier Science,
www.elsevier.com.
Rapid Upper Limb Assessment (RULA)
McAtamney, L and Corlett, E.N. (1993) RULA: A
survey method for the investigation of work-related
upper limb disorders. Published in Applied
Ergonomics, volume 24 (2), pages 91-99. Copies
available from Elsevier Science, www.elsevier.com.
RULA contains a handy one-page worksheet that is
great for establishing joint posture ranges with
comparison to neutral ranges.
Snook Push/Pull Hazard Tables Snook, S.H. and
Ciriello, V.M., (1991) The design of manual
handling tasks: revised tables of maximum
acceptable weights and forces. Published in
Ergonomics, 1991 34(9), pages 1197-1213. You may
obtain a copy from Taylor & Francis,
www.tandf.co.uk/journals.
Task Analysis Kirwan and Ainsworth (1992). A
Guide to Task Analysis. Taylor and Francis,
London. This book reviews many methods of task
analysis and is specifically geared to practical
techniques. A large proportion of the book is about
industrial case studies.
WCB of BC MSI Booklets The WCB provides
publications to assist with implementing the
Ergonomics (MSI) Requirements. Preventing
Musculoskeletal Injury (MSI): A Guide for Employers and
Joint Committees provides a seven-step process to
assist with the application of the ergonomics
requirements along with procedures to investigate
incidents of MSI and a table of common control
measures. Understanding the Risks of Musculoskeletal
Injury (MSI) is intended to help employers with the
requirements of section 4.51(1) to educate workers
in risk identification, signs and symptoms of MSI,
and their potential health effects. Information and
publications available at www.worksafebc.com.
Appendix C - 12
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xxxiv
Risk Control
National Safety Council, 1988 - Making the J ob
Easier An ergonomics idea book. National Safety
Council, 1121 Spring Lake Drive, Itasca, IL 60143-
3201.
NIOSH Elements of Ergonomics Programs, 1997
US Department of Health and Human Services,
Public Health Service, Centres for Disease Control
and Prevention, National Institute for Occupational
Safety and Health. Publication No. 97-117.
Available at www.cdc.gov/ niosh/ homepage.html.
WCB of BC MSI Booklets The WCB provides
publications to assist with implementing the
Ergonomics (MSI ) Requirements. Preventing
Musculoskeletal Injury (MSI): A Guidefor Employers
and J oint Committees provides a seven-step process
to assist with the application of the ergonomics
requirements along with procedures to investigate
incidents of MSI and a table of common control
measures. Understanding theRisks of Musculoskeletal
Injury (MSI) is intended to help employers with the
requirements of section 4.51(1) to educate workers
in risk identification, signs and symptoms of MSI,
and their potential health effects. Information and
publications available at www.worksafebc.com.
Appendix C - 12
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xxxv
Ergonomics Risk Assessment Project
7/17/02
Assessment Date: 12/1/01 Assessment Type: Ergonomics (MSI)
HSA: Langley Health Site: LMH Dept: LMH - 4 SOUTH Occup: LPN Year: 2001
Contact Name: RV Assessed By:DH Shift: variable
Employees Observed:
Job Summary: Performs nursing procedures such as sterile dressings in addition to patient care duties relating to feeding, personal
hygiene and transporting patients.
Task Conduct rounds Frequency/Duration: occasional Risk Assessment
Required
Task Long: Conduct rounds for personal care: bathing, dressing, Freq/Duration text: 1-2 hours each round,
getting patients up or back to bed, getting patients ready to typically done 2-3 times
send to appointments, assisting with toileting needs per shift
Identification:
Risk Factors Freq/Duration Mag/Range AssessmentObservations/Comments Freq Code
awkward posture 1-2 hours total neck > 20 Various hygiene-related duties with patients O
shoulder 20-90 including bathing, dressing and toileting.
Part Code Body Part elbow 0-60 Awkward postures including reaching, bending,
HA Hand/Wrist/Fingers wrist >15 and twisting to access, adjust and position patient
LB Lower Back trunk 20-60 and to see tasks.
Problems reported with commodes (broken, brakes
NE Neck not working)
SH Shoulder Patient can be asked to assist as much as
ELB Elbow possible. Bed height should be adjusted with side
rails down to improve posture.
force as above varies Force required when supporting limbs, amount V
varies depending on patient characteristics.
Pillows can be used as additional supports.
Night tables are difficult to move as they have only
2 wheels with casters.
static posture typically 1-2 Static posture required when supporting limbs. O
minutes Quick stretches to relieve static positioning are
recommended.
Recommendations:
Risk Factor Potential Cause Recommended Controls Person Date
static posture rounds, nursing Sample stretching exercises will be provided. DH 7/31/02
procedures
Comments: Status: Outstanding
Ctl Code: Information/handout
awkward rounds, toileting Check on existing commodes and request maintenance (reported RV 7/31/02
posture, force that some are broken and the brakes do not work) or investigate
purchase of new ones.
Comments: New commodes have been purchased and are in use. Status: Implemented
Ctl Code: Major equipment
awkward rounds, toileting, Consider replacing the legs on the night tables with casters (check RV 7/31/02
posture, force washing with Maintenance). This would make it easier to move the tables
around within the working area.
Comments: Status: Outstanding
Ctl Code: Maintenance
Ergonomic (MSI) Risk Factor Identification and Assessment
Sample Database Report
Appendix D
E
r
g
o
n
o
m
i
c
s
(
M
u
s
c
u
l
o
s
k
e
l
e
t
a
l
)
R
i
s
k
A
s
s
e
s
s
m
e
n
t
F
r
a
s
e
r
H
e
a
l
t
h
A
u
t
h
o
r
i
t
y
x
x
x
v
i
Appendix D-2: Ergonomics Risk Assessment Project Status of Recommendations
ID Assessment Site, department, occupation Job Summary 07/31/02
15 01-Dec-01 LMH, LMH - 4 SOUTH, LPN Performs nursing procedures such as sterile dressings in addition to patient care
duties relating to feeding, personal hygiene and transporting patients.
