You might also like
- OB/GynDocument11 pagesOB/GynAnonymous TYyF7Ul9o100% (2)
- Ob-Gyn OsceDocument2 pagesOb-Gyn Oscechristietwong100% (1)
- TRP OB-GYN Study GuideDocument28 pagesTRP OB-GYN Study Guideemmaaziz100% (9)
- ObyGyn - OSCE (FG2)Document23 pagesObyGyn - OSCE (FG2)roorian100% (1)
- Obgyn UWISE Notes (And Master The Boards)Document8 pagesObgyn UWISE Notes (And Master The Boards)Laura Lopez Roca100% (5)
- Gynecology and Contraception TopicsDocument24 pagesGynecology and Contraception Topicslizzy596No ratings yet
- Endometrial CA and Pregnancy Risk FactorsDocument11 pagesEndometrial CA and Pregnancy Risk FactorsLaura Lopez Roca0% (1)
- Obstetrics and Gyn Outline - NBMEDocument6 pagesObstetrics and Gyn Outline - NBMEGameron777No ratings yet
- OB-GYN - Shelf Review NotesDocument47 pagesOB-GYN - Shelf Review NotesJackJoseph95% (19)
- Clinical Pearls for Reproductive HealthDocument4 pagesClinical Pearls for Reproductive HealthD50% (4)
- Obgyn Clerkship Guide To SuccessDocument6 pagesObgyn Clerkship Guide To SuccessprabhatNo ratings yet
- OBG-GYN Practice QuestionsDocument222 pagesOBG-GYN Practice QuestionsRizwanNo ratings yet
- Divine Intervention Episode 22 Obgyn Shelf Review PDFDocument167 pagesDivine Intervention Episode 22 Obgyn Shelf Review PDFSwisskelly1100% (1)
- ObGyn Outline BeckmannDocument85 pagesObGyn Outline Beckmannp4sierra50% (2)
- Doctor High Yield Obgyn - Not AnnotatedDocument34 pagesDoctor High Yield Obgyn - Not AnnotatedEmanuella Gomez100% (2)
- APGODocument49 pagesAPGOiamdonutNo ratings yet
- Uwise ReviewDocument14 pagesUwise ReviewAnonymous T1G9BQQNo ratings yet
- Obgyn NotesDocument2 pagesObgyn NotesBillie AllenNo ratings yet
- NBME OBGYN2 6 Wrong With Answers Searchable 2 PDFDocument50 pagesNBME OBGYN2 6 Wrong With Answers Searchable 2 PDFSheema ShNo ratings yet
- LSU Peds ReviewDocument27 pagesLSU Peds Reviewnicdeep100% (2)
- OBGYN Shelf NotesDocument7 pagesOBGYN Shelf NotesaelteeNo ratings yet
- STIs, herpes screening, HPV vaccination, and prenatal careDocument26 pagesSTIs, herpes screening, HPV vaccination, and prenatal careAyodeji SotimehinNo ratings yet
- CMS - Ob - Gyn 1-Answers PDFDocument13 pagesCMS - Ob - Gyn 1-Answers PDFSelena GajićNo ratings yet
- Ob Gyn Notes - UWorld 2018Document17 pagesOb Gyn Notes - UWorld 2018Fake person0% (1)
- OB-GYN Oral Exam Study GuideDocument34 pagesOB-GYN Oral Exam Study GuidePatrick Sylvester100% (1)
- ObGyn - OutlineDocument85 pagesObGyn - OutlineMatt McGlothlin100% (2)
- OBGYN Shelf SR: Top 40 OBGYN Questions & AnswersDocument13 pagesOBGYN Shelf SR: Top 40 OBGYN Questions & AnswerslindaNo ratings yet
- CMS Ob&Gyn 4 AnswersDocument21 pagesCMS Ob&Gyn 4 AnswersVictor Conan100% (2)
- High-Yield Shelf NotesDocument170 pagesHigh-Yield Shelf Notes1nertia100% (10)
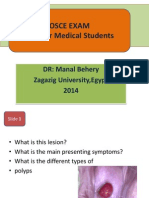
- OSCE in Obstetrics&Gynecology For UndergraduateDocument66 pagesOSCE in Obstetrics&Gynecology For UndergraduateManal Behery80% (5)
- OBGYN NotesDocument29 pagesOBGYN NotesavavNo ratings yet
- USMLE Step 2 CK Bible 2nd EdDocument435 pagesUSMLE Step 2 CK Bible 2nd EdShyama SharmaNo ratings yet
