You might also like
- Diverticulitis Cure: The Ultimate Diverticulitis Diet: Diverticulitis Recipes: Your Ultimate Diverticulitis CookbookFrom EverandDiverticulitis Cure: The Ultimate Diverticulitis Diet: Diverticulitis Recipes: Your Ultimate Diverticulitis CookbookNo ratings yet
- Bowel ObstructionDocument8 pagesBowel ObstructionJils SureshNo ratings yet
- What Is Intestinal ObstructionDocument5 pagesWhat Is Intestinal ObstructionmatrixtrinityNo ratings yet
- Mechanical Causes of Intestinal ObstructionDocument5 pagesMechanical Causes of Intestinal ObstructionKimberly Subade MandilagNo ratings yet
- Bowel ObstructionDocument25 pagesBowel Obstructionc0dy143100% (2)
- Bowel Obstruction Vs IleusDocument62 pagesBowel Obstruction Vs IleusSandra SuryariniNo ratings yet
- What Is Intestinal ObstructionDocument7 pagesWhat Is Intestinal ObstructionsagerNo ratings yet
- K26 Ileus ObsDocument18 pagesK26 Ileus ObsmitrajoeNo ratings yet
- Gi DistressDocument3 pagesGi DistressSushil ShindeNo ratings yet
- Case Study or (PGO)Document10 pagesCase Study or (PGO)Nikki Navalta Dela CruzNo ratings yet
- Surgical ConditionsDocument116 pagesSurgical ConditionsFan EliNo ratings yet
- CholecystitisDocument10 pagesCholecystitisCris Pin BumatangNo ratings yet
- Small Bowel Obstruction: Bowel Obstruction (Or Intestinal Obstruction) Is A Mechanical or FunctionalDocument4 pagesSmall Bowel Obstruction: Bowel Obstruction (Or Intestinal Obstruction) Is A Mechanical or FunctionaljazzshaneNo ratings yet
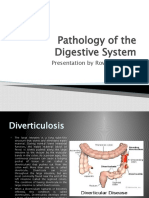
- Pathology of The Digestive System: Presentation by Rowell AngelesDocument25 pagesPathology of The Digestive System: Presentation by Rowell AngelesZEESHAN YOUSUFNo ratings yet
- Intestinal Obstruction, Colorectal CancerDocument49 pagesIntestinal Obstruction, Colorectal CancermeghanaNo ratings yet
- The Diseases of GallbladderDocument27 pagesThe Diseases of GallbladderAroosha IbrahimNo ratings yet
- Intestinal Obstruction: EpidemiologyDocument11 pagesIntestinal Obstruction: EpidemiologyBereket temesgenNo ratings yet
- Paralytic Ileus: Prepared By: Laurence A. Adena, ManDocument43 pagesParalytic Ileus: Prepared By: Laurence A. Adena, ManJanah Beado PagayNo ratings yet
- Small Bowel Obstruction &post Operative IleusDocument62 pagesSmall Bowel Obstruction &post Operative IleusMamanya Fadhil HaniNo ratings yet
- Gastric DisordersDocument135 pagesGastric DisordersEsmareldah Henry SirueNo ratings yet
- Digestive SystemDocument15 pagesDigestive SystemIp Indah PermatasariNo ratings yet
- Gallbladder HydropsDocument6 pagesGallbladder HydropsSaifulAnamNo ratings yet
- Cholecystitis With CholecystolithiasisDocument33 pagesCholecystitis With CholecystolithiasisDino V EscalonaNo ratings yet
- Intestinal Atresia: Presented by Dr. Pankaj YadavDocument39 pagesIntestinal Atresia: Presented by Dr. Pankaj Yadavriri siahaanNo ratings yet
- Small Bowel Obstruction Vs IleusDocument63 pagesSmall Bowel Obstruction Vs IleusKamalesh MurariNo ratings yet
- Intestinal ObstructionDocument9 pagesIntestinal ObstructionHamss AhmedNo ratings yet
