ORI GI NAL COMMUNI CATI ON
The dopaminergic system in upper limb motor blocks (ULMB)
investigated during bimanual coordination in Parkinsons disease
(PD)
Matt J. N. Brown
Quincy J. Almeida
Fariborz Rahimi
Received: 13 June 2014 / Revised: 12 September 2014 / Accepted: 19 September 2014
Springer-Verlag Berlin Heidelberg 2014
Abstract Upper limb motor blocks (ULMB) (inability to
initiate or sudden discontinue in voluntary movements)
have been identied in both unimanual and bimanual tasks
in individuals with Parkinsons disease (PD). In particular,
ULMB have been observed during rhythmic bimanual
coordination when switching between phase patterns which
is required (e.g. between in-phase and anti-phase). While
sensory-perceptual mechanisms have recently been sug-
gested to be involved in lower limb freezing, there has been
no consensus on the mechanism that evokes ULMB or
whether motor blocks respond to dopamine replacement
like other motor symptoms of PD. The current study
investigated the occurrence of ULMB in PD participants
without (off) and with (on) dopamine replacement using
bimanual wrist exionextension with external auditory
cues. In Experiment 1, coordination was performed in
either in-phase (simultaneous exion and extension) or
anti-phase (asymmetrical exion and extension between
the limbs) in one of three sensory conditions: no vision,
normal vision or augmented vision. Cycle frequency was
increased within each trial across seven cycle frequencies
(0.752 Hz). In Experiment 2, coordination was initiated in
either phase pattern and participants were cued to make an
intentional switch between phases in the middle of trials.
Trials were performed at one of two cycle frequencies (1 or
2 Hz) and one of two sensory conditions: no vision or
normal vision. Healthy age-matched control participants
were also investigated in both experiments for the occur-
rence of motor blocks that were measured using automated
detection from a computer algorithm. The results from
Experiment 1 indicated that increasing cycle frequency
resulted in more ULMB in individuals with PD during
continuous coordinated movement, regardless of dopami-
nergic status, phase pattern or sensory condition. Experi-
ment 2 also conrmed an increased occurrence of ULMB
with increased cycle frequency. Furthermore, a large
amount of ULMB were observed when initiating anti-phase
coordination at 2 Hz, as well as after both externally-cued
switches and in catch trials with distracting auditory cues
when no switch was required. Dopamine replacement was
not found to inuence the frequency of ULMB in either
experiment. Therefore, ULMB likely result from non-
hypodopaminergic impairments associated with PD. Spe-
cically, ULMB may be caused by an inability to shift
attentional control under increased cognitive demand that
could be associated with hypoactivation in motor and
prefrontal areas.
Keywords Parkinsons disease Basal ganglia
Dopamine Freezing Motor blocks Upper limb
Bimanual coordination
Introduction
Freezing, the inability to initiate, or a sudden interruption
in voluntary movements, has been identied as one of the
most debilitating symptoms of Parkinsons disease (PD)
M. J. N. Brown Q. J. Almeida (&)
Sun Life Financial Movement Disorders Research and
Rehabilitation Centre (MDRC), Wilfrid Laurier University,
75 University Avenue West, Waterloo, ON N2L 3C5, Canada
e-mail: qalmeida@wlu.ca
F. Rahimi
Department of Electrical Engineering, University of Waterloo,
200 University Avenue West, Waterloo, ON N2L 3G1, Canada
F. Rahimi
Electrical Engineering Department, University of Bonab,
Velayet Highway, East Azerbaijan, Bonab 5551761167, Iran
1 3
J Neurol
DOI 10.1007/s00415-014-7514-5
[1, 2]. Freezing has traditionally been identied in the
lower limbs (freezing of gait, FoG) in PD during specic
aspects of gait including initiation, walking through narrow
spaces or during turning [36]. In addition to FoG, several
studies have identied a similar phenomenon, upper limb
motor blocks (ULMB), in PD during rhythmic unimanual
nger tapping [7, 8] and bimanual coordination [915].
FoG is often associated with PD progression though there
has been difculty in correlating freezing with a specic
pathological mechanism [16, 17]. Our lab recently con-
ducted two experiments in which the effects of dopamine
replacement on coordination and spatiotemporal parame-
ters of rhythmic bimanual movements were assessed [18,
19], although ULMB were not specically examined. The
current study investigated the occurrence of ULMB in PD
participants without (off) and with (on) dopamine
replacement using bimanual wrist exionextension with
external auditory cues. In addition, different parameters
were manipulated during the bimanual movements such as
the type of sensory feedback available during coordination,
required cycle frequency, coordination patterns and pattern
switching to evaluate the mechanisms that could evoke
motor blocks in the upper limbs. The evaluation of ULMB
during dopaminergic modulation as well after manipulation
of these different parameters during upper limb coordina-
tion could provide insight into the role of the dopaminergic
system as it relates to the potential underlying mechanisms
contributing to ULMB.
Currently, the responsiveness of ULMB during biman-
ual movements to dopamine replacement is unknown. The
amount of motor blocks were not inuenced by dopamine
replacement during unimanual nger tapping [8]. More
recently, an investigation evaluating the number of ULMB,
which they referred to as freezing episodes, during
bimanual repetitive movements found that these episodes
were correlated with FoG scores but not disease severity in
PD, suggesting that dopaminergic system dysfunction may
not be the primary contributor to this phenomenon [11].
However, this study did conclude that upper limb freez-
ing and FoG may share a common mechanism that pro-
vokes a breakdown in coordinated movement resulting in
freezing [11]. Similarly, in a subsequent study, more
upper limb freezing episodes (i.e. ULMB) were identied
during small and fast rhythmic bimanual nger movements
rather than when PD patients moved at a comfortable pace
and amplitude [12, 14]. Thus, ULMB may be linked to
spatiotemporal parameters of movement that have previ-
ously been shown to be responsive to dopamine replace-
ment [19]. Furthermore, if ULMB and FoG share common
mechanisms then their responsiveness to dopamine
replacement should be similar. A study investigating FoG
revealed that levodopa signicantly decreased FoG fre-
quency predominantly during turning [6]. However, in the
same study, akinetic FoG (complete lack of movement)
was only identied in the PD patients off levodopa
medications [6]. These results suggest that FoG may be
responsive to dopamine replacement. Recently, different
types of FoG have been identied including off levodopa
FoG that is responsive to dopamine replacement, whereas
in other cases dopamine is argued to have no inuence on
FoG (so-called levodopa-unresponsive FoG), or actually
lead to FoG (so-called pure on FoG) [2, 6, 17, 2023].
FoG episodes that are unresponsive or evoked with dopa-
mine replacement may be linked non-hypodopaminergic
pathology involving mechanisms related to stress, cogni-
tion or sensory-perceptual impairments [3, 17, 24, 25]. It is
important to consider that several mechanisms may
underlie ULMB and subsequently, only some of these
mechanisms may respond to dopamine replacement.
Recently, hypoactivation was identied in cortical motor
and prefrontal areas during upper limb motor blocks, [13]
supporting a role for theses areas in ULMB. However, it is
unclear whether dopamine replacement can modulate these
frontal motor and cognitive networks to reduce ULMB.
