You might also like
- F E T C: Luid AND Lectrolyte Herapy IN HildrenDocument12 pagesF E T C: Luid AND Lectrolyte Herapy IN HildrenHartantoRezaGazaliNo ratings yet
- FLUID AND ELECTROLYTE THERAPY IN CHILDRENDocument12 pagesFLUID AND ELECTROLYTE THERAPY IN CHILDRENTania Febria AzizahNo ratings yet
- Fluid Management - Presentation PDFDocument16 pagesFluid Management - Presentation PDFjuniorebinda100% (1)
- Maintenance Intravenous Fluid Therapy in Children - UpToDateDocument19 pagesMaintenance Intravenous Fluid Therapy in Children - UpToDaterolland_arrizaNo ratings yet
- Pediatric FluidsDocument8 pagesPediatric FluidsprashsubbuNo ratings yet
- Author: Section Editor: Deputy EditorDocument11 pagesAuthor: Section Editor: Deputy EditorVictor Lima AraujoNo ratings yet
- Fluid Management For The Pediatric Surgical Patient POWERPOINTDocument34 pagesFluid Management For The Pediatric Surgical Patient POWERPOINTDipta Anggara100% (2)
- Fluids and Electrolytes - PaediatricsDocument52 pagesFluids and Electrolytes - PaediatricsZweNo ratings yet
- PEDIATRIC FLUIDSDocument42 pagesPEDIATRIC FLUIDSSholehuddin MunajjidNo ratings yet
- Fluid and Electrolytes.3Document43 pagesFluid and Electrolytes.3Medic PediatruNo ratings yet
- Test Bank For Lutzs Nutrition and Diet Therapy 7th by MazurDocument15 pagesTest Bank For Lutzs Nutrition and Diet Therapy 7th by Mazurtracywilsonjftmrqknys100% (27)
- Test Bank Lutzs Nutrition and Diet Therapy 7th Edition Erin e MazurDocument16 pagesTest Bank Lutzs Nutrition and Diet Therapy 7th Edition Erin e Mazurjeremiahhartfozxmbqayn100% (10)
- Fluid TherapyDocument27 pagesFluid TherapyRashed ShatnawiNo ratings yet
- Principles+ +LU6Document35 pagesPrinciples+ +LU6Alvin Ray JuanNo ratings yet
- Improving Management of Diabetic Ketoacidosis in Children: 2001 108 735-740 Eric I. Felner and Perrin C. WhiteDocument8 pagesImproving Management of Diabetic Ketoacidosis in Children: 2001 108 735-740 Eric I. Felner and Perrin C. Whiterien2903No ratings yet
- Perioperative Fluid Management in ChildrenDocument31 pagesPerioperative Fluid Management in ChildrenRashmi SahaNo ratings yet
- Maintenance Fluid Therapy in ChildrenDocument4 pagesMaintenance Fluid Therapy in ChildrenNicole_0No ratings yet
- Fluid and Electrolytes JoyDocument10 pagesFluid and Electrolytes JoyM Rizal IsburhanNo ratings yet
- Fluid & ElectrolyteDocument68 pagesFluid & ElectrolytePranay MallNo ratings yet
- Fluidos y ElectrolitosDocument8 pagesFluidos y ElectrolitosJavierNo ratings yet
- Liquidos PediatriaDocument9 pagesLiquidos PediatriaAndrea RangelNo ratings yet
- Terapi Cairan: Pembimbing: Dr. Dr. Bobby Setiadi Dharmawan, SpaDocument45 pagesTerapi Cairan: Pembimbing: Dr. Dr. Bobby Setiadi Dharmawan, SpaAdamilzaryFikryNo ratings yet
- Fluid and Electrolyte BalanceDocument11 pagesFluid and Electrolyte BalanceSalman AshrafNo ratings yet
- Hipotonicos VS IsotonicosDocument13 pagesHipotonicos VS IsotonicosYeison Duban Gomez CastilloNo ratings yet
- Pedia Alhamdollilah FluidsDocument80 pagesPedia Alhamdollilah FluidsArwyn AncogNo ratings yet
- IndianJAnaesth565454-4188731 113807Document9 pagesIndianJAnaesth565454-4188731 113807T RonaskyNo ratings yet
- IndianJAnaesth565454-1388002 035120Document9 pagesIndianJAnaesth565454-1388002 035120T RonaskyNo ratings yet
- Fluid and Electrolyte ConceptDocument40 pagesFluid and Electrolyte ConceptBarnis Lady Mentari AlamdaniNo ratings yet
- Fluids and Electrolyte PediatricsDocument41 pagesFluids and Electrolyte PediatricsYusron BishryNo ratings yet
- Paed BTDocument9 pagesPaed BTparuNo ratings yet
- Enteral and Parental Nutrititon Case StudyDocument7 pagesEnteral and Parental Nutrititon Case Studyjikute.911No ratings yet