- Intestinal Obstruction FinalDocument10 pagesIntestinal Obstruction FinalAmlan jyoti thanapatiNo ratings yet
- TORRE - GI TakeawaysDocument2 pagesTORRE - GI TakeawaysCARLOS JOSETON PAOLO SANTIAGO TORRENo ratings yet
- Understanding The Gallbladder and BileDocument10 pagesUnderstanding The Gallbladder and BileAbirajanNo ratings yet
- Intestinal ObstructionDocument9 pagesIntestinal ObstructionMuhammad Fuad Jaafar100% (1)
- HerniaDocument9 pagesHerniaMohammad Yordan GandaraNo ratings yet
- IntoDocument2 pagesIntoMaryrose Anne BigleteNo ratings yet
- All FilesDocument35 pagesAll FilesHeena AmnaNo ratings yet
- 58.intestinal ObstructionDocument18 pages58.intestinal ObstructionAdenegan Adesola RaymondNo ratings yet
- Anatomy Atresia, Volvulus, Meckel's Diverticulum: BowelDocument45 pagesAnatomy Atresia, Volvulus, Meckel's Diverticulum: BowelkedokterankeluargaNo ratings yet
- Esophageal DiverticulaDocument18 pagesEsophageal DiverticulaAbigail BascoNo ratings yet
- About IntussusceptionDocument6 pagesAbout IntussusceptionErwin OcampoNo ratings yet
- Small Bowel: Alaa MaaliDocument78 pagesSmall Bowel: Alaa MaaliHalima AssiNo ratings yet
- CHOLECYSTITIS With CHOLECYSTOLITHIASISDocument2 pagesCHOLECYSTITIS With CHOLECYSTOLITHIASISkennice_nereaNo ratings yet
- Appendix: What Is The Appendix?Document9 pagesAppendix: What Is The Appendix?Jeenal LakhaniNo ratings yet
- Pancreatitis Ercp Pain Amylase Lipase ErcpDocument24 pagesPancreatitis Ercp Pain Amylase Lipase ErcpPerplexed CeleryNo ratings yet
- What Is The Appendix?: Lymphatic TissueDocument7 pagesWhat Is The Appendix?: Lymphatic TissuecidjjNo ratings yet
- Cholecystitis: What Is It?Document6 pagesCholecystitis: What Is It?Aziil LiizaNo ratings yet
- Esophageal Stricture: DyspepsiaDocument1 pageEsophageal Stricture: DyspepsiaAmiradyta MahartizaNo ratings yet
- Imperforate Anus PDFDocument3 pagesImperforate Anus PDFNajwaNo ratings yet
- IntussusceptionDocument4 pagesIntussusceptionlovethestarNo ratings yet
- Diverticular DiseaseDocument8 pagesDiverticular Diseasenurizzah_885541100% (1)
- Bowel ObstructionDocument46 pagesBowel ObstructionAhmadNurwanto100% (1)
- Intestinal Atresia and StenosisDocument7 pagesIntestinal Atresia and StenosisMichael NafarinNo ratings yet
- Nursing InterventionsDocument3 pagesNursing InterventionsJemiah Lyn C. BragadoNo ratings yet
- Diverticular DiseaseDocument8 pagesDiverticular Diseasenurse_enzo100% (1)
- Inguinal HerniaDocument19 pagesInguinal HerniaAyu W. AnggreniNo ratings yet
- Intestinal ObstructionDocument4 pagesIntestinal ObstructionArchana SahuNo ratings yet
- Bowel Obstruction Case StudyDocument39 pagesBowel Obstruction Case StudyAya Bolinas100% (2)
- Small Bowel Obstruction - Clinical Diagnosis and TreatmentDocument11 pagesSmall Bowel Obstruction - Clinical Diagnosis and TreatmentVigariooNo ratings yet
- Small and Lrge Intestine Pathology SuufiDocument78 pagesSmall and Lrge Intestine Pathology Suufiahmed mahamedNo ratings yet
- IntussusceptionDocument2 pagesIntussusceptionkentkriziaNo ratings yet
- Overview of Gastrointestinal Tract Perforation 2023Document51 pagesOverview of Gastrointestinal Tract Perforation 2023Ricardo Javier Arreola PeraltaNo ratings yet