- CMS 3 AnswersDocument10 pagesCMS 3 AnswersVictor ConanNo ratings yet
- Divine Intervention Episode 21 Peds Shelf Review PDFDocument139 pagesDivine Intervention Episode 21 Peds Shelf Review PDFSwisskelly1No ratings yet
- Pediatrics SHELFDocument31 pagesPediatrics SHELFAztec100% (5)
- NBME Medicine Shelf Review Session 1 High-Yield TopicsDocument54 pagesNBME Medicine Shelf Review Session 1 High-Yield TopicsHersheyth AggarwalNo ratings yet
- The ShelfDocument18 pagesThe Shelfsowcowdd100% (5)
- Online Med Ed NotesDocument12 pagesOnline Med Ed NotessonNo ratings yet
- Ob & Gyn Form 1 ReviewDocument13 pagesOb & Gyn Form 1 ReviewMohamed Abib100% (6)
- Emma Holliday Surgery Notes - Cornell StyleDocument299 pagesEmma Holliday Surgery Notes - Cornell StyleBanana MuffinNo ratings yet
- January 2020Document5 pagesJanuary 2020nreena aslamNo ratings yet
- B) Reassurance That This Is Normal InitiallyDocument51 pagesB) Reassurance That This Is Normal InitiallygofisheeNo ratings yet
- Obgyn MnemonicsDocument4 pagesObgyn Mnemonicsapi-3700579100% (17)
- OBGYN Student Study GuideDocument39 pagesOBGYN Student Study GuideGoffo13100% (4)
- NBME Pediatrics Exam 2011Document8 pagesNBME Pediatrics Exam 2011lcaskidsn12s60% (5)
- EMMaA - IMDocument100 pagesEMMaA - IMR IghtzedNo ratings yet
- Study Guide For OBGYNDocument34 pagesStudy Guide For OBGYNFiorellaBeatriz100% (1)
- Step 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- Comprehensive Handbook Obstetrics & Gynecology 3rd EdFrom EverandComprehensive Handbook Obstetrics & Gynecology 3rd EdRating: 5 out of 5 stars5/5 (1)
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3From EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3Rating: 5 out of 5 stars5/5 (1)
- The Unofficial Guide to Obstetrics and Gynaecology: Core O&G Curriculum Covered: 300 Multiple Choice Questions with Detailed Explanations and Key Subject SummariesFrom EverandThe Unofficial Guide to Obstetrics and Gynaecology: Core O&G Curriculum Covered: 300 Multiple Choice Questions with Detailed Explanations and Key Subject SummariesRating: 1.5 out of 5 stars1.5/5 (3)
- Medical School Companion Obstetrics and Gynecology Practice Question BookFrom EverandMedical School Companion Obstetrics and Gynecology Practice Question BookNo ratings yet
- U.S. MEDICAL LICENSING EXAM (USMLE) STEP III – Patient Management: Passbooks Study GuideFrom EverandU.S. MEDICAL LICENSING EXAM (USMLE) STEP III – Patient Management: Passbooks Study GuideNo ratings yet
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1From EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1Rating: 5 out of 5 stars5/5 (2)
- Radiology Fundamentals: Introduction to Imaging & TechnologyFrom EverandRadiology Fundamentals: Introduction to Imaging & TechnologyJennifer KissaneNo ratings yet
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessFrom EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanNo ratings yet
- Step Up To Medicine Chapter 03Document868 pagesStep Up To Medicine Chapter 03yanks1120No ratings yet
- Cell Wall Inhibitors and Protein Synthesis Inhibitors Antibiotics Mechanisms of ActionDocument3 pagesCell Wall Inhibitors and Protein Synthesis Inhibitors Antibiotics Mechanisms of Actionyanks1120No ratings yet