Task Short: Conduct rounds for personal care Task Long: Conduct rounds for personal care: bathing, dressing, getting patients up or back to bed,
getting patients ready to send to appointments, assisting with toileting needs
Counter Risk Factor Potential Cause Recommendations Status Date Control Code Control Status
51 static posture rounds, nursing procedures Sample stretching exercises will be 7/31/02 Information/ Outstanding
provided. handout
Counter Risk Factor Potential Cause Recommendations Status Date Control Code Control Status
52 awkward posture, force rounds, toileting Check on existing commodes and request 7/31/02 Major Implemented
maintenance or investigate purchase of new. capital
Counter Risk Factor Potential Cause Recommendations Status Date Control Code Control Status
53 awkward posture, force rounds, toileting, washing Consider replacing the legs on the night 7/31/02 Maintenance Outstanding
tables with casters to make it easier to move
the tables around the work area.
38 Task Short: Perform nursing procedures Task Long: Perform nursing procedures such as changing dressings, catheterizations,
taking/recording blood pressure, temperature and pulse.
Counter Risk Factor Potential Cause Recommendations Status Date Control Code Control Status
54 awkward posture, force patient handling, For purchases, continue to ensure that 7/31/02 Work Existing
repositioning, staff have input (as with the new beds)
moving beds and request possible trials to ensure it will
meet the needs of the unit.
39 Task Short: Assist with patient handling Task Long: Assist with patient handling; repositioning in bed reported to be problematic
Counter Risk Factor Potential Cause Recommendations Status Date Control Code Control Status
55 awkward posture, patient transfers and repositioning MSIP training (4-hour sessions) are 7/31/02 Training In progress
static posture, available and all staff should be
force encouraged to attend. Sessions include
practical demonstrations and hands-on
opportunities for various transfers.
Counter Risk Factor Potential Cause Recommendations Status Date Control Code Control Status
56 awkward posture patient transfers and repositioning Schedule awareness campaigns on a 7/31/02 Information/ In progress
static posture regular basis (bi-monthly). Include handout
force suggested topics as identified from the
risk assessment.
Counter Risk Factor Potential Cause Recommendations Status Date Control Code Control Status
57 awkward posture patient transfers and repositioning Specific to bed repositioning: Trial slide 7/31/02 Minor Outstanding
static posture sheet and request employee feedback on
force their use.
E
r
g
o
n
o
m
i
c
s
R
i
s
k
A
s
s
e
s
s
m
e
n
t
P
r
o
j
e
c
t
S
t
a
t
u
s
o
f
R
e
c
o
m
m
e
n
d
a
t
i
o
n
s
A
p
p
e
n
d
i
x
D
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xxxvii
Workplace Health and Safety
POLICY
The South Fraser Health Region is committed to
promoting a safe and healthy workplace for all
employees. One of our goals is to minimize the
risk of injury to all employees, physicians,
volunteers and the general public. By providing
appropriate facilities, equipment, training,
education, procedures and performance standards,
we will effectively manage workplace health and
safety risks inherent to healthcare and exceed
regulatory requirements.
All employees, physicians and volunteers will
actively participate in the elements of the
Workplace Health & Safety Program to ensure that
all work is performed in a safe manner.
PROCEDURES
Executive Team and Senior Leadership Teams
will:
Ensure that all levels of management are
accountable for workplace health and safety
performance in their area of responsibility.
Initiate the development of health and safety
goals and objectives and review annually.
Ensure that health and safety concerns are
addressed in all aspects of strategic planning.
Managers and Supervisors will:
Develop and implement safe work
procedures.
Provide adequate direction and instruction to
employees in the safe performance of their
duties.
Ensure appropriate education is provided to
staff so that work is performed in accordance
with established safety standards and
practices.
Conduct quality accident investigations to
determine the causes of work related injuries
and to recommend corrective actions to
eliminate the hazard.
Consider health and safety factors in their
decision-making process.
Employees, Physicians and Volunteers will:
Follow all health and safety requirements
according to WCB Occupational Health and
Safety Regulations and the Regions policies
and procedures.
Report all unsafe acts and/ or conditions.
Workplace Health & Safety Department will:
Provide consultation, education and subject
matter expertise to guide compliance with
regulatory and workplace standards in safety
and health.
Coordinate, develop and implement the
Regions Workplace Health & Safety
Program according to Regional requirements
and applicable legislation.
Joint Occupational Health & Safety Committee
will:
Promote safe work practices and working
conditions by raising awareness through
various activities.
Assist in creating a safe place of work by
recommending corrective measures to
management.
Approved by: Executive Team
Appendix E
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xxxviii
NO MANUAL LIFT POLICY
THE SOUTH FRASER HEALTH REGION IS COMMITTED TO MINIMIZING THE RISK OF INJURY TO STAFF AND PATIENTS/
RESIDENTS THROUGH ENGINEERING CONTROLS.
THE SOUTH FRASER HEALTH REGION RECOGNIZES THE PHYSICAL RISKS ASSOCIATED WITH MANUALLY LIFTING,
TRANSFERRING OR REPOSITIONING PATIENTS/RESIDENTS.
NO MANUAL LIFTING OF PATIENTS/RESIDENTS* SHALL BE PERFORMED BY SOUTH FRASER HEALTH REGION STAFF, EXCEPT
IN LIFE THREATENING SITUATIONS.
All patients/residents shall be assessed for their ability to weight bear prior to any
attempt by staff to transfer and/or ambulate, except in life threatening conditions.
A mechanical lift shall be used when any patient/resident is unable to weight bear.
* In the case of infants and small children, where the use of a mechanical lift may be
unsafe, the lift method shall be assessed on an individual basis.
MUSCULOSKELETAL INJURY PREVENTION PROGRAM
NO MANUAL LIFT POLICY
Appendix E
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xxxix
Summary Of Recommendations From Risk Assessments
Variable
Totals or
Average
Individual
computer
workstations
Multi-user
computer
workstations
Material
handling
Patient
Handling
Number of reports reviewed 100 20 20 25 35
Average number of
recommendations per report
6 4 6 6 6
Type of Recommendations
% of recommendations
related to training, including
providing written materials
31% 40% 23% 26% 36%
% of recommendations
related to work process
33% 31% 37% 38% 28%
% of recommendations
related to maintenance
8% 4% 10% 8% 8%
% of recommendations
related to minor capital
expense (< $2000)
24% 25% 29% 26% 16%
% of recommendations
related to major capital
expense (> $2000)
4% 0% 1% 2% 12%
Total 100% 100% 100% 100% 100%
Status of Recommendations
% of recommendations that
are complete
45% 86% 78% 36%
20%
(+16% in
progress)
% of recommendations that
are on capital list
2% 0% 0% 1% 6%
% of recommendations that
are not complete
53% 14% 22% 63% 58%
Total 100% 100% 100% 100% 100%
Costs of Recommendations
% of reports with total costs
of $0
26% 25% 25% 28% 26%
% of reports with total costs
of < $500
46% 75% 74% 44% 21%
% of reports with total costs
of $500-2000
9% 0% 0% 16% 7%
% of reports with total costs
of > $2000
19% 0% 1% 12% 46%
100% 100% 100% 100% 100%
Appendix F - 1
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xl
Project Outcomes: Percent Change in Pre-Project Values vs. Post-Project Values
All data was derived from Workplace Health and Safety database.