- Intestinal Obstruction PDFDocument4 pagesIntestinal Obstruction PDFKiiza AloysiusNo ratings yet
- Ileus: Symptoms Causes Risk Factors Diagnosis Complications Treatments Outlook PreventionDocument13 pagesIleus: Symptoms Causes Risk Factors Diagnosis Complications Treatments Outlook PreventionNurul AmaliyahNo ratings yet
- Critical ThinkingDocument6 pagesCritical ThinkingmatrixtrinityNo ratings yet
- Stress and Illness: Castillo, Justine GDocument19 pagesStress and Illness: Castillo, Justine GmatrixtrinityNo ratings yet
- Distinguishing Features of Anthropology - Characteristics 1-5 6.78 What Are The3 Unique Approaches of AnthropologyDocument2 pagesDistinguishing Features of Anthropology - Characteristics 1-5 6.78 What Are The3 Unique Approaches of AnthropologymatrixtrinityNo ratings yet
- Intelligence in PsychologyDocument29 pagesIntelligence in PsychologymatrixtrinityNo ratings yet
- Group Number: Case Title: Year and Section: Group Members: 1. 5. 2. 6. 3. 7. 4. 8Document1 pageGroup Number: Case Title: Year and Section: Group Members: 1. 5. 2. 6. 3. 7. 4. 8matrixtrinityNo ratings yet
- antepartumTEST1 MOSBYDocument14 pagesantepartumTEST1 MOSBYmatrixtrinity50% (2)
- Antepartumtest2 LippincottDocument7 pagesAntepartumtest2 Lippincottmatrixtrinity100% (1)
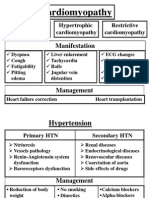
- Cardio DiseasesDocument17 pagesCardio DiseasesmatrixtrinityNo ratings yet
- Intestinal Obstruction5Document4 pagesIntestinal Obstruction5matrixtrinityNo ratings yet
- Burns and Environmental EmergenciesDocument33 pagesBurns and Environmental EmergenciesmatrixtrinityNo ratings yet
- Socio - GENDER, ETHNICITY AND RACEDocument22 pagesSocio - GENDER, ETHNICITY AND RACEmatrixtrinity100% (1)
- Blood ComponentDocument33 pagesBlood Componentmatrixtrinity100% (1)
- Cardiovascular Physio Logic ProcessDocument35 pagesCardiovascular Physio Logic ProcessmatrixtrinityNo ratings yet
- Cerebrovascular Accidents: Rochee P. Benito, RNDocument23 pagesCerebrovascular Accidents: Rochee P. Benito, RNmatrixtrinityNo ratings yet
- Cardiovascular Therapeutic ManagementDocument15 pagesCardiovascular Therapeutic ManagementmatrixtrinityNo ratings yet
- Circulatory System: Rochi Paraon Benito, RN Infection Control NurseDocument15 pagesCirculatory System: Rochi Paraon Benito, RN Infection Control NursematrixtrinityNo ratings yet
- Cardiomyopathy 02Document2 pagesCardiomyopathy 02matrixtrinityNo ratings yet
- Acute Intestinal ObstructionDocument38 pagesAcute Intestinal ObstructionAnonymous O4fTKXvILNo ratings yet
- Group 5 Case 4aDocument83 pagesGroup 5 Case 4aVenny VeronicaNo ratings yet
- Recognizing Bowel Obstruction and IleusDocument35 pagesRecognizing Bowel Obstruction and IleusmustikaNo ratings yet
- Hernia Complications: When To Seek Immediate Medical Attention - Dr. Samrat JankarDocument2 pagesHernia Complications: When To Seek Immediate Medical Attention - Dr. Samrat JankarDr. Samrat JankarNo ratings yet
- Hypertrophic Pyloric StenosisDocument28 pagesHypertrophic Pyloric StenosisAhmad Abu Kush100% (2)
