You might also like
- Congenital Talipes EquinovarusDocument3 pagesCongenital Talipes EquinovarusAgung HaryadiNo ratings yet
- J .'It Nsra"tr Kyytt: LLLSL (UslDocument1 pageJ .'It Nsra"tr Kyytt: LLLSL (UslAgung HaryadiNo ratings yet
- Who Can Provide Effective and Safe Termination of Pregnancy Care? A Systematic ReviewDocument9 pagesWho Can Provide Effective and Safe Termination of Pregnancy Care? A Systematic ReviewAgung HaryadiNo ratings yet
- Validity of Utility Measures For Women With Urge, Stress, and Mixed Urinary IncontinenceDocument6 pagesValidity of Utility Measures For Women With Urge, Stress, and Mixed Urinary IncontinenceAgung HaryadiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Perspective: New England Journal MedicineDocument3 pagesPerspective: New England Journal MedicinePatrick CommettantNo ratings yet
- Silica Awareness Toolbox TalkDocument2 pagesSilica Awareness Toolbox TalkSamar Husain0% (1)
- Josseicka Reynoso ResumeDocument1 pageJosseicka Reynoso ResumeLouis MarchiNo ratings yet
- Antifungal Catheter Lock Therapy 1Document8 pagesAntifungal Catheter Lock Therapy 1Dakota YamashitaNo ratings yet
- Treating Adult Survivors of Childhood Emotional Abuse and Neglect PDFDocument328 pagesTreating Adult Survivors of Childhood Emotional Abuse and Neglect PDFNegura Giulia100% (19)
- Du ProfessorsDocument28 pagesDu Professorsalka sharmaNo ratings yet
- Sri Mulyani PDFDocument7 pagesSri Mulyani PDFHasna RofifahNo ratings yet
- Training Impulsive Children To Talk To Themselves:: University of WaterlooDocument12 pagesTraining Impulsive Children To Talk To Themselves:: University of WaterlooSalma MedinaNo ratings yet
- His Tory of ODDocument13 pagesHis Tory of ODAmar NathNo ratings yet
- FNCP HyperacidityDocument2 pagesFNCP HyperacidityJeriel DelavinNo ratings yet
- THBHDK 15Document1 pageTHBHDK 15RGNitinDevaNo ratings yet
- Competency-Based Learning Material (Common Competency)Document45 pagesCompetency-Based Learning Material (Common Competency)ZOOMTECHVOC TRAINING&ASSESSMENT100% (1)
- Theories and Principle of Health Care EthicsDocument6 pagesTheories and Principle of Health Care EthicspeachyskizNo ratings yet
- 2022 Annual ReportDocument76 pages2022 Annual ReportLive 5 NewsNo ratings yet
- Church Reoperation Request LetterDocument2 pagesChurch Reoperation Request LetterSir Rannie EspantoNo ratings yet
- COMMENTARYDocument4 pagesCOMMENTARYAdrian CadaNo ratings yet
- First Periodical TestDocument4 pagesFirst Periodical TestSarah mae EmbalsadoNo ratings yet
- Dissertation Ideas DrugsDocument6 pagesDissertation Ideas DrugsBuyPapersOnlineForCollegeUK100% (1)
- Article HealthDocument3 pagesArticle Healthkaii cutieNo ratings yet
- Rubber Band Ligation: of HaemorrhoidsDocument1 pageRubber Band Ligation: of HaemorrhoidsdbedadaNo ratings yet
- The Different Types of InsomniaDocument5 pagesThe Different Types of InsomniaDavid WillNo ratings yet
- Managerial Skill Development Unit-3Document44 pagesManagerial Skill Development Unit-3Arif QuadriNo ratings yet
- CNS Stimulants: College of Pharmacy Department of PharmacologyDocument20 pagesCNS Stimulants: College of Pharmacy Department of PharmacologyDrDeepak PrasharNo ratings yet
- Assessment and Treatment of Spasticity: Cori Ponter, PT, MPT, NCS Barrow Neurological Institute 3/23/19Document76 pagesAssessment and Treatment of Spasticity: Cori Ponter, PT, MPT, NCS Barrow Neurological Institute 3/23/19Praneetha100% (2)
- Count To Ten Allowing YourselfDocument1 pageCount To Ten Allowing YourselfwisgeorgekwokNo ratings yet
- Anila 8611Document18 pagesAnila 8611Anila zafarNo ratings yet
- Rchl1pdf PDF CompressDocument111 pagesRchl1pdf PDF CompressCristian CiocoiuNo ratings yet
- School Based Immunization Form Grade 1Document1 pageSchool Based Immunization Form Grade 1maristellaNo ratings yet
- Professional SummaryDocument3 pagesProfessional SummaryVijay LS SolutionsNo ratings yet
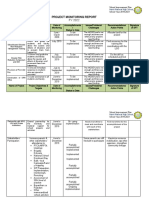
- Project Monitoring Report. GovernanceDocument6 pagesProject Monitoring Report. GovernanceJASMIN FAMANo ratings yet