Variable
PRE-PROJECT
(Baseline
2000)
POST-PROJECT
(Upon project
completion)
% change
Frequency
1
and severity
2
rates
Frequency rate for all incidents +10%
Severity rate for all incidents -28%
Frequency rate for MSIs only +2%
Severity rate for MSIs only -43%
Costs of WCB claims
WCB direct claims costs all incidents -34%
WCB direct claims costs MSIs only -44%
Average cost per MSI WCB claim (lost time only) $3020 $1809 -40%
Average days lost per MSI WCB claim
22.3 12.1 -46%
% of costs that are MSI, year of incident only 89% 75% -15%
% of days lost that are MSI, year of incident only 91% 74% -19%
Incidents and MSIs
% reported incidents that are MSIs 55% 51% -7%
% lost time that are MSIs 77% 72% -6%
Extended/Acute Facility
% of MSI incidents at extended care facilities 40% 20% -50%
% of MSI incidents at acute care facility 60% 80% +33%
Activity at time of MSI
% of MSI incidents related to patient transfer 25% 13% -48%
% of MSI incidents related to patient repositioning 12% 13% +8%
% of MSI incidents related to material handling 15% 21% +40%
% of MSI incidents related to other activities 48% 53% +10%
Occupation
% of MSI incidents for long term care aide 35% 24% -31%
% of MSI incidents for RNs 15% 27% +80%
% of MSI incidents for food service workers 13% 11% -15%
% of MSI incidents for cleaners 9% 7% -22%
% of MSI incidents for LPNs 8% 7% -12%
% of MSI incidents related to other occupations 20% 24% +20%
Body Part Affected
% of MSI incidents to multiple sites, including back,
neck or shoulder
10% 19% +90%
% of MSI incidents to back only 32% 18% -44%
% of MSI incidents to neck and/or shoulder only 26% 10% -61%
% of MSI incidents to other body parts 32% 53% +65%
1
Frequency rate: (Number of lost time incidents * 100) / number of FTEs
2
Severity rate: (Number of days lost (per SFVHR) *100) / number of FTEs
Appendix F - 2
Ergonomics (Musculoskeletal) Risk Assessment
Fraser Health Authority xli
Appendix F - 3
FOLLOW-UP SURVEY FOR MANAGERS
Ergonomics Risk Assessment Project at LMH
Thank you for taking time to complete this survey! The information will be used to evaluate the ergonomics
project at LMH and make improvements to the process for future risk assessments that are conducted at
facilities throughout the health authority.
1. Date: ____________________________________________________________________
2. Department (optional): _______________________________________________________
3. Were you aware that an ergonomics risk assessment project was taking place at LMH and within your
department?
YES NO
4. Are you aware of any changes made in YOUR department as a result of this project?
YES NO
If yes, please list examples:
____________________________________________________________________________________
____________________________________________________________________________________
5. Are you aware of any changes made in OTHER departments as a result of this project?
YES NO
If yes, please list examples:
____________________________________________________________________________________
____________________________________________________________________________________
6. Do you feel that this was a worthwhile project for your department and staff?
YES NO
7. Do you feel that this was a worthwhile project for LMH?
YES NO
8. What did you like about the project or what do you think worked well?
____________________________________________________________________________________
____________________________________________________________________________________
9. Do you have any suggestions as to how the project and process could have been improved?
____________________________________________________________________________________
____________________________________________________________________________________
10. Additional comments (please use the back if more room is required):
____________________________________________________________________________________
Thank you for completing this survey!
Please return to Workplace Safety and Wellness, LMH
Useful Web Sites
References
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xlv
Useful Web Sites
ASSTSAS
Association for health and safety in the workplace,
social affairs sector,
http://www.asstsas.qc.ca/english/default.asp
Bernard, Bruce, B., M.D., M.P.H. (Ed.).
Musculoskeletal Disorders (MSDs) and Workplace
Factors. A Critical Review of Epidemiologic Evidence
for Work-Related Musculoskeletal Disorders of the
Neck, Upper Extremity, and Low Back. From NIOSH
http://www.cdc.gov/niosh/ergosci1.html
California OSHA
A Back Injury Prevention Guide for Health Care
Providers. From Cal/OSHA
http://www.dir.ca.gov/DOSH/
dosh_publications/index.html
Canadian Centre for Occupational Health &
Safety
http://www.ccohs.ca
European Agency for Safety and Health at
Work
http://agency.osha.eu.int/
Garg, Arun. (1999)
Long-Term Effectiveness of Zero-Lift Program in
Seven Nursing Homes and One Hospital.
From University of Wisconsin web site:
http://ergonomics.uwm.edu/zero-lift_report.pdf
Government of Western Australia
Strategies To Reduce The Risk Of Back Strain In
Nursing Homes. Available from web site:
http://www.safetyline.wa.gov.au/pagebin/
pg001136.htm
Health Care Health and Safety Association of
Ontario.
Resource guides:
http://www.hchsa.on.ca
National Institute for Occupational Safety and
Health, NIOSH,
http://www.cdc.gov/niosh/homepage.html
National Occupational Health and Safety
Commission, Commonwealth of Australia
http://www.nohsc.gov.au
National Research Council,
Panel on Musculoskeletal Disorders and the
Workplace, Commission on Behavioral and
Social Sciences and Education. Musculoskeletal
Disorders and the Workplace: Low Back and
Upper Extremities. From National Academies
Press:
http://www.nap.edu/books/0309072840/html/
index.html
Occupational Health and Safety Agency for
Healthcare in British Columbia, OHSAH,
http://www.ohsah.bc.ca
Occupational Safety and Health
Administration, OSHA,
U.S. Department of Labour, Hospital E-Tool
http://www.osha-slc.gov/SLTC/hospital_etool/
index.html and Nursing Home eCAT
http://www.osha-slc.gov/SLTC/
nursinghome_ecat/ergo/ergo.html
Occupational Safety and Health Service of the
Department of Labour, New Zealand
http://www.osh.dol.govt.nz
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xlvi
Patient Safety Center of Inquiry, Tampa
Florida.
www.patientsafetycenter.com
Prevention Dynamics, Portal for Ontario
Health and Safety Associations
http://www.preventiondynamics.com
U.S. Department of Health and Human
Services, Public Health Service, Centres for
Disease Control and Prevention, National
Institute for Occupational Safety and Health.