The primary objective of the current study was to
determine whether ULMB in PD were responsive to
dopamine replacement. Secondary objectives were to:
(a) evaluate the occurrence of ULMB during manipulations
of frequency of movements, visual feedback, phase, and
pattern switching, (b) identify clinical and demographic
characteristics of individuals with PD that display ULMB,
and (c) characterize the type (i.e. unilateral vs. bilateral),
duration and affected limb (more vs. less affected) of
ULMB. It was hypothesized that dopamine replacement
would not signicantly reduce the occurrence of ULMB.
Methods
Participants
The methods used in both experiments and participants
have been described in detail elsewhere [18, 19]. In both
Experiment 1 and 2, 15 (n = 15) individuals with Parkin-
sons disease and 15 (n = 15) healthy age-matched adults
participated. All individuals were right-hand dominant and
evaluated on the Modied Mini-Mental State Examination
(3-MS) for signs of dementia and to ensure all individuals
had the mental capacity to perform the experiment (see
Table 1 for demographic information of participants).
In both experiments, PD participants performed the rst
session after overnight withdrawal from dopaminergic
medication. Individuals were evaluated on the motor sub-
section of the Unied Parkinsons Disease Rating Scale
(UPDRS-III) to document motor symptoms after with-
drawal from dopamine replacement (PD off). After
J Neurol
1 3
completion of the rst session, medication was self-
administered. Re-evaluation of motor symptoms occurred
after a 70 min waiting period to document the response to
dopamine replacement (PD on) (see Table 2 for clinical
characteristics of PD participants). Upper limb laterality
scores were calculated and compared for both limbs from
items 2025 on the UPDRS-III (which examine upper limb
motor symptoms) to classify the more and less affected
limbs [19]. Patient history was reviewed for symptoms of
FoG. Participants were categorized as FoG or non-FoG (as
per a previously established protocol) [3]. PD participants
were recruited from the patient database at the Sun Life
Financial Movement Disorders Research and Rehabilita-
tion Centre (MDRC) at Wilfrid Laurier University. Healthy
controls were recruited from family and friends of PD
participants. Ethics approval for the current experiment
was received from the Human Research Ethics Board
(REB) at Wilfrid Laurier University. All participants pro-
vided written consent prior to participation in the study in
accordance with the Declaration of Helsinki.
Apparatus
Briey, both experiments had participants seated in a height
adjustable chair with their forearms resting on a padded
surface and forearms constrained to avoid unwanted
movements at the elbow and shoulder joints. The forearms
were pronated 90 with the palms facing inward and thumbs
facing upwards. Movements were performed on two sepa-
rate robotic Phantom Omni haptic devices (SensAble
Technologies Inc., Woburn, MA, USA) that were syn-
chronized and linked to a desktop computer (Dell Com-
puter, with a g-force Intel Pentium 4 with SSE2) for data
recording using MatLab R2007b (The MathWorks Inc,
Nattick, MA, USA). A pen-shaped stylus was attached to a
pivoting arm that allowed for three-dimensional (3-D)
movements. Wrist exionextension movements were
performed in rhythm with a computer-generated metro-
nome using QuaRC (Quanser Inc., Markham, On, Canada).
To run all the different experimental sessions, automated
programs were created using Simulink in MatLab R2007b.
Procedure
For both experiments, participants performed wrist ex-
ionextension primarily in the mediallateral direction
with the hands grasping each stylus. However, the wrists
were not constrained allowing 3-D movements if neces-
sary. The goal of both tasks was to maintain rhythmic
coordination synchronized with the metronome. Partici-
pants were instructed to perform movements as large as
possible with both limbs, but no specic amplitude
requirements were given. In both experiments, in-phase
and anti-phase coordination patterns were used [26, 27]. In-
phase required the symmetrical movement of both limbs
with simultaneous extension and exion of the wrists using
homologous muscles. Anti-phase was performed as an
asymmetrical pattern requiring exion of one wrist and
extension of the opposite wrist using non-homologous
muscles.
In Experiment 1, three visual feedback conditions were
used: no vision, normal vision, and augmented vision. In
the normal vision condition participants were able to see
their moving limbs. The no vision condition involved the
removal of vision by blindfolding participants. In the
augmented vision condition moving limbs were covered
by a custom-made apparatus but information of the
moving limbs was provided using a modied Lissajous
gure on the computer monitor (see [19] for more
details). A dynamic cycle frequency protocol was used to
set the cycle frequency for each trial, where the cycle
frequency was gradually increased from 0.75 to 2 Hz at
set intervals. Each trial lasted 50 s beginning with a
resting period of 5 s. Each phase and sensory feedback
manipulation was randomly performed and resulted in a
total of 18 trials within each session. Each participant
performed a total of 36 trials over 2 sessions (i.e. off vs.
on).
In Experiment 2, participants performed in either no
vision or normal vision conditions. Participants began each
trial by performing continuous coordination in either in-
phase or anti-phase. At the midpoint of each 23-s trial, a
high-pitched auditory cue signaled individuals to perform a
Table 1 Summary of demographic information for PD and healthy age-matched control (HC) participants including age, gender and Modied
Mini-Mental State Examination (3-MS) scores
Experiment 1 Experiment 2
PD HC PD HC
N 15 15 15 15
Age (years) 68 (6.4) 65.5 (7.3) 67 (7.5) 67.8 (8.7)
Gender Male = 7, female = 8 Male = 6, female = 9 Male = 8, female = 7 Male = 5, female = 10
3-MS score (out of 100) 94.1 (5.2) 96.3 (3.7) 95.5 (4.5) 95.9 (3.0)
Years of education (years) 14.5 (3.8) 14.5 (3.8) 14.5 (3.3) 14.1 (3.3)
J Neurol
1 3
rapid and smooth transition (intentional switch) to the
opposite phase pattern without stopping. To avoid antici-
pation of the voluntary switch, the experimenter randomly
cued the beginning of trials with a verbal go signal 2, 4 or
6 s after the beginning of each trial (resulting in switches
randomly occurring 5.5, 7.5, 9.5, or 11.5 s after the initi-
ation of trials). The combination of switch, cycle frequency
and sensory condition resulted in 24 trials per session. PD
Table 2 Clinical characteristics of PD patients including motor subscale scores on Unied Parkinsons Disease Rating Scale (UPDRS-III),
dopamine medication, disease laterality and history of freezing of gait (FoG)
Participant Experiment Dopamine
medication
a
Time off
medication
(in hours)
UPDRS-III
off (score out
of 108)
a
Time on
medication
UPDRS-III
on (score out
of 108)
a
Previous
history of
FoG
b
Disease
laterality
c
Bilaterally
affected?