- Copd and SCDDocument10 pagesCopd and SCDyanks1120No ratings yet
- Uworld NotesDocument10 pagesUworld Notesyanks1120No ratings yet
- IM STEP 2 NotesDocument74 pagesIM STEP 2 Notesyanks1120100% (3)
- PrologueDocument3 pagesPrologueyanks1120No ratings yet
- Post-void residual volume and bladder scan interpretationDocument7 pagesPost-void residual volume and bladder scan interpretationyanks1120No ratings yet
- Kaplan Gen Surg Upper GIDocument1 pageKaplan Gen Surg Upper GIyanks1120No ratings yet
- Normal Breath SoundsDocument1 pageNormal Breath Soundsyanks1120No ratings yet
- AnemiaDocument4 pagesAnemiayanks1120No ratings yet
- ID Fungal InfectionsDocument2 pagesID Fungal Infectionsyanks1120No ratings yet
- Cell Wall Inhibitors and Protein Synthesis Inhibitors Antibiotics Mechanisms of ActionDocument3 pagesCell Wall Inhibitors and Protein Synthesis Inhibitors Antibiotics Mechanisms of Actionyanks1120No ratings yet
- Dermatomyositis ParagraphsDocument1 pageDermatomyositis Paragraphsyanks1120No ratings yet
- Breast CancerDocument2 pagesBreast Canceryanks1120No ratings yet
- I. Definition/General Consideration: AnaphylaxisDocument1 pageI. Definition/General Consideration: Anaphylaxisyanks1120No ratings yet
- Post-void residual volume and bladder scan interpretationDocument7 pagesPost-void residual volume and bladder scan interpretationyanks1120No ratings yet
- Normal Breath SoundsDocument1 pageNormal Breath Soundsyanks1120No ratings yet
- I. Definition/General Consideration: AnaphylaxisDocument1 pageI. Definition/General Consideration: Anaphylaxisyanks1120No ratings yet
- Acute PancreatitisDocument2 pagesAcute Pancreatitisyanks1120No ratings yet
- Acute Coronary SyndromeDocument3 pagesAcute Coronary Syndromeyanks1120No ratings yet
- ICM 5 ReviewDocument7 pagesICM 5 Reviewyanks1120No ratings yet
- Abdominal PainDocument2 pagesAbdominal Painyanks1120No ratings yet
- MeningitisDocument3 pagesMeningitisyanks1120No ratings yet
- Viral HepatitisDocument2 pagesViral Hepatitisyanks1120No ratings yet
- ImmunizationsDocument2 pagesImmunizationsyanks1120No ratings yet
- Hypo Thyroid Is MDocument2 pagesHypo Thyroid Is Myanks1120No ratings yet
- Anemia ChemistryDocument1 pageAnemia Chemistryyanks1120No ratings yet
- Lower Back PainDocument2 pagesLower Back Painyanks1120No ratings yet
- Pediatric Intracranial TumorsDocument1 pagePediatric Intracranial Tumorsyanks1120No ratings yet
- Ingham County Rescinds Two Emergency Orders Including Mask Requirement in Educational Institutions, Effective Feb. 19Document2 pagesIngham County Rescinds Two Emergency Orders Including Mask Requirement in Educational Institutions, Effective Feb. 19Jake DraugelisNo ratings yet
- 1996 AAZV ProceedingsDocument568 pages1996 AAZV Proceedingscristina_gomhNo ratings yet
- Official reprint from UpToDate® on gestational hypertensionDocument16 pagesOfficial reprint from UpToDate® on gestational hypertensionNestor FloresNo ratings yet
- CleeeeanDocument33 pagesCleeeeanJohn RockNo ratings yet
