You might also like
- Sik Weny LoboDocument15 pagesSik Weny LobonoviNo ratings yet
- Presentation On Health Care System ModelsDocument37 pagesPresentation On Health Care System ModelsTashi Makpen100% (1)
- Comparative Study of UK, USA and Indian Health Care SystemDocument12 pagesComparative Study of UK, USA and Indian Health Care SystemArnab Chatterjee67% (3)
- Health System Model of VietnamDocument20 pagesHealth System Model of Vietnamsneha khuranaNo ratings yet
- Health Insurance: Passed By: Rhea May PoriloDocument12 pagesHealth Insurance: Passed By: Rhea May PoriloRhea May PoriloNo ratings yet
- European Health Care Systems ComparisonDocument15 pagesEuropean Health Care Systems ComparisonNofalyaKamalinNo ratings yet
- Report On Health Insurance 2Document23 pagesReport On Health Insurance 2DrJaideep KumarNo ratings yet
- Health Care Schemes Project at KamineniDocument78 pagesHealth Care Schemes Project at KamineniVenugopal VutukuruNo ratings yet
- Health Financing MethodsDocument3 pagesHealth Financing MethodsMuna Hassan MustafaNo ratings yet
- Healthcare Reform ChecklistDocument60 pagesHealthcare Reform ChecklistSam Vaknin100% (18)
- Herbert - Nyirenda 1590992698 ADocument39 pagesHerbert - Nyirenda 1590992698 ADavid LyeluNo ratings yet
- The Singaporean Health Care SystemDocument16 pagesThe Singaporean Health Care SystemKholishotun NufusNo ratings yet
- Healthcare SystemsDocument2 pagesHealthcare SystemsFlor IgartuaNo ratings yet
- Comparative Healthcare SystemsDocument95 pagesComparative Healthcare SystemsLuiggi GordilloNo ratings yet
- 2023 MBCHB Health Financing and Provider Payment MechanismsDocument59 pages2023 MBCHB Health Financing and Provider Payment MechanismsKELLY KIPKOECHNo ratings yet
- BSC II Health Financing in UgandaDocument25 pagesBSC II Health Financing in UgandaYusto FoshizoNo ratings yet
- Health Care System of The Philippines and Switzerland PhilippinesDocument2 pagesHealth Care System of The Philippines and Switzerland PhilippinesJohn Adrian MaulionNo ratings yet
- Averting The Medicare Crisis: Health IRAs, Cato Policy AnalysisDocument8 pagesAverting The Medicare Crisis: Health IRAs, Cato Policy AnalysisCato InstituteNo ratings yet
- Philippine Health Insurance CorporationDocument7 pagesPhilippine Health Insurance CorporationEllen Glae DaquipilNo ratings yet
- Ealth Nsurance IN Ndia: R M - 05PH2010Document6 pagesEalth Nsurance IN Ndia: R M - 05PH2010api-26832469No ratings yet
- Medical Health Insurance Systems in Europe, USA, Canada, and AustraliaDocument13 pagesMedical Health Insurance Systems in Europe, USA, Canada, and Australiaeko abiNo ratings yet
- Healthcare FinancingDocument4 pagesHealthcare Financingabas ibrahimNo ratings yet
- Health SystemsDocument8 pagesHealth SystemsLloyd SalesNo ratings yet
- Canada: Robert G. Evans University of British ColumbiaDocument10 pagesCanada: Robert G. Evans University of British ColumbiaDylan MartinezNo ratings yet
- Health Care in Canada Has Long Been A Source of National PrideDocument24 pagesHealth Care in Canada Has Long Been A Source of National PridecadecortxNo ratings yet
- Healthcare Reform: Enhancing Services On A Sustainable BasisDocument18 pagesHealthcare Reform: Enhancing Services On A Sustainable BasisextravaganzarNo ratings yet
- International Social Welfare ProgramsDocument10 pagesInternational Social Welfare ProgramsZaira Edna JoseNo ratings yet