Publication No. 97-117. Elements of Ergonomics
Programs, A Primer Based on Workplace Evaluations
of Musculoskeletal Disorders. Available from NIOSH
http://www.cdc.gov/niosh/ephome2.html
Washington State Department of Labour and
Industries.
Washington State WAC 296-62-05105 Appendix B.
http://www.lni.wa.gov/wisha/ergo/Default.htm
Workers Compensation Board of B.C.
http://www.worksafebc.com and http://
healthcare.healthandsafetycenter.com/s/home.asp
Workplace Health Safety and Compensation
Commission of New Brunswick
http://www.whscc.nb.ca
Workplace Safety and Insurance Board,
Ontario.
http://www.wsib.on.ca/wsib/wsibsite.nsf/public/
PreventionHSSI
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xlvii
References
Ahlberg-Hulten, G.K., Theorell, T., & Sigala,
F. (1995).
Social support, job strain and musculoskeletal pain
among female health care personnel. Scand J Work
Environ Health, 21(6), 435-439.
American National Standard Institute (1996).
Draft ergonomics checklist: control of work-related
cumulative trauma disorders. Part I: upper extremities.
New York, NY: American National Standards
Institute, Z-365-1996. Unpublished draft.
Armstrong, T.J., Buckle, P., Fine, L.J.,
Hadberg, M., Jonsson, B., & Kilborn, A.,
(1993).
A conceptual model for work-related neck and
upper-limb musculoskeletal disorders. Scand J
Work Environ Health, 19(2), 73-84.
LAssociation pour la sant et la scurit du
travail, secteur affaires sociales ASSTSAS,
(1994). Moving Patient Safety Principles, English
Version of the PDSB Programme. Published by
LAssociation pour la sant et la scurit du
travail, secteur affaires sociales (ASSTSAS).
Burton, A.K., Symonds, T.L., Zinzen, E.,
Tillotson, K.M., Caboor, D., Van Roy, P., &
Clarys, J.P. (1997).
Is ergonomic intervention alone sufficient to limit
musculoskeletal problems in nurses? Occupational
Medicine, 47(1), 25-32.
Canadian Standard Association, (2000).
Guideline on Office Ergonomics, CSA Z412.
Canadian Standards Association.
Chaffin, D.B., & Andersson, G.B. (1984).
Occupational biomechanics.
New York, NY: John Wiley & Sons Inc.
Ciriello, V.M., Snook, S.H., Webster, B.S., &
Dempsey, P. (2001).
Psychophysical study of six hand movements.
Ergonomics, 44(10), 922-936.
Corlett, E.N. et al., (1994).
The Guide to Handling of Patients. IMPACC USA
in cooperation with National Back Pain
Association and the Royal College of Nursing.
Corlett, E.N., & Bishop, R.P. (1976).
A technique for assessing postural discomfort.
Ergonomics, 19(2),175-182.
Cromie, J.E., Robertson, V.J., & Best, M.O.
(2000).
Work-related musculoskeletal disorders in physical
therapists: prevalence, severity, risks, and
responses. Physical Therapy, 80(4), 336-351
Day, R., Hartman, D., & Casper, D. (2000).
Evaluation of Ergonomic and Security Toll Booth.
Workers Compensation Board of British
Columbia.
DeGusseme, L. (1995)
Langley Memorial Hospital Musculoskeletal Injury
Prevention Program Evaluation Report. Langley
Memorial Hospital MSIP Program Evaluation
Committee.
Drury, C.G., Broderick, R.L., Weidman, C.H.,
& Reynolds Mozrall, J.L. (1999).
A corporate-wide ergonomics programme:
implementation and evaluation. Ergonomics,
42(1), 208-228.
Eastman Kodak Company (1983).
Ergonomics design for people at work, New York, NY:
Van Nostrand Reinhold Company.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xlviii
Engels, J.A., van der Gulden, J.W.J., Senden,
T.F., Hertog, C.A.W.M., Kolk, J.J., &
Binkhorst, R.A. (1994).
Physical work load and its assessment among the
nursing staff in nursing homes. American College of
Occupational and Environmental Medicine, 36(3), 338-
345.
Ergoweb (2001).
Applied Workplace Ergonomics Training Course
Manual. Ergoweb Inc.
Evanoff, B.A., Bohr, P.C., & Wolf, L.D. (1999).
Effects of a participatory ergonomics team among
hospital orderlies. American Journal of Industrial
Medicine, 35, 358-365.
Feletto, Mario. (2001).
A Back Injury Prevention Guide for Healthcare
Workers. Occupational Safety and Health Associa-
tion of California.
Fernandes, C. (2000).
Measurement of Violence in the Emergency Department
and Assessment of a Strategy to Reduce Health Care
Worker Risk. Workers Compensation Board of
British Columbia.
Fosnaught, M. (1999).
Injuries on the job: PTs at risk. Magazine of
Physical Therapy, 7(4), 34-40.
Fragala, G. et al. (2001).
Patient Care Ergonomics Resource Guide: Safe Patient
Handling and Movement. Tampa: Patient Safety
Center of Inquiry, from
www.patientsafetycenter.com.
Fragala, G. (2000).
The new ergonomic program standard and work-
related injuries in health care: Part 1- Effective
ergonomic interventions in patient handling tasks.
MSIs in Health Care.
Gamble, E. (1997).
Evaluation of Interventions Developed to Prevent/
Reduce Musculoskeletal Injuries in Health Care Workers
Caused by Patient Handling. Workers Compensa-
tion Board of British Columbia.
Garg, A., & Moore, J.S. (Eds.). (1992).
Epidemiology of low back pain. Occupational
Medicine: State of the Art Reviews, 7(4), 599-608.
Gilding, E. (1996).
Reducing back injuries through the implementation of a
transfer assessment program. Workers Compensa-
tion Board of British Columbia.
Grandjean, E. (1982).
Fitting The Task to the Man. London, England:
Taylor and Francis.
Halpern, M., Hiebert, R., Nordin, M.,
Goldsheyder, D., & Crane, M. (2001).