1 1 LD-CD 15 21 90 14.5 N L\R N
2 1 LD-CD, tri,
pram
15 38 70 30.5 Y L\R Y
3 1 LD-CD 13.5 27 90 13.5 N R\L N
4 1 LD-CD 15.5 30.5 75 22 Y L\R Y
5 1 rop, ras 17 29.5 85 17.5 N R\L N
6 1 LD-CD 13.5 41.5 70 30.5 N R\L N
7 1 LD-CD 18 42.5 70 22.5 N R\L Y
8 1 LD-CD,
ent, ras
16.5 18.5 70 10 N L\R N
9 1 LD-CD 12 46 90 35.5 N L\R Y
10 1 LD-CD 14.5 20 70 12.5 N L\R N
11 1 LD-CD, ent 16 21.5 75 12.5 Y L\R Y
12 1 LD-CD,
pram
14.5 34 70 23 Y R\L N
13 1 LD-CD 17 26.5 70 10.5 N L\R N
14 1 LD-CD,
ras, pram,
13.5 31 75 22 Y R\ Y
15 1 LD-CD 12.5 32 75 23 N \R N
16 2 LD-CD 15 32.5 70 23.5 N R\L Y
17 2 LD-CD/ent 12.5 42.5 75 32 N L\R Y
18 2 LD-CD 12 34 85 25 N L\R N
19 2 LD-CD 15 35.5 70 29 Y L\R Y
20 2 LD-CD,
pram
14 31 75 25.5 Y R\L Y
21 2 LD-CD,
rop, sel
12 39.5 75 24 Y R\L Y
22 2 LD-CD/
ent, ras
16 16 70 9 N L\R N
23 2 LD-CD 12.5 38 75 31 Y L\R Y
24 2 LD-CD 14.5 38.5 65 31.5 N R\L Y
25 2 LD-CD 12.5 47.5 90 37.5 Y R\L Y
26 2 Rop 12 32 75 23.5 N R\L Y
27 2 LD-CD 19 30 80 24.5 N L\R Y
28 2 LD-CD 21.5 15.5 75 10 N R\L N
29 2 Pram 17.5 28.5 70 18.5 N L\R N
30 2 LD-CD 14 26 70 19 N R\L Y
LD-CD levodopa-carbidopa (L-dopa/Dopa decarboxylase inhibitor), ras rasagiline (MAO-B selective agent), pram pramipexole (dopamine
receptor agonist), ent entacapone (COMT inhibitors), rop ropinirole (dopamine receptor agonist), tri trihexyphenidyl (antimuscanrinic)
a
UPDRS-III scores represent clinical evaluation on the motor subsection of the Unied Parkinsons Disease Rating Scale. Disease laterality was
based on the sum of scores on the right side compared to the left side
b
Previous history of freezing of gait was obtained from patient history on database
c
Disease laterality was based on the sum of scores of UPDRS-III on the right side compared to the left side
J Neurol
1 3
participants performed a total of 48 trials across two ses-
sions and healthy controls performed 24 trials in one ses-
sion. In addition, to rule out that the high-pitched auditory
cue did not act as a distractor provoking ULMB, before
each experimental session participants performed six catch
trials (3 at 1 Hz and 3 at 2 Hz). These trials had partici-
pants perform continuous coordination in anti-phase for
23 s where at the midpoint a high-pitched auditory cue
would occur but without instructions to voluntarily switch
between patterns.
Data processing and analysis
For both experiments, displacement data was collected at a
rate of 1,000 Hz from each haptic device and stored for
ofine analysis using MatLab. Displacement data was used
to calculate coordination accuracy, coordination stability,
limb frequencies and limb amplitudes [18, 19]. The
movement amplitude of each limb was used for analyzing
ULMB.
The current study classied motor blocks using criteria
that combined previous denitions. Freezing in the
upper limbs have previously been classied based on at
least 1 s of no change in movement amplitude [9, 10].
However, recent research in freezing of gait has indicated
that total cessation in movement does not always occur
with a freeze [28]. Thus, the denition for upper limb
freezing was recently modied to incorporate either a
reduction in amplitude (less than 50 % of regular ampli-
tude) prior to a freeze or irregular cyclic movement [11,
12, 14, 28]. Thus, in both experiments ULMB were
dened as a 75 % reduction of amplitude for at least 1 s.
The current denition of motor blocks allowed classi-
cation of ULMB that did not produce a total arrest in
movement.
In both experiments, detection of motor blocks was
automated using a script created in MatLab R2007b. All
motor blocks that were detected by the computer algorithm
were visually inspected on displacement proles to ensure
that ULMB were accurately detected with the automated
script. Visual inspection was performed to conrm that the
automated script did not incorrectly classify irregular
movements as ULMB. Voluntary stops were analyzed and
documented during each collection to ensure that motor
blocks were not falsely identied as intentional arrests in
movement (and vice versa). A voluntary stop was dened
as any discontinued movement that was not preceded by a
reduction in amplitude [11]. These could occur in re-
establishing coordination after a transition, early termina-
tion of movement at the end of a trial, or during trials due
to equipment restrictions. During the testing sessions, two
investigators recorded any time distinct voluntary stops
occurred.
In Experiment 1, ULMB were detected using the peak-
to-peak amplitude of each cycle measured over a trial and
compared to the reference amplitude. The reference
amplitude of movement was obtained from the mean peak-
to-peak amplitude within each trial when participants were
moving at 1 Hz. Thus, ULMB were classied as a 75 %
reduction in amplitude compared to the reference ampli-
tude for at least 1 s.
In Experiment 2, the reference amplitude was modied
from Experiment 1 for two reasons. Unlike Experiment 1,
not all trials had movements at 1 Hz and motor blocks were
extremely prominent at 2 Hz. Furthermore, the investiga-
tors noted that in some trials participants were blocked for
nearly the whole duration of a trial, which eliminated the
ability to use the reference amplitude within each trial
similar to Experiment 1. As a consequence, the mean
amplitude was calculated over 4 s within each trial before
the cue to switch (from 6 to 10 s). The trial with the largest
maximum amplitude (over these 4 s) was used as the ref-
erence amplitude, separately for each limb and dopami-
nergic status.
Chi-square analyses compared the amount of ULMB
based on dopaminergic status, sensory condition, phase and
cycle frequency in both experiments. T tests were also used
to evaluate whether the duration of motor blocks differed in
PD patients off compared to on. In Experiment 2,
ULMB were separated both before and after voluntary
transitions. In addition, the amount of motor blocks was
documented in catch trials after the auditory cue. An a
level of 0.05 was used to dene statistical signicance. In
the event of signicance between more than two variables
for either cycle frequency or sensory condition, individual
Chi-square tests were performed to determine which fac-
tors were different.
Results
Occurrence and characteristics of ULMB
and individuals with PD experiencing ULMB
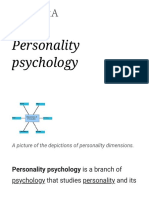
An example of a motor block is displayed in Fig. 1. In
Experiment 1, at least one motor block was documented in
six out of 15 PD participants (3 more affected on left side
and 3 more affected on right side). Only two out of the six
were classied as FoG (compared to 3 out of 9 who did not
display ULMB were identied as FoG). The duration of
ULMB ranged from 1.27 to 14.51 s with an average length
of 2.75 (2.4) s. No signicant difference in the duration
of ULMB were revealed between PD off
(mean = 2.80 s) and on (mean = 2.71 s) (t (38) = 0.10
p = 0.92). Table 3 presents the breakdown of ULMB by
the limb(s) they were evoked and dopaminergic status.
J Neurol
1 3
In Experiment 2, ULMB were identied before the cue
to switch in 5 out of 15 PD participants. Only one out of the
ve was classied as a FoG and all were more affected on
the left side. The duration of ULMB ranged from 1.2 to
5.2 s (mean = 2.6 1.2 s). No signicant differences in
the duration of ULMB was determined between PD off
(mean = 2.59) and on (mean = 2.76) (t (50) = -0.43,
p = 0.67). After the cue to switch, ULMB were identied
in 8 out of 15 PD participants (6 more affected on the left
side and considered bilaterally affected). Only three out of
eight that displayed ULMB were identied as FoG (com-
pared to 2 out of 7 who did not display ULMB were FoG).
