You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Hilton Head Relocation GuideDocument50 pagesHilton Head Relocation GuidebernardhhiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Julie Toon Pawley ResumeDocument1 pageJulie Toon Pawley Resumebernardhhi100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Nancy Toon Duchess ArticleDocument8 pagesNancy Toon Duchess ArticlebernardhhiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Bigriver Playbill ScribdDocument6 pagesBigriver Playbill ScribdbernardhhiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Footloose Playbill FinalDocument6 pagesFootloose Playbill Finalbernardhhi100% (3)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Heroes On Horseback Summer 08 NewsletterDocument2 pagesHeroes On Horseback Summer 08 NewsletterbernardhhiNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Forest Beach Condo Detail PagesDocument7 pagesForest Beach Condo Detail PagesbernardhhiNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
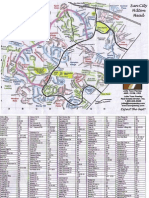
- Sun City Hilton Head Street Map-JTPDocument2 pagesSun City Hilton Head Street Map-JTPbernardhhi100% (3)
- JanFeb 08 WebDocument16 pagesJanFeb 08 WebbernardhhiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Forest Beach Condos Market OverviewDocument111 pagesForest Beach Condos Market Overviewbernardhhi100% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Spring 2008 Continuing-Registration-FormDocument1 pageSpring 2008 Continuing-Registration-FormbernardhhiNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Heroes On Horseback Participant Registration and Photo Release FormDocument11 pagesHeroes On Horseback Participant Registration and Photo Release FormbernardhhiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ladybird Book - The PolicemanDocument15 pagesLadybird Book - The Policemanbernardhhi91% (11)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- HOH Volunteer FormsDocument4 pagesHOH Volunteer FormsbernardhhiNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Summer 2008 Continuing-Registration-FormDocument1 pageSummer 2008 Continuing-Registration-FormbernardhhiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Participant Registration FORMSDocument6 pagesParticipant Registration FORMSbernardhhi100% (1)
- The Magnesium MiracleDocument3 pagesThe Magnesium MiracleAuthentic English70% (10)
- NICE DRAFT - Drug Allergy Diagnosis and Management of Drug Allergy in Adults, Children and Young PeopleDocument29 pagesNICE DRAFT - Drug Allergy Diagnosis and Management of Drug Allergy in Adults, Children and Young Peopletian download doangNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Case ReportDocument19 pagesCase ReportvivitaslimNo ratings yet
- Growth - Development of Fetus - NeonateDocument40 pagesGrowth - Development of Fetus - NeonatesujidahNo ratings yet
- Unstable Angina: CausesDocument5 pagesUnstable Angina: CausesMahnoorNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Neurodevelopmental AssessmentDocument11 pagesNeurodevelopmental AssessmentReem SaNo ratings yet
- An Urgent Letter To Albertans From ICU PhysiciansDocument4 pagesAn Urgent Letter To Albertans From ICU PhysiciansCalgary Herald NewsroomNo ratings yet
- Buccal Midazolam CEWT Pi MidazDocument2 pagesBuccal Midazolam CEWT Pi MidazAgnieszka WaligóraNo ratings yet
- Mechanism of HyperventilationDocument1 pageMechanism of HyperventilationEdio PathicNo ratings yet
- Biology C - Lesson 1 - Circulatory SystemDocument46 pagesBiology C - Lesson 1 - Circulatory SystemMuhammad Azrie0% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- An Essay On "Covid-19 Pandemic" by Prof. Dr. Mustafa Asim SafakDocument9 pagesAn Essay On "Covid-19 Pandemic" by Prof. Dr. Mustafa Asim Safakkasmakiprawi72No ratings yet
- The Developmental Epidemiology of Anxiety Disorders Phenomenology, Prevalence, and ComorbityDocument18 pagesThe Developmental Epidemiology of Anxiety Disorders Phenomenology, Prevalence, and ComorbityShirleuy GonçalvesNo ratings yet
- OET Speaking Criteria ChecklistDocument4 pagesOET Speaking Criteria ChecklistNobomita GhoshNo ratings yet
- Short Case Hydrocephalus: by Febrianto Haba Bunga, S.Ked Consultant DR .Donny Argie, SP - BSDocument29 pagesShort Case Hydrocephalus: by Febrianto Haba Bunga, S.Ked Consultant DR .Donny Argie, SP - BSErkoNo ratings yet
- Famotidine (Pepcid)Document1 pageFamotidine (Pepcid)Cassie100% (1)
- Skripsi Jonathan Darell Widjaja 1206230025Document41 pagesSkripsi Jonathan Darell Widjaja 1206230025Jonathan Darell WijayaNo ratings yet
- Ankylosing SpondylitisDocument5 pagesAnkylosing SpondylitisHarry IsraNo ratings yet
- S17820en PDFDocument433 pagesS17820en PDFsafasayedNo ratings yet
- Massive Transfusion ProtocolDocument5 pagesMassive Transfusion ProtocolArlette Araceli Barbosa IbarraNo ratings yet
- Patient Report BALRAM SINGHDocument2 pagesPatient Report BALRAM SINGHNeeraj KumarNo ratings yet
- Cefaleia - ContinuumDocument195 pagesCefaleia - ContinuumRafaelNo ratings yet
- The Health Belief ModelDocument5 pagesThe Health Belief ModelYerichu JNo ratings yet
- MNDDocument28 pagesMNDGayle VillarizaNo ratings yet
- Novo Nordisk Strategy Global Access Diabetes CareDocument12 pagesNovo Nordisk Strategy Global Access Diabetes CareAmir IntizarNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Choanal Atresia PDFDocument8 pagesChoanal Atresia PDFMonna Medani LysabellaNo ratings yet
- Allison H. Feibus, MD, MS: Summa Cum LaudeDocument9 pagesAllison H. Feibus, MD, MS: Summa Cum Laudemmmmder7No ratings yet
- Lesson Exemplar in Mapeh Grade Level Learning Area QuarterDocument8 pagesLesson Exemplar in Mapeh Grade Level Learning Area QuarterErwin Balid GasconNo ratings yet
- HirsutismDocument19 pagesHirsutismCita KresnandaNo ratings yet
- The Sight Vol. 5Document60 pagesThe Sight Vol. 5optometrynepalNo ratings yet
- FORMAT OF A TEACHING PLAN NewDocument6 pagesFORMAT OF A TEACHING PLAN NewJahay NielNo ratings yet