The test-retest reliability of a new occupational
risk factor questionnaire for outcome studies of
low back pain. Applied Ergonomics, 32, 39-46.
Healthcare Benefit Trust, (2001).
Industry Report Risk Assessment Tool for Aggressive
Behaviour Management in Continuing Care Residential
Pilot Project. Vancouver: Healthcare Benefit Trust.
Healthcare Benefit Trust, (1997).
Ergonomics In Healthcare: Safe, Healthy and Effective
Workplaces, Series of modules.Vancouver:
Healthcare Benefit Trust.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority xlix
Hertzman, C., McGrail, K., & Hirtle, B.
(1999).
Summary Report of the Incidence and Prevalence of
Worker Injury and Subsequent Outcome in British
Columbia: A Record Linkage Study. Workers
Compensation Board of British Columbia.
Hignett, S. (2001).
Embedding ergonomics in hospital culture: top-
down and bottom-up strategies. Applied Ergonomics,
32, 61-69.
Hignett, S., & McAtamney, L. (2000).
Rapid entire body assessment (REBA).
Applied Ergonomics, 31, 201-205.
Holder, N.L., Clark, H.A., DiBlasio, J.M.,
Hughes, C.L., Scherpf, J.W., Harding, L., &
Shepard, K.F. (1999). Cause, prevalence, and
response to occupational musculoskeletal injuries
reported by physical therapists and physical
therapist assistants (Research Project). Physical
Therapy, 79, 7.
Jarrell, R.B. (1997).
Home care workers: Injury prevention through risk
factor reduction. Occupational Medicine: State of the
Art Reviews. Philadelphia: Hanley & Belfus, Inc.,
757-766.
Josephson, M. et al. (1997).
Musculoskeletal symptoms and job strain among
nursing personnel.Occupational and Environ-
mental Medicine, 54, 681-685.
Kalavar, S.S., Hunting, K.L. (1996).
Musculoskeletal symptoms among
cytotechnologists. Ergonomics, 27, 11.
Karasek, R., Theorell, T. (1990).
Healthy Work: Stress, Productivity and the Reconstruct-
ion of Working Life. Washington USA: Basic Books.
Karasek, R.A. (1979).
Job demands, job decision latitude and mental
strain: implications for job redesign. Administrative
Science Quarterly, 24, 285-307.
Keyserling, W.M., Stetson, D.S., Silverstein,
B.A., Brouwer, M.L. (1993).
A checklist for evaluating ergonomic risk factors
associated with upper extremity cumulative
trauma disorders. Ergonomics, 36(7), 807-831.
Kilborn, A. (1994).
Repetitive work of the upper extremity Part II: the
scientific basis (knowledge base) for the guide.
International Journal of Industrial Ergonomics, 14, 59-
86.
Kirwan & Ainsworth (1992).
A Guide to Task Analysis. London: Taylor and
Francis.
Koehoorn, M., Kennedy, S., Derners, P.,
Hertzman, C., & Village, J. (2000).
Musculoskeletal Injuries Among Health Care Workers:
Individual, Biomechanical and Work Organization
Factors. Workers Compensation Board of British
Columbia.
Kuorinka, I., Jonssen, B., Kilborn, A.,
Vinterberg, H., Biering-Sorensen, F.,
Andersson, G., & Jorgensen, K. (1987).
Standardized nordic questionnaires for the analysis
of musculoskeletal symptoms. Applied Ergonomics,
18, 233-237.
Larese, F., & Fiorito, A. (1994).
Musculoskeletal disorders in hospital nurses: a
comparison between two hospitals. Ergonomics,
37(7), 1205-1211.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority l
Loisel, P., Gosselin, L., Durand, P., Lemaire,
J., Poitras, S., Abenhaim, L. (2001).
Implementation of a participatory ergonomics
program in the rehabilitation of workers suffering
from subacute back pain. Applied Ergonomics, 53-
60.
McAtamney, L., Corlett, E.N. (1993).
RULA: a survey method for the investigation of
work-related upper limb disorders. Applied Ergo-
nomics, 24(7), 91-99.
McDiarmid, M.A., Kessler, E.R. (1997).
Occupational Medicine: The Health Care Worker.
State of the Art Reviews, 12(4), Philadelphia:
Hanley & Belfus, Inc.
Marion, S., Hertzman, C., & Ostry, A. (1999).
Reliability of Four Methods of Measuring Psychosocial
Job Strain. Workers Compensation Board of
British Columbia.
Meittunen, E.J., Matzke, K., & Sobszak S.C.
(1999).
Identification of risk factors for a challenging
ergonomic issue: The patient transfer. Journal of
Healthcare Safety, Compliance & Infection Control,
January 1999.
Moore, J.S. & A. Garg. (1995).
The strain index: A proposed method to analyze
jobs for risk of distal upper extremity disorder.
American Industrial Hygiene Association Journal, 56,
443-458.
National Safety Council. (1988).
Making the job easier an ergonomics idea book.
Itasca, IL: National Safety Council.
Neumann, W.P., Wells, R.P., Norman, R.W.,
Frank, J., Shannon, H., Kerr, M.S., the
OUBPS Working Group (2001).
A posture and load sampling approach to
determining low-back pain risk in occupational
settings. International Journal of Industrial
Ergonomics. 65-77.
NIOSH. (1981).
Work practices guide for manual materials handling.
Cincinnati, OH: U.S. Department of Health and
Human Services, Public Health Service, Centers
for Disease Control, National Institute for
Occupational Safety and Health, DHHS (NIOSH)
Publication 81-122.
NIOSH. (1997).
Bernard B, (Ed.). Musculoskeletal disorders and
workplace factors: A critical review of epidemiologic
evidence for work-related musculoskeletal disorders of
the neck, upper extremity, and low back. Second
Printing. Cincinnati, OH: U.S Department of
Health and Human Services, Public Health
Service, Centers for Disease Control and
Prevention, National Institute for Occupational
Safety and Health, DHHS (NIOSH) Publication
Number 97-141.
NIOSH, (1997).
Elements of Ergonomics Programs; A Primer Based on
Workplace Evaluations of Musculoskeletal Disorders.
US Department of Health and Human Services,
Public Health Service, Centres for Disease Control
and Prevention, National Institute for
Occupational Safety and Health. Publication No.
97-117.
Nora, K., & Imada, A.S. (1991).
Participatory ergonomics. Bristol, PA: Taylor &
Francis Inc.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority li
Nussbaum, M.A., & Torres, N. (2001).