The duration of ULMB ranged from 1.1 to 9.1 s
(3.02 1.9 s). No signicant differences were observed in
the duration of ULMB between PD off (mean = 3.09 s)
compared to PD on (mean = 3.11 s) (t (95) = -0.05,
p = 0.96). Tables 4 and 5 presents the breakdown of
ULMB by the limb(s) they were evoked and dopaminergic
status before and after the cue to switch phase patterns,
respectively.
It should be noted that three motor blocks were
identied in healthy control participants after the cue to
switch in Experiment 2. Based on visual inspection, these
trials represented short voluntary stops, which were not
preceded by amplitude reductions (see Fig. 2). As a con-
sequence, these episodes were not classied as ULMB. In
PD, 41 ULMB were identied within the transition period
after the cue to switch. However, 12 out of the 41 episodes
(29.3 %) were classied as delayed responses. As a con-
sequence, 17 trials remained where motor blocks may have
Fig. 1 (top) An example of a
motor block in the more
affected left limb of PD non-
FOG (below) red line illustrates
the point when all the criteria
were met for a ULMB by the
computer algorithm. Green line
represents the beginning of the
motor block, while the end of
the motor block was represented
by the end of the trial
Table 3 Breakdown of ULMB detected using computer-algorithm and visually veried in PD both off and on dopaminergic medication in
Experiment 1
PD off PD on
More affected
a
Less affected
a
Both limbs
a
Total
a
More affected
a
Less affected
a
Both limbs
a
Total
a
Total ULMB 18 (13) 1 (1) 0 19 (14) 14 (9) 3 (2) 4 (4) 21 (15)
% of total trials
b
4.8 0.04 0 5.2 3.3 0.07 1.5 5.6
% of total ULMB
c
40.9 2.3 0 43.2 31.8 6.8 9.1 47.7
a
Out of brackets represents all motor blocks including when multiple motor blocks occurred in the same trial. In brackets, represents the total
number of trials which an ULMB occurred
b
Percentage (%) is calculated by dividing motor blocks (excluding motor blocks when multiple blocks occurred) by total trials of each
dopaminergic status (n = 270)
c
Percentage (%) is calculated from all motor blocks including when multiple motor blocks occurred (n = 40 motor blocks)
J Neurol
1 3
Table 4 The amount of ULMB before pattern switching in PD participants in Experiment 2
PD off PD on
More affected
a
Less affected
a
Both limbs
a
Total
a
More affected
a
Less affected
a
Both limbs
a
Total
a
Total ULMB 24 (20) 0 (0) 1 (1) 25 (21) 27 (22) 0 (0) 0 (0) 27 (22)
% of total trials
b
5.6 0 0.28 5.88 6.1 0 0 6.1
% of total ULMB
c
45.3 0 1.9 47.2 50.9 0 0 50.9
a
Out of brackets represents all ULMB including when multiple motor blocks occurred in the same trial. In brackets, only represents the total
number of trials which an ULMB occurred
b
Percentage (%) is calculated by dividing motor blocks (excluding motor blocks when multiple ULMB occurred) by total trials of each
dopaminergic status (n = 360)
c
Percentage (%) is calculated from dividing motor blocks by all ULMB (n = 52 motor blocks) including when multiple ULMB occurred in
same trial and both limbs blocked at same time
Table 5 The amount of ULMB after pattern switching in PD participants in Experiment 2
PD off PD on
More affected
a
Less affected
a
Both limbs
a
Total
a
More affected
a
Less affected
a
Both limbs
a
Total
a
Total ULMB 41 (31) 1 (1) 5 (5) 47 (37) 49 (28) 1 (1) 0 (0) 50 (29)
% of total trials
b
8.6 0.06 1.7 10.6 7.8 0.06 0 8.3
% of total ULMB
c
40.2 0.09 4.9 45.2 48.0 0.09 0 48.09
a
Out of brackets represents all ULMB including when multiple motor blocks occurred in the same trial. In brackets, represents the total number
of trials which an ULMB occurred
b
Percentage (%) is calculated by dividing ULMB (excluding motor blocks when multiple ULMB occurred) by total trials of each dopaminergic
status (n = 360)
c
Percentage (%) is calculated from dividing motor blocks by all ULMB (n = 97 ULMB) including when multiple ULMB occurred in same trial
and both limbs blocked at same time
Fig. 2 (top) An example of a
motor block detected in the
right limb during a transition in
a healthy control (below) red
line represents the point when
all the criteria were met for a
ULMB by the computer
algorithm. Green lines illustrate
when the computer algorithm
detected the motor block
J Neurol
1 3
occurred within the transition period. However, none of
these ULMB could clearly be identied based on visual
inspection since amplitude reductions would have occurred
to perform transitions. In addition, these transitional
ULMB appeared similar in some circumstances to the
motor blocks detected in healthy controls (see Fig. 3).
Thus, ULMB after the cue to switch phase patterns in
Experiment 2 only represents trials where ULMB did not
occur during the transition period and could clearly be
identied as ULMB (Fig. 4).
In the catch trials used in Experiment 2, ULMB were
identied 64 trials in PD participants after the distracting
auditory cue when no switch occurred. Only 41 out of 64
were visually conrmed as ULMB. Several of these trials
were veried as small voluntary stops with the auditory cue
that were noted by the investigators during testing and
Fig. 3 (top) An example of PD
motor block detected in the
less affected left limb during the
transition period (below) red
line represents the point when
all the criteria were met for a
ULMB by the computer
algorithm. Green lines illustrate
when the motor block was
detected by the computer
algorithm
Fig. 4 (top) An example of a
multiple ULMB after a pattern
switch from anti-phase to in-
phase in the more affected limb
of PD (below) blue lines
represent periods of decreased
amplitude that did not last 1 s.
Red lines illustrate the points
when all the criteria were met
for a ULMB by the computer
algorithm. Green lines represent
the beginning and end of each
motor block. The second motor
block terminated at the end of
the trial
J Neurol
1 3
veried during analysis as they were not preceded by
amplitude reductions.
Multiple ULMB occurred in the same trial in 8 out of 41
(19.5 %) trials. Both limbs froze in 3 out of 41 (7.3 %) of
trials. As a result, ULMB were identied in 17 separate
trials out of 90 (18.9 %) total catch trials of PD
participants.
Effects of dopamine replacement, sensory conditions,
phase pattern and cycle frequency on ULMB
In Experiment 1, only cycle frequency was found to sig-
nicantly increase the amount of ULMB (v
2
(5) = 34.6,
p \0.001). Individual comparisons using Chi-square tests
revealed that more motor blocks occurred at 1.75 (n = 15)
and 2 Hz (n = 14) compared to the three slowest cycle
frequencies (0.75 Hz (n = 0), 1 Hz (n = 1) and 1.25 Hz
(n = 3)). Additionally, more motor blocks occurred at
1.5 Hz (n = 7) compared to the two slowest cycle fre-
quencies (0.75 and 1 Hz). Importantly, no effects of sen-
sory condition, phase pattern or dopamine replacement
(off n = 19 vs. on n = 21) were observed.
