IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 13, Issue 6 Ver. III (Jun. 2014), PP 05-08
www.iosrjournals.org
www.iosrjournals.org 5 | Page
An evaluation of association between pre-hospital care with
injury severity scores among survivors of road traffic accidents in
a north Indian setting
Dr.Ravi Kant Singh
1
, Prof. Ashish Kumar
2
, Prof. G.K.Singh
3
, Prof. Santosh
Kumar
4
, Dr.Nidhi Singh
5
1Deptt. of Orthopaedics, King Georges Medical University, Lucknow (Uttar Pradesh) India
2Deptt. of Orthopaedics, King Georges Medical University
3Founder Director, AIIMS, Patna, Bihar,
4Deptt. of Orthopaedics, King Georges Medical University,
5Research Scholar,
Abstract: Objective: To compare the AIS and ISS scores according to pre-hospital care received among the
subjects of trauma victims
Methods: This was a cross-sectional study conducted in a trauma centre of north Indian tertiary care hospital.
The detailed history of the subjects was taken and AIS and ISS scores were calculated for each subject. The
subjects who got accident with a vehicle and admitted in the centre were included in the study. The burned and
subjects <12 years were excluded from the study.
Results: A total of 869 subjects were included in the study and majority were males (81.5%). Most of the
subjects received pre-hospital care (76.1%). The AIS was significantly (p=0.02) higher who received pre-
hospital care (1.770.58) than those who did not know (1.501.00) among head & neck injured subjects.
Similar observation was found among the subjects of face and extremities injured. The ISS was lower among
those who did not receive pre-hospital care (5.712.64) compared with who received (6.182.61). The ISS was
significantly (p=0.0001) different among the subjects who received pre-hospital care, did not received and
unknown injuries.
Conclusion: The pre-hospital care is an important factor for the survival of injured subjects. Specific strategy
should be made to provide the pre-hospital care at the site of victims.
Key words: Pre-hospital care, trauma, strategy
I. Introduction
Injury scoring systems are designed to accurately assess injury severity, appropriately triage the
injured, and develop and refine trauma patient care (Furnival, 1999). Trauma scores quantify the severity and
extent of injury, aid with the prediction of survival and subsequent morbidity, (Fani-Salek, 1999) and allow
health care providers to communicate in common terms. One disadvantage of injury scoring systems is that
patient information is reduced to a simple score, and important details may be lost. To accurately estimate
patient outcome, it is necessary to precisely assess the patients anatomic and physiologic injury, as well as any
preexisting medical conditions that can impair the patients ability to respond to the stress of the injuries
sustained.
Characterization and documentation of injury severity are requirements for the evaluation of trauma
systems and development of initiative in injury control. The development of valid and useful quality
improvement methods, comparisons of therapeutic modalities with the outcomes of trauma patients, collection
of basic epidemiologic trauma data and effective use of pre-hospital and inter-hospital triage are major needs in
the trauma care system (Brenneman et al, 1998). A prerequisite to meet these needs is the uniform application of
severity scales to the trauma patients (Sharma et al, 2003). Current commonly used scales can be grouped
according to the type of patient information on which they are based, such as: Physiologic Scores that include
vital signs such as pulse, blood pressure, respiratory rate and level of consciousness. Glasgow Coma Scale
(GCS), Revised Trauma Scale (RTS), for patients with serious head injuries, Circulation, Respiration,
Abdominal/Thoracic, Motor, Speech Scale (CRAMS), Acute Physiology and Chronic Health Evaluation
(APACHE), etc. The Injury Severity Score (ISS) is virtually the only anatomical scoring system in use and
correlates linearly with mortality, morbidity, hospital stay and other measures of severity.
The present study was designed to compare the AIS and ISS scores according to pre-hospital care
received among the subjects of trauma victims in a tertiary care hospital of north India.