Effects of training in modifying working methods
during common patient-handling activities.
International Journal of Industrial Ergonomics, 33-41.
Occupational Safety and Health Adminis-
tration, OHSA, (1993).
Ergonomics program management guidelines for
meatpacking plants. Washington, DC: U.S.
Department of Labor, Occupational Safety and
Health Administration, OSHA Report 3123.
Occupational Health and Safety Agency for
Healthcare in British Columbia, OHSAH
(2000).
Safe Patient & Resident Handling, Acute & Long Term
Care Sectors Handbook.
Occupational Health and Safety Agency for
Healthcare in British Columbia, OHSAH
(2001).
Musculoskeletal Injury Prevention Program;
Implementation Guide.
Orr, Gary, B. (1997).
Ergonomics Programs for Health Care Organ-
izations. Occupational Medicine: State of the Art
Reviews, 12(4), 687-799. Philadelphia: Hanley &
Bellus, Inc.
Oxenburgh, M. (1991).
Increasing productivity and profit through health and
safety. Sydney, Australia: CCH International.
Parker, G. (1999).
Back To The Future A Training Handbook.
Workers Compensation Board of British
Columbia.
Paris-Seeley, N., Eng, P., & Raschke, S. (2000).
Evaluation of portable transfer devices to reduce the risk
of musculoskeletal injury (MSI) to home care workers
and development of performance requirements for such
devices.
Pike, I., et al. (1997).
The prevalence of musculoskeletal disorders
among diagnostic medical sonographers, Journal of
Diagnostic Medical Sonography, 13(5), 219-227.
Putz-Anderson, V., Ed. (1988).
Cumulative trauma disorders a manual for muscu-
loskeletal diseases of the upper limb. Bristol, PA:
Taylor & Francis Inc.
Ridyard, D., Tapp, L., & Wylie, L. (2001).
Ergonomic job measurement system. American
Society of Safety Engineers, 29-32.
Royal College of Nursing. (1999).
Code of Practice for Patient Handling. London:
Royal College of Nursing (RCN). Re-order
number 000 604.
Royal College of Nursing. (1999).
Manual Handling Assessments in Hospitals and the
Community, An RCN Guide. London: Royal College
of Nursing (RCN). Re-order number 000 605.
Sanders, M.S., & McCormick, E.J. (1987).
Human factors in engineering and design, 6
th
ed. New
York: McGraw Hill.
Sewell, J. (1999).
Repositioning in Bed: Injury Prevention (Research
Project). Workers Compensation Board of British
Columbia.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority lii
Sewell, J. (1999).
Repositioning in Bed: Injury Prevention (Trainers
Manual). Workers Compensation Board of
British Columbia.
Snook, S.H., & Ciriello, V.M. (1991).
The design of manual handling tasks: revised
tables of maximum acceptable weights and forces.
Ergonomics, 34(9), 1197-1213.
South Fraser Health Region. (2001).
Internal memo Activities Template: Ergonomics Risk
Assessment Project, prepared by Workplace Health
and Safety, January 2001.
South Fraser Health Region. (2001).
Internal memo Investment In Workplace Safety and
Health Leadership, prepared by Workplace Health
and Safety, June 1999.
Tuohy Main, Kate (1999).
A Manual of Handling People, Implementing a
No-lift Approach, 2nd edition. New Lambton
Heights NSW Australia: Tuohy Main Pty Ltd
Waters, T.R., Putz-Anderson, V., & Garg, A.
(1994).
Applications manual for the revised NIOSH lifting
equation. Cincinnati, OH: U.S. Department of
Health and Human Services, Public Health
Service, Centers for Disease Control and Preven-
tion, National Institute for Occupational Safety
and Health, DHHS (NIOSH) Publication No. 94-
110.
Waters, T.R., Putz-Anderson, V., Garg, A., &
Fine, L.J. (1993).
Revised NIOSH equation for the design and
evaluation of manual lifting tasks. Ergonomics, 36
(7), 749-776.
Wheeler, W. (2000).
Back To Health: Musculoskeletal Injury Prevention for
Health Care Workers. Workers Compensation
Board of British Columbia.
Woodson, W.E., Tillman, B., & Tillman, P.
(1992). Human factors design handbook. 2
nd
ed. New
York, NY: McGraw Hill, Inc.
Workers Compensation Board of B.C. (2001).
Preventing musculoskeletal injury (MSI); a guide for
employers and joint committees.
Available at: www.worksafebc.com.
Workers Compensation Board of B.C. (2001).
Understanding the risks of musculoskeletal injury
(MSI), an educational guide for workers on sprains,
strains, and other MSIs.
Available at: www.worksafebc.com.
Workers Compensation Board of B.C. (2000).
Health Care Industry Focus Report on Occupational
Injury and Disease.
Workers Compensation Board of B.C., The
Secretariat for Regulation Review Board of
Governors (1994).
Draft Ergonomics Regulations and: Statement of
Context, Draft Code of Practice, Proposed
Implementation Strategy.
Workplace Health & Safety Agency, (1992).
Musculoskeletal Injuries Prevention Program (MIPP);
Participants Manual.
Workplace Safety & Insurance Board. Business
Results Through Health & Safety,
from www.wsib.on.ca/wsib/wsibsite.nsf/public/
BusinessResultsHealthSafety, 73.