In Experiment 2 before the cue to switch, analyses
revealed that cycle frequency signicantly increased the
amount of ULMB (v
2
(1) = 19.6, p \0.001) as more
ULMB were identied in trials at 2 Hz (n = 41) compared
to 1 Hz (n = 11). In addition, phase signicantly inu-
enced the amount of ULMB (v
2
(1) = 14.8, p \0.001)
revealing more ULMB during anti-phase (n = 40) com-
pared to in-phase (n = 12). The four combinations of cycle
frequency and phase were also compared. Chi-square
analysis found a signicant effect (v
2
(3) = 32.4,
p \0.001) demonstrating that more ULMB occurred dur-
ing anti-phase coordination at 2 Hz (n = 29) compared to
during anti-phase coordination at 1 Hz (n = 11) or in-
phase coordination at 2 Hz (n = 12). No ULMB were
documented during in-phase coordination at 1 Hz. No
signicant differences on the amount of ULMB were
observed with dopamine replacement (off n = 25 vs. on
n = 27) or sensory condition (no vision n = 30 vs. normal
vision n = 22).
In Experiment 2 after the cue to switch, Chi-square
analysis indicated that cycle frequency had a signicant
inuence on the amount of motor blocks (v
2
(1) = 24.2,
p \0.001). Overall, more ULMB were identied at 2 Hz
(n = 72) compared to 1 Hz (n = 25). In addition, there
was a signicant inuence of phase on the number of
ULMB (v
2
(1) = 10.3, p \0.001) as more ULMB were
identied after switching to and performing anti-phase
(n = 64) compared to in-phase (n = 33). No effects of
dopamine replacement (off n = 47vs. on n = 50) or
sensory condition (no vision n = 53 vs. normal vision
n = 44) were revealed on the occurrence of ULMB
(p [0.05).
Discussion
The primary objective of the current study was to evaluate
the responsiveness of ULMB to dopaminergic treatment. A
secondary objective was to evaluate how potential mech-
anisms contributing to ULMB might be involved in this
responsiveness, by manipulating sensory feedback,
required cycle frequency, phase pattern and pattern
switching during coordination. The novel nding of the
current study was that there was no signicant difference in
the frequency or duration of ULMB between PD off and
on dopamine replacement during bimanual coordination.
Furthermore, increased cycle frequency, anti-phase coor-
dination, cued-switching to anti-phase coordination (from
in-phase) all contributed to signicant increase in ULMB.
Interestingly, sensory feedback had no inuence on the
occurrence of ULMB.
Dopaminergic system and ULMB
The current ndings demonstrating neither difference in
the number nor duration of ULMB between PD off and
on dopamine replacement is in agreement with previous
research that identied manual motor blocks during uni-
manual nger tapping were also not dopa-responsive [8].
These results seem to suggest that ULMB is primarily
evoked by mechanism(s) outside the hypodopaminergic
system that are not ameliorated by dopamine replacement.
Although there have been conicting results in FoG [2,
6, 17, 2023], there is some evidence that dopamine
replacement can decrease the occurrence and spatiotem-
poral precursors of FoG [6, 20, 21]. In addition, the prev-
alence of episodes of akinetic FoG (complete absence of
movement) were only documented in PD off state after
dopaminergic withdrawal [6]. It is likely that these epi-
sodes (i.e. akinetic FoG) could be classied as FoG that is
responsive to dopamine replacement whereas other types
of FoG are unresponsive to levodopa or even emerge only
after levodopa [17, 29]. Thus, these results would support
that the mechanisms underlying ULMB are potentially
shared with the mechanisms underlying FoG that are
unresponsive to levodopa therapy.
Neural networks contributing to ULMB
Surprisingly, only ve out of the total 14 individuals with
PD that displayed ULMB that were identied in both the
current experiments had a history of FoG. This result is
conicting with a previous report [11], which found that
J Neurol
1 3
the amount of upper limb freezing episodes were corre-
lated with scores on a freezing of gait questionnaire in
individuals with PD, suggesting freezing shares a common
mechanism. It should be noted that we did not directly
examine FoG in our patients. However, some of the
patients used in the current experiment have been identied
as FoG in other experiments in our lab [3, 4]. Thus, our
results suggest that FoG and ULMB do not necessarily
share a common mechanism. It may be possible that
ULMB may precede FoG in individuals with PD as pre-
viously suggested [11]. If this were the case, this would
support ULMB as a predictor of the future development of
FoG [14]. Alternatively, ULMB and FoG could be linked
to different neural mechanisms.
Recently, a functional imaging study investigating
motor arrests while walking in a virtual reality environment
in PD patients determined that these episodes were asso-
ciated with impaired processing in prefrontal (increased
BOLD signals), posterior parietal (increased BOLD sig-
nals), basal ganglia (decreased BOLD signal), sensorimotor
(decreased BOLD signals), and brainstem mesencephalic
locomotor (MCL) regions (decreased BOLD signals) [30].
In contrast, functional imaging of upper limb motor blocks
in PD patients determined that these episodes were asso-
ciated with altered activity in cortical motor areas
(increased BOLD signals), striatum (decreased BOLD
signals) and anterior prefrontal cortex (increased BOLD
signals) but not brainstem MCL [13]. Based on these
neuroimaging studies, it is plausible that cortical prefrontal
and motor networks may be involved in both ULMB and
FoG. However, specic involvement of posterior parietal
cortex, STN and brainstem areas such as MCL and PPN
may solely contribute to FoG.
Potential mechanisms contributing to ULMB
Surprisingly, the manipulation of sensory feedback had no
inuence on the occurrence of ULMB in either of the
current experiments. Previous research has suggested that
sensory-perceptual impairments may contribute to FoG [2,
3, 17]. However, visual sensory-perceptual impairments do
not appear to be a primary contributor to ULMB based on
our results, nor do they appear to respond to dopaminergic
treatment during bimanual coordination. In both Experi-
ment 1 and Experiment 2, the largest amount of ULMB
occurred when cycle frequency was at or approached 2 Hz.
In Experiment 1, 36 out of the 40 ULMB occurred at cycle
frequencies between 1.52 Hz. In Experiment 2, 113 out of
149 ULMB occurred at 2 Hz. Previous research has iden-
tied an increased amount of upper limb freezing epi-
sodes during fast (50 % faster than normal cadence) as well
as fast and small (5 vs. 10 cm) bilateral alternating
movements [15]. These results were in contrast to previous
studies that did not nd signicant differences between the
amount of upper limb freezing during normal and fast-
paced bimanual nger coordination [11, 14]. However, it
was previously demonstrated that upper limb freezing
episodes were preceded by high frequency hastening that
included an increase in frequency and decrease in ampli-
tude prior to freezing episodes [14]. Based on the spa-
tiotemporal parameters previously reported [19], overall
amplitudes of movements in PD were small, while fre-
quency of movements was similar to aged-matched con-
trols. Thus, it may be possible that in particular
circumstances the small amplitude-high frequency move-
ments provoke ULMB. This observation would be in line
with previous research in FoG that reduced stride length
and increased stepping frequency precedes FoG [1, 20].
Given that in-phase coordination is well known to be the
preferred mode of coordination (as compared to anti-phase)
due to the tight temporal-spatial coupling between
homologous muscles, one possible explanation of the
increased occurrence of ULMB during anti-phase com-
pared to in-phase coordination (Experiment 2) could be
related to decient movement lateralization (i.e. increased
mirrored activity) in PD [3134]. Several studies investi-
gating unilateral upper limb movements in PD, particularly
with lateralized or hemiParkisonian features, have found
that there is increased movement or EMG activity in the
resting limb, reective of mirror movements (MM) [31
35]. Interestingly, MM are more pronounced in the less
affected limb rather than affected limb in PD, which point
to increased M1 activity that results from decreased
transcallosal inhibition (or increased excitation) [32, 33].