- Perioperative Fluid ManagementDocument123 pagesPerioperative Fluid ManagementAnonymous 86gki5No ratings yet
- 240 - TTC #3Document3 pages240 - TTC #3vercia8877No ratings yet
- Manajemen Perioperatif Terapi Cairan Pada PediatriDocument35 pagesManajemen Perioperatif Terapi Cairan Pada PediatriZulhendraNo ratings yet
- Fluid & Ele. MGTDocument36 pagesFluid & Ele. MGTMerwan KemalNo ratings yet
- Fluids and Electrolytes For PediatricsDocument31 pagesFluids and Electrolytes For PediatricsJeno Luis J. ACUBNo ratings yet
- Dehydration: Body-Fluid CompositionDocument5 pagesDehydration: Body-Fluid CompositionThegreat Mokz Mokz ThegreatNo ratings yet
- Table: I. Composition of The Mg. Sodium Diei - . - .Document25 pagesTable: I. Composition of The Mg. Sodium Diei - . - .Henry Bagus WicaksonoNo ratings yet
- Fluid Therapy in Paediatrics - RevisedDocument5 pagesFluid Therapy in Paediatrics - RevisedJehangir AllamNo ratings yet
- Case Study-Infant With Fluid Imbalance08-10-KEYDocument3 pagesCase Study-Infant With Fluid Imbalance08-10-KEYreecoleNo ratings yet
- Fluid Electrolytes Bablance 150308Document16 pagesFluid Electrolytes Bablance 150308Shruthi RathishNo ratings yet
- 1 FluidsDocument17 pages1 FluidsMae CalunsagNo ratings yet
- 4.fluid and ElectrolytesDocument23 pages4.fluid and ElectrolytesManju KumariNo ratings yet
- Intravenous Fluid Therapy: Michael OrnesDocument27 pagesIntravenous Fluid Therapy: Michael OrnesOkto Mara Fandi HarahapNo ratings yet
- What Is Plasma Osmolality?:, 23 Mei 2007 Fluid and Electrolyte TherapyDocument17 pagesWhat Is Plasma Osmolality?:, 23 Mei 2007 Fluid and Electrolyte TherapyRani ChesarNo ratings yet
- Maternal Child NursingDocument24 pagesMaternal Child NursingRodneyDanielsdnip100% (32)
- Fluids, electrolytes and acid-base balanceDocument13 pagesFluids, electrolytes and acid-base balanceMansoor TariqNo ratings yet
- Fluid & Electrolyte Management in Neonates: Critical Aspect of Care of High Risk InfantsDocument78 pagesFluid & Electrolyte Management in Neonates: Critical Aspect of Care of High Risk Infantsdrhemantparakh100% (1)
- Care Plan FVDDocument5 pagesCare Plan FVDapi-283213958No ratings yet
- Fluids and Electrolytes in Pediatrics FinalDocument41 pagesFluids and Electrolytes in Pediatrics FinalArun GeorgeNo ratings yet
- Leukemia Case StudyDocument32 pagesLeukemia Case Studydsaitta108No ratings yet
- Fluid Calculation For Iv InfusionDocument8 pagesFluid Calculation For Iv InfusionAsma SaleemNo ratings yet
- FLUID MANAGEMENT IN MALNUTRITIONDocument30 pagesFLUID MANAGEMENT IN MALNUTRITIONCHALIE MEQUNo ratings yet
- Basics of Fluid and Transfusion Therapy in PediatricDocument9 pagesBasics of Fluid and Transfusion Therapy in Pediatric'sally' RosaLie EllyNo ratings yet
- Metabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentFrom EverandMetabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentCarole IchaiNo ratings yet
- Acid-Base and Electrolyte Handbook for Veterinary TechniciansFrom EverandAcid-Base and Electrolyte Handbook for Veterinary TechniciansAngela Randels-ThorpNo ratings yet
- Basic Monitoring in Canine and Feline Emergency PatientsFrom EverandBasic Monitoring in Canine and Feline Emergency PatientsElizabeth J ThomovskyRating: 1 out of 5 stars1/5 (1)
- Fluid and Electrolytes in Pediatrics: A Comprehensive HandbookFrom EverandFluid and Electrolytes in Pediatrics: A Comprehensive HandbookNo ratings yet
- Equine Fluid TherapyFrom EverandEquine Fluid TherapyC. Langdon FieldingNo ratings yet
- The Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?From EverandThe Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?No ratings yet
- Full Nice EpilepsyDocument152 pagesFull Nice EpilepsywalidNo ratings yet
- 100 ECG For AKP - With AnswersDocument102 pages100 ECG For AKP - With AnswersaeyousefNo ratings yet