Ergonomics (Musculoskeletal) Risk Assessment Project
Fraser Health Authority liii
Acknowledgements:
Project Steering Committee Members:
Warren Ballard
Representative
Hospital Employees Union
Kathy Churchill
Representative
British Columbia Nurses Union
Larry DeGusseme
Occupational Hygienist, Industry Services
Workers Compensation Board of British
Columbia
Deanna Harrison
Ergonomist, Workplace Safety and Wellness
Fraser Health Authority
Alison Hutchison
Disability Prevention Consultant, Workplace
Safety and Wellness
Fraser Health Authority
Frances Hutchison
Disability Prevention Consultant, Workplace
Safety and Wellness
Fraser Health Authority
Dave Keen
Director, Workplace Safety and Wellness
Fraser Health Authority
Stephen Symon
Industry Specialist, Industry Services - Healthcare
Workers Compensation Board of British
Columbia
Maggie Walters
Representative
British Columbia Government and Service
Employees Union
Assessment Project Report Designed by:
Gordon Jang
Media Services Technician
Fraser Health Authority
Copyright Nov. 2002
You might also like
- LAW OF ContractDocument1 pageLAW OF ContractKhurshid Manzoor Malik50% (2)
- Office ErgonomicsDocument14 pagesOffice ErgonomicsNereus90No ratings yet
- Ergonomics Engineering and Administrative ControlsDocument676 pagesErgonomics Engineering and Administrative ControlsAden Parker100% (2)
- Wonderland Audition PacketDocument5 pagesWonderland Audition PacketBritt Boyd100% (1)
- Manual Handling Assessment - RPS Floor SortingDocument5 pagesManual Handling Assessment - RPS Floor SortingBayu Aji S100% (1)
- COMPREHENSIVE Occupational Health GuideDocument102 pagesCOMPREHENSIVE Occupational Health Guidejoyc013050% (2)
- LGC Shadow Title Master - Pot: Workplace ErgonomicsDocument57 pagesLGC Shadow Title Master - Pot: Workplace ErgonomicsAlexandra BanteguiNo ratings yet
- Ergonomics, Manual Handling and Safe Lifting at WorkDocument35 pagesErgonomics, Manual Handling and Safe Lifting at WorkIke NancyNo ratings yet
- An Etymological Dictionary of The Scottivol 2Document737 pagesAn Etymological Dictionary of The Scottivol 2vstrohmeNo ratings yet
- Occupational Health and SafetyDocument13 pagesOccupational Health and SafetyVam ArmodiaNo ratings yet
- Ergonomics Risk Assessment PDFDocument2 pagesErgonomics Risk Assessment PDFVictoriaNo ratings yet
- Work Related Neck and Uper Limb Musculoeskeletal DisordersDocument117 pagesWork Related Neck and Uper Limb Musculoeskeletal Disordersakamacho84No ratings yet
- Occupational Health and SafetyDocument52 pagesOccupational Health and SafetyRamadan Rashad100% (2)
- Workplace Health and Safety Management Systems: D.I.Y GuideFrom EverandWorkplace Health and Safety Management Systems: D.I.Y GuideRating: 1 out of 5 stars1/5 (1)
- Ergonomics PDFDocument29 pagesErgonomics PDFNur KamiliaNo ratings yet
- Industrial HygieneDocument47 pagesIndustrial HygieneFatima CellonaNo ratings yet
- Noise Assessment ReportDocument29 pagesNoise Assessment ReportThupten Gedun Kelvin OngNo ratings yet
- Health and Safety BenchmarkingDocument16 pagesHealth and Safety BenchmarkingHealthSafety90% (20)
- OHSDocument203 pagesOHSsamsat76100% (4)
- Office ErgonomicsDocument29 pagesOffice ErgonomicsAshish ShahNo ratings yet
- Oocupational Health and SafetyDocument87 pagesOocupational Health and SafetyGayathri RNo ratings yet
- Nursing in Occupational HealthDocument7 pagesNursing in Occupational HealthjorgeacctNo ratings yet
- Ergonomic Workplace Design For Health, Wellness, and ProductivityDocument725 pagesErgonomic Workplace Design For Health, Wellness, and Productivitydoughstone90% (10)
- Occupational Health & Safety (OHS)Document36 pagesOccupational Health & Safety (OHS)MmeraKi100% (1)
- Sample Ergonomics Program PDFDocument18 pagesSample Ergonomics Program PDFSyv Consultores AsociadosNo ratings yet
- HSG 65 Guide To Measuring H&S Performance 2002Document30 pagesHSG 65 Guide To Measuring H&S Performance 2002venapusaNo ratings yet
- Organizational Behavior (Perception & Individual Decision Making)Document23 pagesOrganizational Behavior (Perception & Individual Decision Making)Irfan ur RehmanNo ratings yet
- Safety Committee Orientation TrainingDocument11 pagesSafety Committee Orientation TrainingAriel Peralta AdvientoNo ratings yet
- Training Program: By: Rahul AhujaDocument17 pagesTraining Program: By: Rahul Ahujakei HoinaNo ratings yet
- Easy Ergonomics A Practical Approach For Improving The WorkplaceDocument88 pagesEasy Ergonomics A Practical Approach For Improving The WorkplaceVu LeNo ratings yet
- Offi Ce Ergonomics: Practical Solutions For A Safer WorkplaceDocument73 pagesOffi Ce Ergonomics: Practical Solutions For A Safer WorkplaceManas KarnureNo ratings yet
- Office Ergonomics:: What Makes It Unique To Manage?Document15 pagesOffice Ergonomics:: What Makes It Unique To Manage?kumar21189No ratings yet
- Osha Ergonomics PDFDocument44 pagesOsha Ergonomics PDFCynthia Catherine Janacky100% (2)
- Ergonomics STDDocument51 pagesErgonomics STDRamesh Maverick100% (1)
- Manual Handling Presentation HandoutDocument22 pagesManual Handling Presentation Handoutcharbelhanna100% (2)
- BPK 180W - Office Ergonomics Evaluation - FinalDocument46 pagesBPK 180W - Office Ergonomics Evaluation - FinalShayla ShabkhizNo ratings yet
- A Comprehensive Guide To HR Best Practices You Need To Know This Year (Infographic)Document42 pagesA Comprehensive Guide To HR Best Practices You Need To Know This Year (Infographic)MALATHI MNo ratings yet
- Heat StressDocument28 pagesHeat StressDDR20140% (1)
- Ergonomics: An IntroductionDocument14 pagesErgonomics: An IntroductionsanaydhnNo ratings yet
- ILO - Fundamental Principles of OHSDocument221 pagesILO - Fundamental Principles of OHSGustavo AlcântaraNo ratings yet
- Safety Education and TrainingDocument40 pagesSafety Education and Trainingkevin punzalan100% (4)