- Riggs, Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer, 2019Document14 pagesRiggs, Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer, 2019karla perezNo ratings yet
- Prednisone Drug StudyDocument4 pagesPrednisone Drug StudyTom CuencaNo ratings yet
- Clinical Presentation On AppendicectomyDocument30 pagesClinical Presentation On AppendicectomyValarmathiNo ratings yet
- American Survival Guide - June 2020 USA PDFDocument100 pagesAmerican Survival Guide - June 2020 USA PDFwilliam bayona100% (3)
- Chloromethyl Methyl Ether: Hazard SummaryDocument4 pagesChloromethyl Methyl Ether: Hazard SummaryJahajNo ratings yet
- NO-BS BODYBUILDING - The JDB Bible For Advanced Health & Fitness - Bold and Determined-1Document7 pagesNO-BS BODYBUILDING - The JDB Bible For Advanced Health & Fitness - Bold and Determined-1Salvador Braulio Rodriguez CarrilloNo ratings yet
- Wound Care ManagementDocument5 pagesWound Care ManagementsandraNo ratings yet
- Nursing Informatics: The Evolution of Data-Driven HealthcareDocument18 pagesNursing Informatics: The Evolution of Data-Driven HealthcareMelissa Marie Custodio100% (1)
- Immunization of ChildrenDocument20 pagesImmunization of ChildrenKatrina LoweNo ratings yet
- HemodialysisDocument2 pagesHemodialysisjustin_saneNo ratings yet
- Geriatic Health Care TeamDocument14 pagesGeriatic Health Care TeamKaiser AntojaNo ratings yet
- Text BookDocument696 pagesText BookMaged Saif100% (9)
- Repertory of Miasms H 36011Document32 pagesRepertory of Miasms H 36011Fazal Akhtar100% (2)
- EBN - Chicken PoxDocument5 pagesEBN - Chicken PoxGlaizalyn Fabella TagoonNo ratings yet
- Writing Task 2 - Discussion - Health Promotion or TreatmentDocument1 pageWriting Task 2 - Discussion - Health Promotion or TreatmentNguyễn Phước Hà ThiênNo ratings yet
- Test Bank For Wongs Essentials of Pediatric Nursing 11th Edition Marilyn J Hockenberry Cheryl C Rodgers David WilsonDocument7 pagesTest Bank For Wongs Essentials of Pediatric Nursing 11th Edition Marilyn J Hockenberry Cheryl C Rodgers David Wilsondennisgallegosmkrgyabsod100% (13)
- Seoul St. Mary's Hospital Dental CareDocument1 pageSeoul St. Mary's Hospital Dental CareAhmed AlhadiNo ratings yet
- Blood Sample ProcessingDocument4 pagesBlood Sample Processingkarina nilasariNo ratings yet
- Clinical Trial Feasibility ChecklistDocument3 pagesClinical Trial Feasibility ChecklistIrina NeiNo ratings yet
- Youssry L. Jaranilla MD: Talisay, Lipa City Batangas Oriental Mindoro 09303523092Document5 pagesYoussry L. Jaranilla MD: Talisay, Lipa City Batangas Oriental Mindoro 09303523092Youssry JaranillaNo ratings yet
- Kew Fdar1Document1 pageKew Fdar1Mariam JubelNo ratings yet
- NPHDocument2 pagesNPHbimaindra97No ratings yet
- DiclofenacDocument22 pagesDiclofenacintan kusumaningtyasNo ratings yet
- PDF 2479849263Document2 pagesPDF 2479849263galalNo ratings yet
- MATUCOL 3 Meses Seguridad Efectividad de Metodos de InduccionDocument11 pagesMATUCOL 3 Meses Seguridad Efectividad de Metodos de InduccionMitsury Jacqueline Flores C.No ratings yet
- Principles of Management of Open FracturesDocument24 pagesPrinciples of Management of Open FracturesdhonnaNo ratings yet