Furthermore, increased MM have been observed in the less
affected limb when PD patients move at cycle frequencies
between 0.52 Hz compared to 2.53 Hz [31], as in the
current experiments. Thus, if impaired movement laterali-
zation particularly during anti-phase coordination were
responsible for evoking ULMB, then motor blocks would
be expected to be more prevalent in the less rather than
more affected limb during bimanual coordination. How-
ever, nearly all ULMB in the current experiments were
identied in the more affected limb suggesting this is not a
likely mechanism for provoking motor blocks.
Alternatively, the increased ULMB could be related
attentional demand imposed by auditory cueing and/or
anti-phase coordination. In both experiments, increased
cycle frequency (Experiments 1 and 2) and anti-phase
coordination (Experiment 2) were associated to increase
ULMB. Previous research did not reveal increased upper
limb freezing during anti-phase or high-frequency
movements during bimanual nger coordination [14].
However, auditory pacing in this study [14] only occurred
for the rst six movement cycles then coordination was
internally generated without auditory cues unlike the
J Neurol
1 3
continuous cues provided in our experiments. It has pre-
viously been suggested that anti-phase coordination
requires greater attentional resources than in-phase coor-
dination [3638]. Furthermore, it has been suggested that
external cueing during anti-phase coordination increases
the complexity of the task [39]. Interestingly, in a previous
study all but one upper limb freezing episodes were
documented during rhythmic nger bimanual coordination
after auditory cues were removed within trials [12]. Fur-
thermore, PD with FoG demonstrated signicantly smaller
as well as increased frequency error, frequency variability,
relative phase error and relative phase variability after
removal of the auditory cues suggesting that PD with FoG
benet and are dependent on external cues [12]. However,
based on this study [12], it is unclear how many upper limb
freezing episodes may have been provoked by the
removal of the auditory cue itself.
In Experiment 2, the largest amount of ULMB (n = 97)
were identied after the cue to transition between coordi-
nation patterns. It has previously been found that voluntary
pattern switching from in-phase to anti-phase (compared to
anti-phase to in-phase) resulted in a greater occurrence of
upper limb freezing (53.9 % compared to 15.5 %) [9].
These ndings are in line with the notion that phase
switching, particularly when there was an increased dif-
culty after de-stabilizing in-phase coordination, requires
increased cognitive demand resulting in movement inter-
ruptions [9]. However, these effects may not necessarily be
unique to switching between coordination patterns as
results of Experiment 2 also found that distracting auditory
cues during catch trials also led to a considerable amount of
ULMB (n = 41). Thus, it may be possible that the key
contributor to provoking ULMB is the shifting of atten-
tional resources rather than a sensory-perceptual impair-
ment. It should be noted that the dynamic cycle frequency
increases used in Experiment 1 would have also included
attentional shifts when each new cueing frequency was
implemented. Sharing or shifting of attentional resources as
well as suppressing behaviours are both related to execu-
tive function of the prefrontal cortex, that can be affected in
PD. [40, 41] As previously reviewed, altered processing
have been identied in the prefrontal cortex during both
upper and lower limb motor blocks [13, 30]. Furthermore, a
functional imaging study investigating the effects of high
cognitive loads on motor arrests in PD patients while
walking in virtual reality found that motor arrests were
associated with decreased functional connectivity between
both the right and left cognitive control networks (CCN)
(between the dorsolateral prefrontal cortex and posterior
parietal cortex) as well as basal ganglia [42]. Specically
during pre-arrest periods, a decreased functional connec-
tivity was revealed between the right CCN and basal
ganglia [42]. It was concluded that abnormal
communication between the left and right CCN as well as
right CCN and basal ganglia during periods of high cog-
nitive load and low dopamine underlie FoG [42]. Based on
these ndings, if a similar neural network is involved in
ULMB, then it would suggest that ULMB do not neces-
sarily occur due to shifting between motor sets but rather
due to increased attention demand that can be produced
when having to shift attention between both motor and
sensory demands.
Conclusion
The occurrence or duration of ULMB were not decreased
after administration of dopamine replacement, suggesting
non-hypodopaminergic PD neuropathology is likely
responsible for ULMB. Furthermore, an increased occur-
rence of ULMB was associated with increased cycle fre-
quencies, anti-phase coordination, switching between
coordination patterns, and distracting auditory cues during
continuous coordination. These results suggest a signicant
decit in PD in shifting attentional resources with
increased motor and sensory demands may underlie
ULMB. This may be associated with the decreased func-
tional connectivity between right and left CCN as well as
right CCN and basal ganglia that has been associated with
motor arrests in the lower limbs [42]. It is likely that the
inability to adequately shift attentional resources evoked a
breakdown to small amplitude-high frequency movements
that was previously shown to precede upper limb freezing
[14]. Future neuroimaging research should be directed at
examining the functional connectivity between the CCN
and basal ganglia during ULMB. In addition, future
research should examine whether different types of ULMB
may exist and its relationship with different forms of FoG.
Acknowledgments We would like to thank both Dr. Alice Nie-
uwboer and Dr. Sarah Vercruysse from University of Leuven for
providing their denition and examples of upper limb freezing in a
personal communication before publication. This project was sup-
ported by National Science and Engineering Research Council
(NSERC) scholarship to the rst author, North American Society for
Psychology of Sport and Physical Activity (NASPSPA) Graduate
Student Award to the rst author, NSERC grant to the second author
and Canadian Fund for Innovation (CFI) grant to second author.
Conicts of interests On behalf of all authors, the corresponding
author states that there is no conict of interest.
References
1. Nieuwboer A, De Weerdt W, Desloovere K et al (2001) Abnor-
malities of the spatiotemporal characteristics of gait at the onset
of freezing in Parkinsons disease. Mov Disord 16:10661075.
doi:10.1002/mds.1206
J Neurol
1 3
2. Nutt JG, Bloem BR, Giladi N et al (2011) Freezing of gait:
moving forward on a mysterious clinical phenomenon. Lancet
Neurol 10:734744. doi:10.1016/S1474-4422(11)70143-0
3. Almeida QJ, Lebold CA (2010) Freezing of gait in Parkinsons
disease: a perceptual cause for a motor impairment? J Neurol
Neurosurg Psychiatry 81:513518. doi:10.1136/jnnp.2008.
160580
4. Bhatt H, Pieruccini-Faria F, Almeida QJ (2013) Dynamics of
turning sharpness inuences freezing of gait in Parkinsons dis-
ease. Parkinsonism Relat Disord 19:181185. doi:10.1016/j.park
reldis.2012.09.006
5. Giladi N, McMahon D, Przedborski S et al (1992) Motor blocks
in Parkinsons disease. Neurology 42:333339
6. Schaafsma JD, Balash Y, Gurevich T et al (2003) Characteriza-
tion of freezing of gait subtypes and the response of each to
levodopa in Parkinsons disease. Eur J Neurol 10:391398
7. Nakamura R, Nagasaki H, Narabayashi H (1978) Disturbances of
rhythm formation in patients with Parkinsons disease: part 1.