- Intestinal ObstructionDocument59 pagesIntestinal ObstructionGeorge GuruNo ratings yet
- Bowel Obstruction - ppt1Document30 pagesBowel Obstruction - ppt1Elfrida Aulia100% (1)
- Ebook Comprehensive Radiographic Pathology 6Th Edition Eisenberg Test Bank Full Chapter PDFDocument46 pagesEbook Comprehensive Radiographic Pathology 6Th Edition Eisenberg Test Bank Full Chapter PDFsinapateprear4k100% (11)
- Mcqs IV Year Students SurgeryDocument38 pagesMcqs IV Year Students SurgeryAbdimajiidNo ratings yet
- Study Guide For Med Surg 1Document15 pagesStudy Guide For Med Surg 1desireemaenugentNo ratings yet
- Acute AbdomenDocument125 pagesAcute Abdomenvinitha kattaNo ratings yet
- 12 - Paediatric Abdomen RadiologyDocument74 pages12 - Paediatric Abdomen RadiologyMaria DoukaNo ratings yet
- Atresia of Jejunum and IleumDocument5 pagesAtresia of Jejunum and IleumTiffany AdelinaNo ratings yet
- Calvo Fetal GITractDocument154 pagesCalvo Fetal GITractRaluca HabaNo ratings yet
- PVNR Telangana Veterinary University: Veterinary Surgery and Radiology Credit Hours:2+1Document8 pagesPVNR Telangana Veterinary University: Veterinary Surgery and Radiology Credit Hours:2+1Naveen BasudeNo ratings yet
- SURGERY 2018-2008 Regular+Supplementary Chapter Wise Question Papers WBUHSDocument16 pagesSURGERY 2018-2008 Regular+Supplementary Chapter Wise Question Papers WBUHSBcBaba 007100% (1)
- Medical Terminology Express A Short Course Approach by Body System 2nd Edition Gylys Test BankDocument13 pagesMedical Terminology Express A Short Course Approach by Body System 2nd Edition Gylys Test Banksinapateprear4k100% (23)
- Surgery MCQDocument24 pagesSurgery MCQMoiz Khan88% (8)
- Paralytic Ileus: Prepared By: Laurence A. Adena, ManDocument43 pagesParalytic Ileus: Prepared By: Laurence A. Adena, ManJanah Beado PagayNo ratings yet
- 2.large Bowel ObstructionDocument13 pages2.large Bowel Obstructionurmila prajapatiNo ratings yet
- EMQs For Medical Students Volume 2 2eDocument30 pagesEMQs For Medical Students Volume 2 2ePasTestBooks50% (2)
- Gastric Dilation and Volvulus Syndrome in DogDocument4 pagesGastric Dilation and Volvulus Syndrome in DogPutu SuandhikaNo ratings yet
- Cases Elog BookDocument13 pagesCases Elog BookFaryal UfaqNo ratings yet
- డా.వై.యస్ ఆర్. ఆరోగ్య శ్రీ వ్యాదుల వివరాలు PDFDocument222 pagesడా.వై.యస్ ఆర్. ఆరోగ్య శ్రీ వ్యాదుల వివరాలు PDFThrinadh KosuriNo ratings yet
- Thesis Topics of MS General SurgeryDocument20 pagesThesis Topics of MS General SurgeryNaveed Khan75% (12)
- تجميعات مزاولة و بورد و توظيف تحديث 8-2016Document86 pagesتجميعات مزاولة و بورد و توظيف تحديث 8-2016Mahitab M. Alkhoudary80% (5)
- Surgical Complications: Maj. Hafizur Rashid SazalDocument43 pagesSurgical Complications: Maj. Hafizur Rashid SazalHafizur RashidNo ratings yet
- 2 Intestinal Obstruction. IntussusceptionDocument28 pages2 Intestinal Obstruction. IntussusceptionGede SubhagaNo ratings yet
- 990617 EUS教學 (12) 急診超音波在兒科急症之應用Document67 pages990617 EUS教學 (12) 急診超音波在兒科急症之應用juice119100% (1)
- Management of Intestinal ObstructionDocument33 pagesManagement of Intestinal ObstructionSya Samat100% (1)