An evaluation of association between pre-hospital care with injury severity scores among survivors ...
www.iosrjournals.org 6 | Page
II. Material And Methods
This was a cross-sectional study conducted among the subjects admitted in the Trauma centre of KG
Medical University, Lucknow. The study was approved by the institutional ethical committee. The informed
consent was taken from each subjects/attendant before including in the study. The inclusion criteria was
subjects admitted in Trauma Centre suffered injuries due to road traffic accidents. The exclusion criteria were
an injury on road without involvement of vehicle (subjects slipping & falling on the road & sustaining injury),
injury involving a stationary vehicle (subjects getting injured while washing or loading a vehicle), brought dead
due to RTA, subjects not giving informed consent (in coma, unconscious, for more than 3 days post injury &
unable to understand or reply due to shock, subjects referred to trauma centre after being treated elsewhere for
more than 3 days, burn subjects and subjects under 12 years.
The Abbreviated Injury Scale (AIS) of each injury was determined using Association for Advancement
of Automobile Medicine 1990 protocol. Each case was examined in detail and ISS calculated based on the AIS.
Other relevant parameters like age, sex, survival status, date & time of injury and medical interventions done
were also recorded. Depending on the type of injury, Abbreviated injury score is calculated for each case.
Injuries are ranked on a scale of 1 to 6, with 1 being minor, 5 severe and 6 an unsurvivable injury. From
Abbreviated Injury Score (AIS), Injury severity score is calculated. The Injury Severity Score is an anatomical
scoring system that provides an overall score for patients with multiple injuries. Each injury is assigned an
Abbreviated Injury Scale score and is allocated to one of six body regions (Head, Face, Chest, Abdomen,
Extremities (including Pelvis), and external). Only the highest AIS score in each body region is used. The 3
most severely injured body regions have their score squared and added together to produce the ISS score.
The results are presented in percentages. The association of pre-hospital care with the outcome of
trauma was assessed by using Chi-square test. The p-value<0.05 was considered significant. All the analysis
was carried out by using SPSS 16.0 version (Chicago, Inc. USA).
III. Results
Table-1 presents the distribution of the injured subjects according to age and gender. Most of the
subjects were between 20-30 years (46.7) followed by 31-40 (21.4%) and majority were males (81.5%).
The majority (85.2%) of the subjects received first aid from nearby government hospital followed by
nearby private hospital/clinic and at accident place (Fig.1).
The AIS was significantly (p=0.02) higher who received pre-hospital care (1.770.58) than those who did not
know (1.501.00) among head & neck injured subjects. Similar observation was found among the subjects of
face and extremities injured. The ISS was lower among those who did not receive pre-hospital care (5.712.64)
compared with who received (6.182.61). The ISS was significantly (p=0.0001) different among the subjects
who received pre-hospital care, did not received and unknown injuries.
The AIS was significantly different with the different timing of the pre-hospital care in head & neck,
face, chest, abdominal & pelvic content, extremities and external. The ISS was significantly (p=0.002) higher
among those who received pre-hospital care after 60 minute (6.192.86) than within 30 minute and 30-60
minutes (6.182.52) (Table-3).
Table-1: Distribution of the injured subjects according to age and gender
Age in years No.
(n=869)
%
Age in years
<20 113 13.0
20-30 406 46.7
31-40 186 21.4
41-50 112 12.9
51-60 39 4.5
>60 13 1.5
Gender
Male 708 81.5
Female 161 18.5
An evaluation of association between pre-hospital care with injury severity scores among survivors ...
www.iosrjournals.org 7 | Page
Fig.1: Distribution of the subjects according to place of first AID received
Table-2: Comparison of AIS and ISS scores according to Pre hospital care
AIS scores ISS
Pre-
hospital
care
No.