- UK Country Profile 2008Document3 pagesUK Country Profile 2008albajcNo ratings yet
- Health Financing FunctionsDocument4 pagesHealth Financing FunctionsFredy GunawanNo ratings yet
- Model of Healthcare FinancingDocument2 pagesModel of Healthcare FinancingdebestieNo ratings yet
- Dr. Padma Bhatia: Assistant Professor Department of Community Medicine G.M.C., Bhopal. M.P. IndiaDocument30 pagesDr. Padma Bhatia: Assistant Professor Department of Community Medicine G.M.C., Bhopal. M.P. IndiaSakshi SuriNo ratings yet
- Chapter 5 Health EconDocument7 pagesChapter 5 Health EconDoffCruzNo ratings yet
- Health Insurance1Document3 pagesHealth Insurance1jincygeevarghese7132No ratings yet
- Philippine Health CareDocument8 pagesPhilippine Health CareCarl Mark Vincent BabasoroNo ratings yet
- Sistem ImunDocument16 pagesSistem ImunDwii N AriiyantooNo ratings yet
- Nu710 w5 - Paper International Healthcare SystemsDocument11 pagesNu710 w5 - Paper International Healthcare Systemsapi-577441503No ratings yet
- Healthcare System in JapanDocument4 pagesHealthcare System in JapanBayuAkbarSyarifNo ratings yet
- Who 1Document23 pagesWho 1DBXGAMINGNo ratings yet
- France Healthcare SystemsDocument20 pagesFrance Healthcare SystemsRutvik GandhiNo ratings yet
- Health Care USA Chapter 8Document76 pagesHealth Care USA Chapter 8David TurnerNo ratings yet
- Privatisation of Healthcare in IndiaDocument2 pagesPrivatisation of Healthcare in IndiaParminder SinghNo ratings yet
- Health Care SystemDocument5 pagesHealth Care SystemadelekeyusufNo ratings yet
- Health InsurancesDocument7 pagesHealth InsurancesGlorina KumarNo ratings yet
- 9.4 Ethical Issues in The Provision of Health CareDocument7 pages9.4 Ethical Issues in The Provision of Health CareAngelica NatanNo ratings yet
- KFF Primer On MedicareDocument45 pagesKFF Primer On Medicarethanks maNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Health Insurance in Low Income Countries: Where Is The Evidence That It Works?Document29 pagesHealth Insurance in Low Income Countries: Where Is The Evidence That It Works?OxfamNo ratings yet
- Effective Discipline To Raise Healthy Children: Policy StatementDocument12 pagesEffective Discipline To Raise Healthy Children: Policy StatementJesse M. MassieNo ratings yet
- Identifying Child Abuse Fatalities During Infancy: Clinical ReportDocument11 pagesIdentifying Child Abuse Fatalities During Infancy: Clinical ReportJesse M. MassieNo ratings yet
- Difficult Patient Encounters: Assessing Pediatric Residents' Communication Skills Training NeedsDocument19 pagesDifficult Patient Encounters: Assessing Pediatric Residents' Communication Skills Training NeedsJesse M. MassieNo ratings yet
- Clinical Considerations Related To The Behavioral Manifestations of Child MaltreatmentDocument15 pagesClinical Considerations Related To The Behavioral Manifestations of Child MaltreatmentJesse M. MassieNo ratings yet
- Oral and Dental Aspects of Child Abuse and Neglect: Clinical ReportDocument10 pagesOral and Dental Aspects of Child Abuse and Neglect: Clinical ReportJesse M. MassieNo ratings yet
- Ongoing Pediatric Health Care For The Child Who Has Been MaltreatedDocument18 pagesOngoing Pediatric Health Care For The Child Who Has Been MaltreatedJesse M. MassieNo ratings yet
- Placement Changes and Emergency Department Visits in The First Year of Foster CareDocument9 pagesPlacement Changes and Emergency Department Visits in The First Year of Foster CareJesse M. MassieNo ratings yet