- OhsDocument202 pagesOhsNasa Taufik AkbarNo ratings yet
- Ergonomics PresentationDocument18 pagesErgonomics Presentationapi-463810148No ratings yet
- Occupational EconomicsDocument626 pagesOccupational EconomicsVirmantas Juocevicius100% (1)
- Cement Processing Hol CimDocument1 pageCement Processing Hol CimShailesh RaneNo ratings yet
- Wrkplace Env & Ergonomics Part1Document29 pagesWrkplace Env & Ergonomics Part1Muhammad AizatNo ratings yet
- ErgonomicsDocument21 pagesErgonomicsIreneLeahC.Romero100% (1)
- Production Ergonomics Designing PDFDocument297 pagesProduction Ergonomics Designing PDFmlutfima100% (1)
- Principles of Occupational Health and Hygiene An Introduction 3rdDocument575 pagesPrinciples of Occupational Health and Hygiene An Introduction 3rdqampy100% (5)
- Quality Management GurusDocument61 pagesQuality Management GuruscleofecaloNo ratings yet
- TN Vision 2023 PDFDocument68 pagesTN Vision 2023 PDFRajanbabu100% (1)
- Gamboa Vs Chan 2012 Case DigestDocument2 pagesGamboa Vs Chan 2012 Case DigestKrissa Jennesca Tullo100% (2)
- Occupational Health And Safety A Complete Guide - 2021 EditionFrom EverandOccupational Health And Safety A Complete Guide - 2021 EditionNo ratings yet
- Safety Culture AssesmentDocument2 pagesSafety Culture AssesmentdeeNo ratings yet
- Applied Industrial Ergonomics 4.3 - tcm1038-133720Document342 pagesApplied Industrial Ergonomics 4.3 - tcm1038-133720Leardy100% (2)
- Ergonomics Survey Presentation 11 SlidesDocument11 pagesErgonomics Survey Presentation 11 Slidesanon_808484261No ratings yet
- Presentation Ergonomics Oct2010Document32 pagesPresentation Ergonomics Oct2010harshvardhan0% (1)
- Ergonomics Evaluation Methods: This Chapter ProvidesDocument22 pagesErgonomics Evaluation Methods: This Chapter ProvidesSherina Capola100% (1)
- 5.7 Occupational Health and Safety ChecklistDocument7 pages5.7 Occupational Health and Safety ChecklistRyan Jeffrey Padua Curbano100% (1)
- ErgonomicsDocument18 pagesErgonomicsbalakaleesNo ratings yet
- Certified Health And Safety Consultant A Complete Guide - 2020 EditionFrom EverandCertified Health And Safety Consultant A Complete Guide - 2020 EditionNo ratings yet
- Humidex User ManualDocument8 pagesHumidex User ManualYuli WicahyoNo ratings yet
- International Journal of Greenhouse Gas Control: ArticleinfoDocument8 pagesInternational Journal of Greenhouse Gas Control: ArticleinfoYuli WicahyoNo ratings yet
- 3 - Research Methods (Week 3)Document36 pages3 - Research Methods (Week 3)Yuli WicahyoNo ratings yet
- UROLITIASISDocument5 pagesUROLITIASISIkrima Firda MaharaniNo ratings yet
- FKK, Uitm Shah Alam Bukit Cerakah: Conducted byDocument2 pagesFKK, Uitm Shah Alam Bukit Cerakah: Conducted byYuli WicahyoNo ratings yet
- Model FineDocument34 pagesModel FineYuli WicahyoNo ratings yet
- Removing Heavy Metals From Waste WaterDocument21 pagesRemoving Heavy Metals From Waste Waterrlh2022100% (1)
- Removing Heavy Metals From Waste WaterDocument21 pagesRemoving Heavy Metals From Waste Waterrlh2022100% (1)
- Adverbs Before AdjectivesDocument2 pagesAdverbs Before AdjectivesJuan Sanchez PrietoNo ratings yet
- Apple Festival Program 2017Document3 pagesApple Festival Program 2017Elizabeth JanneyNo ratings yet
- Labor Rules English Noi Quy Bang Tieng Anh PDFDocument27 pagesLabor Rules English Noi Quy Bang Tieng Anh PDFNga NguyenNo ratings yet
- Launchy 1.25 Readme FileDocument10 pagesLaunchy 1.25 Readme Fileagatzebluz100% (1)
- Animal Welfare in Bangladesh and The Role of Obhoyaronno CaseDocument11 pagesAnimal Welfare in Bangladesh and The Role of Obhoyaronno CaseZarin Tanjim WoyshorjoNo ratings yet
- RSA ChangeMakers - Identifying The Key People Driving Positive Change in Local AreasDocument29 pagesRSA ChangeMakers - Identifying The Key People Driving Positive Change in Local AreasThe RSANo ratings yet
- PHD Thesis - Table of ContentsDocument13 pagesPHD Thesis - Table of ContentsDr Amit Rangnekar100% (15)
- DHBVNDocument13 pagesDHBVNnitishNo ratings yet
- Laboratory Methodsin ImmnunologyDocument58 pagesLaboratory Methodsin Immnunologyadi pNo ratings yet
- What Is SCOPIC Clause - A Simple Overview - SailorinsightDocument8 pagesWhat Is SCOPIC Clause - A Simple Overview - SailorinsightJivan Jyoti RoutNo ratings yet
- Undertaking:-: Prime Membership Application Form (Fill With All Capital Letters)Document3 pagesUndertaking:-: Prime Membership Application Form (Fill With All Capital Letters)Anuj ManglaNo ratings yet
- Gastric Emptying PresentationDocument8 pagesGastric Emptying Presentationrahul2kNo ratings yet
- Intro To EthicsDocument4 pagesIntro To EthicsChris Jay RamosNo ratings yet
- 40+ Cool Good Vibes MessagesDocument10 pages40+ Cool Good Vibes MessagesRomeo Dela CruzNo ratings yet
- Syllabus Biomekanika Kerja 2012 1Document2 pagesSyllabus Biomekanika Kerja 2012 1Lukman HakimNo ratings yet
- Pronouns Workshop SENADocument7 pagesPronouns Workshop SENAPaula Rodríguez PérezNo ratings yet
- W2-Prepares Feasible and Practical BudgetDocument15 pagesW2-Prepares Feasible and Practical Budgetalfredo pintoNo ratings yet
- 23 East 4Th Street NEW YORK, NY 10003 Orchard Enterprises Ny, IncDocument2 pages23 East 4Th Street NEW YORK, NY 10003 Orchard Enterprises Ny, IncPamelaNo ratings yet
- Field Assignment On Feacal Sludge ManagementDocument10 pagesField Assignment On Feacal Sludge ManagementSarah NamyaloNo ratings yet
- Mooting ExampleDocument35 pagesMooting Exampleluziro tenNo ratings yet
- Lista Agentiilor de Turism Licentiate Actualizare 16.09.2022Document498 pagesLista Agentiilor de Turism Licentiate Actualizare 16.09.2022LucianNo ratings yet
- CGP Module 1 FinalDocument19 pagesCGP Module 1 Finaljohn lexter emberadorNo ratings yet
- Sarcini: Caiet de PracticaDocument3 pagesSarcini: Caiet de PracticaGeorgian CristinaNo ratings yet