Characteristics of tapping response to the periodic signals. Per-
cept Mot Skills 46:6375
8. Ziv I, Avraham M, Dabby R et al (1999) Earlv-occurrence of
manual motor blocks in Parkinsons disease : a quantitative
assessment. Acta Neurol Scand 99:106111
9. Almeida QJ, Wishart LR, Lee TD (2003) Disruptive inuences of
a cued voluntary shift on coordinated movement in Parkinsons
disease. Neuropsychologia 41:442452
10. Almeida QJ, Wishart LR, Lee TD (2002) Bimanual coordination
decits with Parkinsons disease : the inuence of movement
speed and external cueing. Mov Disord 17:3037. doi:10.1002/
mds.10030
11. Nieuwboer A, Vercruysse S, Feys P et al (2009) Upper limb
movement interruptions are correlated to freezing of gait in
Parkinsons disease. Eur J Neurosci 29:14221430. doi:10.1111/j.
1460-9568.2009.06681.x
12. Vercruysse S, Spildooren J, Heremans E et al (2012) Abnor-
malities and cue dependence of rhythmical upper-limb move-
ments in Parkinson patients with freezing of gait. Neurorehabil
Neural Repair 26:636645. doi:10.1177/1545968311431964
13. Vercruysse S, Spildooren J, Heremans E et al (2013) The neural
correlates of upper limb motor blocks in Parkinsons disease and
their relation to freezing of gait. Cereb Cortex. doi:10.1093/cer
cor/bht170
14. Vercruysse S, Spildooren J, Heremans E et al (2012) Freezing in
Parkinsons disease: a spatiotemporal motor disorder beyond gait.
Mov Disord 27:254263. doi:10.1002/mds.24015
15. Williams AJ, Peterson DS, Ionno M et al (2013) Upper extremity
freezing and dyscoordination in Parkinsons disease: effects of
amplitude and cadence manipulations. Parkinsons Dis. doi:10.
1155/2013/595378
16. Lees AJ (2007) Unresolved issues relating to the shaking palsy on
the celebration of James Parkinsons 250th birthday. Mov Disord
22:S327S334. doi:10.1002/mds.21684
17. Heremans E, Nieuwboer A, Vercruysse S (2013) Freezing of gait
in Parkinsons disease: where are we now? Curr Neurol Neurosci
Rep 13:350. doi:10.1007/s11910-013-0350-7
18. Brown MJN, Almeida QJ (2011) Evaluating dopaminergic sys-
tem contributions to cued pattern switching during bimanual
coordination. Eur J Neurosci 34:632640. doi:10.1111/j.1460-
9568.2011.07773.x
19. Almeida QJ, Brown MJN (2013) Is DOPA-responsive hypoki-
nesia responsible for bimanual coordination decits in Parkin-
sons disease? Front Neurol 4:117. doi:10.3389/fneur.2013.
00089
20. Iansek R, Huxham F, McGinley J (2006) The sequence effect and
gait festination in Parkinson disease: contributors to freezing of
gait? Mov Disord 21:14191424. doi:10.1002/mds.20998
21. Okuma Y (2006) Freezing of gait in Parkinsons disease. J Neurol
253:VII27VII32. doi:10.1007/s00415-006-7007-2
22. Bloem BR, Hausdorff JM, Visser JE, Giladi N (2004) Falls and
freezing of gait in Parkinsons disease: a review of two inter-
connected, episodic phenomena. Mov Disord 19:871884. doi:10.
1002/mds.20115
23. Nomoto M, Nagai M (2006) Pharmacological consideration of
the symptoms resistant to dopaminergic therapy. Parkinsonism
Relat Disord 12:S83S87. doi:10.1016/j.parkreldis.2006.05.
025
24. Giladi N, Hausdorff JM (2006) The role of mental function in the
pathogenesis of freezing of gait in Parkinsons disease. J Neurol
Sci 248:173176. doi:10.1016/j.jns.2006.05.015
25. Vercruysse S, Devos H, Munks L et al (2012) Explaining freezing
of gait in Parkinsons disease: motor and cognitive determinants.
Mov Disord 27:16441651. doi:10.1002/mds.25183
26. Kelso JAS, Southard DL, Goodman D (1979) On the nature of
human interlimb coordination. Science 203:10291031
27. Kelso J, Holt K, Rubin P, Kugler P (1981) Patterns of human
interlimb coordination emerge from the properties of non-linear,
limit-cycle oscillatory processes- theory and data. J Mot Behav
13:226261
28. Giladi N, Nieuwboer A (2008) Understanding and treating
freezing of gait in parkinsonism, proposed working denition,
and setting the stage. Mov Disord 23(Suppl 2):S423S425.
doi:10.1002/mds.21927
29. Espay AJ, Fasano A, van Nuenen BFL et al (2012) On state
freezing of gait in Parkinson disease: a paradoxical levodopa-
induced complication. Neurology 78:454457. doi:10.1212/
WNL.0b013e3182477ec0
30. Shine JM, Matar E, Ward PB et al (2013) Exploring the cortical
and subcortical functional magnetic resonance imaging changes
associated with freezing in Parkinsons disease. Brain
136:12041215. doi:10.1093/brain/awt049
31. Van den Berg C, Beek PJ, Wagenaar RC, van Wieringen PCW
(2000) Coordination disorders in patients with Parkinsons dis-
ease: a study of paced rhythmic forearm movements. Exp Brain
Res 134:174186. doi:10.1007/s002210000441
32. Vidal JS, Derkinderen P, Vidaihet M et al (2003) Mirror move-
ments of the non-affected hand in hemiparkinsonian patients: a
reection of ipsilateral motor overactivity? J Neurol Neurosurg
Psychiatry 74:13521353
33. Espay AJ, Li J-Y, Johnston L et al (2005) Mirror movements in
parkinsonism: evaluation of a new clinical sign. J Neurol Neu-
rosurg Psychiatry 76:13551358. doi:10.1136/jnnp.2005.062950
34. Cincotta M, Borgheresi A, Balestrieri F et al (2006) Mechanisms
underlying mirror movements in Parkinsons disease: a trans-
cranial magnetic stimulation study. Mov Disord 21:10191025.
doi:10.1002/mds.20850
35. Kishore A, Espay AJ, Marras C et al (2007) Unilateral versus
bilateral tasks in early asymmetric Parkinsons disease: differ-
ential effects on bradykinesia. Mov Disord 22:328333. doi:10.
1002/mds.21238
36. Temprado J-J, Zanone P-G, Monno A, Laurent M (1999)
Attentional load associated with performing and stabilizing pre-
ferred bimanual patterns. J Exp Psychol Hum Percept Perform
25:15791594. doi:10.1037//0096-1523.25.6.1579
37. Stinear JW, Byblow WD (2001) Phase transitions and postural
deviations during bimanual kinesthetic tracking. Exp Brain Res
137:467477. doi:10.1007/s002210000665
38. Ridderikhoff A, Peper CLE, Beek PJ (2008) Attentional loads
associated with interlimb interactions underlying rhythmic
bimanual coordination. Cognition 109:372388. doi:10.1016/j.
cognition.2008.10.002
39. Johnson KA, Cunnington R, Bradshaw JL et al (1998) Bimanual
co-ordination in Parkinsons disease. Brain 121:743753
J Neurol
1 3
40. Rodriguez-Oroz MC, Jahanshahi M, Krack P et al (2009) Initial
clinical manifestations of Parkinsons disease: features and
pathophysiological mechanisms. Lancet Neurol 8:11281139.
doi:10.1016/S1474-4422(09)70293-5
41. Brown RG, Marsden CD (1988) Internal versus external cues and
the control of attention in Parkinsons disease. Brain 111:323345
42. Shine JM, Matar E, Ward PB et al (2013) Freezing of gait in
Parkinsons disease is associated with functional decoupling
between the cognitive control network and the basal ganglia.