- IJMEDocument7 pagesIJMEJesse M. MassieNo ratings yet
- Making The Most of Mentors: A Guide For MenteesDocument5 pagesMaking The Most of Mentors: A Guide For MenteesJesse M. MassieNo ratings yet
- Jpeds Aom 208Document3 pagesJpeds Aom 208Jesse M. MassieNo ratings yet
- Emergency Severity IndexDocument114 pagesEmergency Severity Indexpafin100% (3)
- i-PASS OBSERVATION TOOLDocument1 pagei-PASS OBSERVATION TOOLJesse M. MassieNo ratings yet
- Persistent Fear and Anxiety Can Affect Young Childrens Learning and Development PDFDocument16 pagesPersistent Fear and Anxiety Can Affect Young Childrens Learning and Development PDFCristina AlexeevNo ratings yet
- Growth Chart IDocument1 pageGrowth Chart IJesse M. MassieNo ratings yet
- Cbig Cross-ReportingDocument25 pagesCbig Cross-ReportingJesse M. MassieNo ratings yet
- Suidi Oklahoma ProviderDocument28 pagesSuidi Oklahoma ProviderJesse M. MassieNo ratings yet
- Ckeck List Operacional - Usda Inst Saude e SegDocument3 pagesCkeck List Operacional - Usda Inst Saude e SegQualidade CooperalfaNo ratings yet
- dBA PROTECT YOUR HEARINGDocument4 pagesdBA PROTECT YOUR HEARINGJesse M. MassieNo ratings yet
- 2018 OdhhsDocument124 pages2018 OdhhsJesse M. MassieNo ratings yet
- Status EpileticusDocument2 pagesStatus EpileticusJesse M. MassieNo ratings yet
- Vroom Tips: Brain Building BasicsDocument16 pagesVroom Tips: Brain Building BasicsJesse M. MassieNo ratings yet
- What Is Child Abuse and Neglect? Recognizing The Signs and SymptomsDocument8 pagesWhat Is Child Abuse and Neglect? Recognizing The Signs and SymptomsJesse M. MassieNo ratings yet
- Vroom Tips: Brain Building BasicsDocument7 pagesVroom Tips: Brain Building BasicsJesse M. MassieNo ratings yet
- SB773Document257 pagesSB773Jesse M. MassieNo ratings yet
- Recommendations For Preventive Pediatric Health Care: Bright Futures/American Academy of PediatricsDocument2 pagesRecommendations For Preventive Pediatric Health Care: Bright Futures/American Academy of PediatricsJesse M. MassieNo ratings yet
- Domestic Violence Oklahoma 2017Document44 pagesDomestic Violence Oklahoma 2017Jesse M. MassieNo ratings yet
- Child Abuse Neglect Prevention OklahomaDocument44 pagesChild Abuse Neglect Prevention OklahomaJesse M. MassieNo ratings yet
- Preventing Adverse Childhood Experiences (Aces) :: Leveraging The Best Available EvidenceDocument40 pagesPreventing Adverse Childhood Experiences (Aces) :: Leveraging The Best Available EvidenceJesse M. MassieNo ratings yet
- COVID Positive/PUI: PAPR Prioritization MatrixDocument1 pageCOVID Positive/PUI: PAPR Prioritization MatrixJesse M. MassieNo ratings yet
- Intimate Partner Violence, Sexual Violence, Stalking: Before The Age of 18Document1 pageIntimate Partner Violence, Sexual Violence, Stalking: Before The Age of 18Jesse M. MassieNo ratings yet
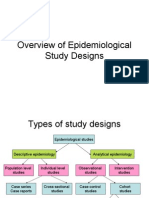
- Overview of Epidemiological Study DesignsDocument16 pagesOverview of Epidemiological Study DesignsLakshmi Seth100% (2)
- AQUALIPODocument16 pagesAQUALIPOAvalavenia Molina AbadNo ratings yet
- TB PDFDocument66 pagesTB PDFKyaw Zin HtetNo ratings yet
- Care Study OsteomyelitisDocument23 pagesCare Study OsteomyelitisJake Pitos100% (1)
- Assessment of Knowledge Attitude and Practice On Emergency Contraceptive Among Goba Female High School and Preparatory StudentsDocument9 pagesAssessment of Knowledge Attitude and Practice On Emergency Contraceptive Among Goba Female High School and Preparatory StudentsLawrence MungaNo ratings yet