(n=869)
% Head &
Neck
Face Chest Abdominal
& pelvic
content
Extremiti
es
External
Yes 661 76.1 1.770.58
2
1.450.49
2
1.590.70 1.080.93
2
1.760.52
2
1.010.07 6.182.61
No 179 20.6 1.580.61 1.520.50 1.500.53 1.920.76
3
1.650.54 1.010.10 5.712.64
2
Not
known
29 3.3
1.501.00
2
2.000.40
2
2.000.65 4.000.16
2,3
1.120.35
2
1.000.00 7.761.70
2
p-value
1
0.02* 0.04* 0.52 0.001* 0.001* 0.80 0.0001*
1
ANOVA, *Significant,
2
p<0.05,
3
p<0.01 (Post-hoc comparison test)
Table-3: Comparison of AIS and ISS scores according to time of Pre hospital care
Time of
Pre-
hospital
care
No.
(n=661)
% AIS scores ISS
Head &
Neck
Face Chest Abdominal &
pelvic content
Extremities External
Within
30
minutes
185 28.0
1.790.50 1.490.50 1.400.50 0.430.53 1.760.48 1.010.10 6.192.86
30-60
minutes
447 67.6
1.760.62 1.440.49 1.740.80 1.250.96 1.740.54 1.000.06 6.182.52
>60
minutes
29 4.4
1.920.60 1.970.51 1.920.89 1.940.11 1.990.49 1.290.03 6.992.35
p-value
1
0.02* 0.01* 0.02* 0.002* 0.003* 0.004* 0.002*
1
ANOVA, *Significant
IV. Discussion
The present study investigated the association between AIS and ISS with the pre-hospital care received.
In our best knowledge, none of the study had correlated these parameters. Common to all RTI studies males are
the commonly affected population in our study as males tend to travel more in comparison to females with age
group of 20-30 years (Sharma et al, 2002; Sharma et al, 2005). Baker et al introduced the ISS in 1974 as a
means of summarizing multiple injuries in a single patient. The ISS is defined as the sum of squares of the
highest AIS grade in the 3 most severely injured body regions and ranges from 1-75. An ISS of 75 is assigned to
anyone with AIS of 6, as all the AIS 6 injuries are inherently fatal (Sharma et al, 2005).
Every trauma service should review the process and outcome of patient care on monthly basis as
recommended by the Joint Commission on Accreditation of Healthcare Organization's (JCAHO) mandated
reviews of quality improvement and utilization. Indices of severity and audit criteria are of value in identifying
aberrant outcomes or potential problems in patient care, and in prompting remedial action. Strategies for quality
improvement in trauma care should involve the policy or process of managing the major trauma victim
(Rutledge et al, 1993).
The AP addresses some of the shortcomings of the ISS. It uses the AIS descriptors of anatomic injury,
but includes only four body regions: A =head/brain and spinal cord; B = thorax/neck; C = all other serious
injuriesother than in the areas of A and B; and D = all non-serious injuries (Furnival, 1999; Fani-Salek, 1999).
An evaluation of association between pre-hospital care with injury severity scores among survivors ...
www.iosrjournals.org 8 | Page
Injuries with an AIS value >2, which are defined as serious, are scored for the first three categories above
(Furnival, 1999). All minor injuries, defined as AIS scores of 2, are classified as non-serious, regardless of
their anatomic location (Fani-Salek, 1999). The total AP score is the sum of the square roots of the sum of the
squares of the AIS for all individual injuries within a region (Furnival, 1999; Fani-Salek, 1999). This allows the
second and third injuries occurring within a given region to be considered in the final AP score, preventing the
loss of information that occurs with the ISS (Furnival, 1999). AP is most useful in an inpatient setting and has
neither been widely used nor validated for paediatric trauma (Furnival, 1999; Fani-Salek, 1999).
Trauma registries must be founded on complete, accurate data that includes explicit and accurate
descriptions of physiologic derangement and injuries as well as accurate injury coding based on ICD-9-CM
codes, by the clinicians in medical record.
V. Conclusion
The pre-hospital care is an important factor for the survival of injured subjects. Specific strategy should
be made to provide the pre-hospital care at the site of victims.
Source of funding:
Conflict of interest:
References
[1]. Furnival RA, Schunk JE. ABCs of scoring systems for pediatric trauma. Pediatr Emerg Care 1999; 15:215223.