Brain 1:111. doi:10.1093/brain/awt272
J Neurol
1 3
You might also like
- tmp3CAB TMPDocument16 pagestmp3CAB TMPFrontiersNo ratings yet
- tmpEFCC TMPDocument6 pagestmpEFCC TMPFrontiersNo ratings yet
- tmpCE8C TMPDocument19 pagestmpCE8C TMPFrontiersNo ratings yet
- Tmp1a96 TMPDocument80 pagesTmp1a96 TMPFrontiersNo ratings yet
- tmpF178 TMPDocument15 pagestmpF178 TMPFrontiersNo ratings yet
- tmp80F6 TMPDocument24 pagestmp80F6 TMPFrontiersNo ratings yet
- tmp6F0E TMPDocument12 pagestmp6F0E TMPFrontiersNo ratings yet
- Tmpa077 TMPDocument15 pagesTmpa077 TMPFrontiersNo ratings yet
- tmp60EF TMPDocument20 pagestmp60EF TMPFrontiersNo ratings yet
- tmpE7E9 TMPDocument14 pagestmpE7E9 TMPFrontiersNo ratings yet
- tmpFFE0 TMPDocument6 pagestmpFFE0 TMPFrontiersNo ratings yet
- tmp6382 TMPDocument8 pagestmp6382 TMPFrontiersNo ratings yet
- tmpF407 TMPDocument17 pagestmpF407 TMPFrontiersNo ratings yet
- tmpF3B5 TMPDocument15 pagestmpF3B5 TMPFrontiersNo ratings yet
- tmpE3C0 TMPDocument17 pagestmpE3C0 TMPFrontiersNo ratings yet
- tmp37B8 TMPDocument9 pagestmp37B8 TMPFrontiersNo ratings yet
- tmp72FE TMPDocument8 pagestmp72FE TMPFrontiersNo ratings yet
- tmpC0A TMPDocument9 pagestmpC0A TMPFrontiersNo ratings yet
- Tmp75a7 TMPDocument8 pagesTmp75a7 TMPFrontiersNo ratings yet
- tmp8B94 TMPDocument9 pagestmp8B94 TMPFrontiersNo ratings yet
- tmp998 TMPDocument9 pagestmp998 TMPFrontiersNo ratings yet
- tmp27C1 TMPDocument5 pagestmp27C1 TMPFrontiersNo ratings yet
- tmp9D75 TMPDocument9 pagestmp9D75 TMPFrontiersNo ratings yet
- tmp4B57 TMPDocument9 pagestmp4B57 TMPFrontiersNo ratings yet
- tmpD1FE TMPDocument6 pagestmpD1FE TMPFrontiersNo ratings yet
- tmpA0D TMPDocument9 pagestmpA0D TMPFrontiersNo ratings yet
- tmpB1BE TMPDocument9 pagestmpB1BE TMPFrontiersNo ratings yet
- tmp2F3F TMPDocument10 pagestmp2F3F TMPFrontiersNo ratings yet
- tmpC30A TMPDocument10 pagestmpC30A TMPFrontiersNo ratings yet
- tmp3656 TMPDocument14 pagestmp3656 TMPFrontiersNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CrucigramaDocument2 pagesCrucigramaclara soto mendiolaNo ratings yet
- Honeycomb ProblemDocument3 pagesHoneycomb Problemapi-266350282No ratings yet
- Introduction To Information Rertrieval AnswerDocument6 pagesIntroduction To Information Rertrieval AnswerHafidz Jazuli Luthfi100% (4)
- CBT Model for Cognitive StimulationDocument19 pagesCBT Model for Cognitive StimulationAisyah IcahNo ratings yet
- Concordanta Timpurilor Si VB IndirectaDocument4 pagesConcordanta Timpurilor Si VB IndirectaFlo FlorinNo ratings yet
- Answers To How To Master Your Life - Scribd DR LENDocument11 pagesAnswers To How To Master Your Life - Scribd DR LENJackie A Paulson100% (4)
- Inclusive Education Assignment 1Document6 pagesInclusive Education Assignment 1api-297865241100% (1)
- Personality PsychologyDocument101 pagesPersonality PsychologyAnonymous gUjimJKNo ratings yet
- Screening for Memory and Concentration IssuesDocument2 pagesScreening for Memory and Concentration IssuesRhodora SumalinogNo ratings yet
- Creating SimpleOCR ApplicationDocument9 pagesCreating SimpleOCR Applicationabusiddiq1No ratings yet
- Defense Against Adversarial Attacks On Deep Convolutional Neural Networks Through Nonlocal DenoisingDocument8 pagesDefense Against Adversarial Attacks On Deep Convolutional Neural Networks Through Nonlocal DenoisingIAES IJAINo ratings yet
- Shared Book Reading by Parents With Young ChildrenDocument7 pagesShared Book Reading by Parents With Young ChildrenZuriyatini Hj ZainalNo ratings yet
- Lesson Plan in Grade VI-English 6 Adverb of MannerDocument8 pagesLesson Plan in Grade VI-English 6 Adverb of MannerLengie Canacan MontejoNo ratings yet
- Saima Ambreen Psychology 20015 QAU ISDDocument350 pagesSaima Ambreen Psychology 20015 QAU ISDSana SajidNo ratings yet
- Introduction and Review: EspañolDocument14 pagesIntroduction and Review: EspañolAlmyr Jay JimenezNo ratings yet
- Path Fit RefDocument2 pagesPath Fit RefMa. Roycelean PascualNo ratings yet
- 15 - Conceptual Database DesignDocument31 pages15 - Conceptual Database Designshevadanze100% (1)
- Time Management Literature Review-690Document5 pagesTime Management Literature Review-690api-455561998No ratings yet
- Lear Jonathan Aristotelian InfinityDocument25 pagesLear Jonathan Aristotelian Infinityαλεξάνδρα σούσουNo ratings yet
- T1W4Document2 pagesT1W4Lavina KayNo ratings yet
- Catch Up Friday Gr10 Mar1Document3 pagesCatch Up Friday Gr10 Mar1milafer dabanNo ratings yet
- FS 1 - Episode 4Document10 pagesFS 1 - Episode 4Janel MendozaNo ratings yet
- Slide OlogyDocument6 pagesSlide OlogyNagore BelokiNo ratings yet
- Attachment Related PsychodynamicsDocument30 pagesAttachment Related PsychodynamicsMiguel DebonoNo ratings yet
- UNESCO Declaration on Education for Peace, Human Rights and DemocracyDocument14 pagesUNESCO Declaration on Education for Peace, Human Rights and DemocracyYugesh D PANDAYNo ratings yet
- Daily English Lesson Plan for 3rd Grade StudentsDocument36 pagesDaily English Lesson Plan for 3rd Grade StudentsisliNo ratings yet
- Communicating in Costa RicaDocument21 pagesCommunicating in Costa Ricaglanier89No ratings yet
- Deep Learning Ensemble Detects Diabetic Retinopathy StagesDocument10 pagesDeep Learning Ensemble Detects Diabetic Retinopathy StagesMuhammad Junaid AliNo ratings yet
- DCGAN How does it workDocument19 pagesDCGAN How does it workfreedom mutepfeNo ratings yet
- Virtual Reality Use in Architectural Design StudioDocument12 pagesVirtual Reality Use in Architectural Design StudioSarah Abdelaziz Abdelmonem MohamedNo ratings yet