- Curriculum Vitae Dr. Ari AstramDocument4 pagesCurriculum Vitae Dr. Ari AstramBedah ManadoNo ratings yet
- Equipoise HajjajDocument4 pagesEquipoise HajjajerrelyoNo ratings yet
- Prevalence and Recurrence Rate of Perianal Abscess - A Population-Based Study, Sweden 1997 - 2009Document5 pagesPrevalence and Recurrence Rate of Perianal Abscess - A Population-Based Study, Sweden 1997 - 2009Ridha Aswina DalimuntheNo ratings yet
- Assisting in Patients Undergoing A ThoracentesisDocument7 pagesAssisting in Patients Undergoing A Thoracentesiscoosa liquorsNo ratings yet
- Contraindications To Implant Treatment 1Document1 pageContraindications To Implant Treatment 1Hussien A. Abu OlbaNo ratings yet
- 02-09 2022 Pharm Pediatrics 2022 R4Document44 pages02-09 2022 Pharm Pediatrics 2022 R4Amira HelayelNo ratings yet
- The Carcinosin Drug Picture - Dr. FoubisterDocument34 pagesThe Carcinosin Drug Picture - Dr. FoubisterRogelio VillegasNo ratings yet
- Generic Name: Quinupristin/Dalfopristin - Injection (Kwin-ue-PRIS-tin/DAL-foe-PRIS-tin)Document4 pagesGeneric Name: Quinupristin/Dalfopristin - Injection (Kwin-ue-PRIS-tin/DAL-foe-PRIS-tin)Jrose CuerpoNo ratings yet
- Mrcpsych TipsDocument7 pagesMrcpsych Tipsmahadev470% (1)
- Wellness Massage AssessmentDocument3 pagesWellness Massage AssessmentElizabeth QuiderNo ratings yet
- Florence NightingaleDocument30 pagesFlorence Nightingalezeeky35No ratings yet
- Adolescent Substance AbuseDocument47 pagesAdolescent Substance AbuseIssa Thea BolanteNo ratings yet
- A Clinical Report On Partial Pulpotomy and Capping With Calcium Hydroxide in Permanent Incisors With Complicated Crown FractureDocument6 pagesA Clinical Report On Partial Pulpotomy and Capping With Calcium Hydroxide in Permanent Incisors With Complicated Crown Fractureroy sepNo ratings yet
- Inventory List at in Emergei (Cy: PrsentDocument1 pageInventory List at in Emergei (Cy: PrsentVirginia BennettNo ratings yet
- Problem PrioritizationDocument2 pagesProblem PrioritizationRegie GonzagaNo ratings yet
- Introduction To Medical MicrobiologyDocument60 pagesIntroduction To Medical Microbiologytummalapalli venkateswara rao100% (1)
- Uro-Gynaecology From Cambridge To UAE?Document28 pagesUro-Gynaecology From Cambridge To UAE?Michelle FynesNo ratings yet
- 2012 SLICC Criteria Systemic Lupus ErythematosusDocument10 pages2012 SLICC Criteria Systemic Lupus ErythematosusNaufal AndaluNo ratings yet
- Application of Functional Orthodontic Appliances To Treatment of Mandibular Retrusion Syndrome PDFDocument18 pagesApplication of Functional Orthodontic Appliances To Treatment of Mandibular Retrusion Syndrome PDFThu Trang Pham100% (1)
- DEMENTIADocument42 pagesDEMENTIAputri maharaniNo ratings yet
- Fdar Charting: Date, Time, and Shift Focus Progress NotesDocument1 pageFdar Charting: Date, Time, and Shift Focus Progress NotesYuvi Luardo100% (1)
- Nhs Bronchiolitis Pathway Acute Setting South East Coast SCNDocument2 pagesNhs Bronchiolitis Pathway Acute Setting South East Coast SCNdrgrizahNo ratings yet
- Jurnal Bahasa InggrisDocument9 pagesJurnal Bahasa InggrisNur Riza Maulidina100% (1)
- Malaysia Cancer StatisticsDocument136 pagesMalaysia Cancer Statisticsdigital896100% (1)
- LEV Medicine - Rejuvenation Research Guest EditorialDocument2 pagesLEV Medicine - Rejuvenation Research Guest EditorialoliverNo ratings yet