[2]. Fani-Salek MH, Totten VY, Terezakis SA. Trauma scoring systems explained. Emerg Med 1999; 11:155166.
[3]. Brenneman FD, Boulonger BR, McLellan BA, et al. Measuring injury severity: time for a change? J Trauma Injury, Infection and
Critical Care, 1998; 44 (4): 580-584.
[4]. Sharma BR, Harish D, Singh G et al. Pattern of Head Injuries in Fatal Road Traffic Accidents. Bahrain Med. Bulletin. 2003; 25 (1):
22 - 25.
[5]. Sharma BR, Gautam CS, Singh R. Road Traffic Accidents Vis--vis Problems Related to Ageing. Hospital Today 2002; VII (10):
523- 528.
[6]. Sharma BR. The Injury Scale - a valuable tool for forensic documentation of trauma. J Clinical Forensic Medicine. 2005; 12 (1): 21
-28.
[7]. Sharma BR, Gupta M, Bangar S. NISS a valuable tool for trauma scoring on autopsy. J Biological Sciences 2005; 8 (7): 995 - 1000.
[8]. Rutledge R, Fakhry S, Baker C, et al. Injury severity grading in trauma patients: a simplified technique based upon ICD 9 coding.
J Trauma 1993; 35: 497.
[9]. Furnival RA, Schunk JE. ABCs of scoring systems for pediatric trauma. Pediatr Emerg Care 1999; 15:215223.
You might also like
- Effects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaDocument10 pagesEffects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaInternational Organization of Scientific Research (IOSR)100% (1)
- Youth Entrepreneurship: Opportunities and Challenges in IndiaDocument5 pagesYouth Entrepreneurship: Opportunities and Challenges in IndiaInternational Organization of Scientific Research (IOSR)100% (1)
- Necessary Evils of Private Tuition: A Case StudyDocument6 pagesNecessary Evils of Private Tuition: A Case StudyInternational Organization of Scientific Research (IOSR)No ratings yet
- Comparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockDocument2 pagesComparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockInternational Organization of Scientific Research (IOSR)No ratings yet
- Factors Affecting Success of Construction ProjectDocument10 pagesFactors Affecting Success of Construction ProjectInternational Organization of Scientific Research (IOSR)No ratings yet
- Design and Analysis of Ladder Frame Chassis Considering Support at Contact Region of Leaf Spring and Chassis FrameDocument9 pagesDesign and Analysis of Ladder Frame Chassis Considering Support at Contact Region of Leaf Spring and Chassis FrameInternational Organization of Scientific Research (IOSR)No ratings yet
- Design and Analysis of An Automotive Front Bumper Beam For Low-Speed ImpactDocument11 pagesDesign and Analysis of An Automotive Front Bumper Beam For Low-Speed ImpactInternational Organization of Scientific Research (IOSR)No ratings yet
- Fatigue Analysis of A Piston Ring by Using Finite Element AnalysisDocument4 pagesFatigue Analysis of A Piston Ring by Using Finite Element AnalysisInternational Organization of Scientific Research (IOSR)No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Zamboanga Historical Dates-Islam 1400s To Death of Gen. Alvarez 1942Document22 pagesZamboanga Historical Dates-Islam 1400s To Death of Gen. Alvarez 1942arenriquezNo ratings yet
- Bus Ticket Confirmation PDFDocument2 pagesBus Ticket Confirmation PDFAnonymous g0akpV9loNo ratings yet
- The State V Oscar Leonard Carl PistoriusDocument73 pagesThe State V Oscar Leonard Carl Pistoriusvuv2bav6No ratings yet
- Rifts - Character Sheet Version 2 PDFDocument2 pagesRifts - Character Sheet Version 2 PDFMilander42No ratings yet
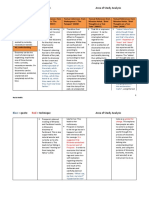
- Quote Technique Area of Study Analysis: Repetition of "Leave" and "Alone"Document19 pagesQuote Technique Area of Study Analysis: Repetition of "Leave" and "Alone"Krishna KannanNo ratings yet
- Warcraft Rules ConversionDocument182 pagesWarcraft Rules ConversionsaxonD777100% (3)
- Lich ArtificerDocument4 pagesLich ArtificerrzielaznickiNo ratings yet
- Frankenstein, or The 8 Bit Prometheus by Riccardo Balli (Chili Com Carne, 2018)Document140 pagesFrankenstein, or The 8 Bit Prometheus by Riccardo Balli (Chili Com Carne, 2018)Riccardo100% (1)
- Death Note "The Last Name"Document4 pagesDeath Note "The Last Name"Mikaela Siriban VillamoraNo ratings yet
- HellDocument2 pagesHellArghya ChakrabortyNo ratings yet
- The Barrow of The Moon DruidDocument29 pagesThe Barrow of The Moon DruidArmando Signore100% (1)
- Book ReviewDocument4 pagesBook Reviewapi-255518614No ratings yet
- 1932 White Zombie ScriptDocument26 pages1932 White Zombie ScriptJames D. SassNo ratings yet
- This Is A Book For Survivors of Unspeakable Loss - The Suicide of A Loved OneDocument13 pagesThis Is A Book For Survivors of Unspeakable Loss - The Suicide of A Loved OnenatasaknezNo ratings yet
- Themes in HamletDocument5 pagesThemes in HamletChiosa AdinaNo ratings yet
- John Sparrow Thompson Grave Site Monitoring Report 2011Document20 pagesJohn Sparrow Thompson Grave Site Monitoring Report 2011Jordan PressNo ratings yet
- Inheritance LawDocument13 pagesInheritance LaweisworoNo ratings yet
- Why Do We Kill? Kelvin Sewell and Stephen JanisDocument4 pagesWhy Do We Kill? Kelvin Sewell and Stephen JanisApple SpotcrimeNo ratings yet
- A Systematic Review of The Mortality of DepressionDocument12 pagesA Systematic Review of The Mortality of Depressionadri90No ratings yet
- Heirs of Maximo Regoso Vs Court of AppealsDocument1 pageHeirs of Maximo Regoso Vs Court of AppealsPiaNo ratings yet
- Beowulf - An Anglo-Saxon Epic Poem PDFDocument117 pagesBeowulf - An Anglo-Saxon Epic Poem PDFNaejla M. SajirdesNo ratings yet
- Chapter 3: Death Legal Presumption of Death: A Person Is Deemed To Have Died, If Absent Without Explanation From His orDocument6 pagesChapter 3: Death Legal Presumption of Death: A Person Is Deemed To Have Died, If Absent Without Explanation From His orHomer SimpsonNo ratings yet
- 72 Shohda-e-KarbalaDocument2 pages72 Shohda-e-KarbalaZain HemaniNo ratings yet
- Lesson of The KaibabDocument2 pagesLesson of The Kaibabapi-294565326No ratings yet
- Mithridates of PontusDocument9 pagesMithridates of PontusMihaela Botnari-GuţuNo ratings yet
- Film Mirip Crows ZeroDocument1 pageFilm Mirip Crows ZeroAjie Bagus RamadiantoNo ratings yet
- The Akathist of Thanksgiving by Hieromartyr Grigori Petroff Kontakion 1Document14 pagesThe Akathist of Thanksgiving by Hieromartyr Grigori Petroff Kontakion 1Marco AntonioNo ratings yet
- Lesson 4: The Cadaver: Group 2Document19 pagesLesson 4: The Cadaver: Group 2Ashly Nicole MontajesNo ratings yet
- Police BlotterDocument2 pagesPolice BlotterFreeza Masculino Fabrigas100% (1)
- Aranas V.mercadoDocument2 pagesAranas V.mercadopaulus johnes PavericioNo ratings yet