- Basic Medical Sciences (3rd Ed)Document442 pagesBasic Medical Sciences (3rd Ed)aeyousefNo ratings yet
- Common Respiratory VideosDocument25 pagesCommon Respiratory VideosaeyousefNo ratings yet
- Neurological Conditions Revison Table1Document8 pagesNeurological Conditions Revison Table1aeyousefNo ratings yet
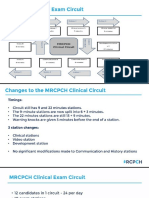
- MRCPH Clinical Exam Changes From September 2019Document42 pagesMRCPH Clinical Exam Changes From September 2019aeyousefNo ratings yet
- Developmental Assessment in One PageDocument1 pageDevelopmental Assessment in One PageTONY GO AWAYNo ratings yet
- NRPDocument8 pagesNRPaeyousefNo ratings yet
- Nervous System Exam Guide for ChildrenDocument4 pagesNervous System Exam Guide for ChildrenaeyousefNo ratings yet
- Dka GuidelineDocument16 pagesDka GuidelineGhada HusseinNo ratings yet
- The Big Six Clinical GuidelineDocument41 pagesThe Big Six Clinical GuidelineaeyousefNo ratings yet
- Clinical Cases Mrcpch1Document223 pagesClinical Cases Mrcpch1aeyousef100% (1)
- Causes of Obesity in ChildrenDocument2 pagesCauses of Obesity in ChildrenaeyousefNo ratings yet
- DERMA TAS Pastest Derma Part 1bDocument128 pagesDERMA TAS Pastest Derma Part 1baeyousefNo ratings yet
- Clinical Cases For MRCPCH PART 2 Applied Knowledge in PracticeDocument218 pagesClinical Cases For MRCPCH PART 2 Applied Knowledge in Practiceaeyousef88% (16)
- 10th MSS CPC Clinical AbstractDocument4 pages10th MSS CPC Clinical Abstractregadel07No ratings yet
- CVP Insertion Close Tube Thoracostomy RDocument6 pagesCVP Insertion Close Tube Thoracostomy RFaye Nadine T. CABURALNo ratings yet
- Effects of Social Media On The Psychology of PeopleDocument6 pagesEffects of Social Media On The Psychology of PeopleIJAFRCNo ratings yet
- Skenario 2 Saraf & PerilakuDocument30 pagesSkenario 2 Saraf & PerilakuPrima Eriawan PutraNo ratings yet
- 8 Curious Meridians Exercises for LongevityDocument6 pages8 Curious Meridians Exercises for Longevitypeter911x100% (2)
- BTL Ultrasound 5000 - User ManualDocument16 pagesBTL Ultrasound 5000 - User ManualAlexaNo ratings yet
- Prokaryotic Cells: Eukaryotes Vs Prokaryotes: What's The Difference?Document8 pagesProkaryotic Cells: Eukaryotes Vs Prokaryotes: What's The Difference?Anggun Teh PamegetNo ratings yet
- HBCJ Npev Vedw T60B PDFDocument20 pagesHBCJ Npev Vedw T60B PDFAnonymous fPQaCe8No ratings yet
- Neurology Crossword Puzzle Answer KeyDocument1 pageNeurology Crossword Puzzle Answer KeyRavinaAhujaNo ratings yet
- Skeletal System PowerpointDocument40 pagesSkeletal System PowerpointLee KaiYangNo ratings yet
- LP UapDocument18 pagesLP UapHat MutisalNo ratings yet
- University of Phoenix Anatomy and Physiology Week 2 QuizDocument2 pagesUniversity of Phoenix Anatomy and Physiology Week 2 QuizSophia FHSNo ratings yet
- Receptors IntroductionDocument53 pagesReceptors IntroductionSunilNo ratings yet
- Alzheimer's Disease and Memory Drugs PDFDocument97 pagesAlzheimer's Disease and Memory Drugs PDFbradbaderNo ratings yet
- Evaluation of Preoperative Pulmonary RiskDocument19 pagesEvaluation of Preoperative Pulmonary RiskCharlieBrown_QBNo ratings yet
- 0610 - 2016 - 41 Paper 4Document20 pages0610 - 2016 - 41 Paper 4Muhammad HassaanNo ratings yet
- Host defense mechanisms overviewDocument7 pagesHost defense mechanisms overviewmyfilesNo ratings yet
- The Integumentary System: Layers and Functions of SkinDocument8 pagesThe Integumentary System: Layers and Functions of SkinAmanuel MaruNo ratings yet
- DFT Brochure FitnessDocument2 pagesDFT Brochure Fitnessmrtickle91No ratings yet
- The Urinary System: Prepared by Patty Bostwick-Taylor, Florence-Darlington Technical CollegeDocument91 pagesThe Urinary System: Prepared by Patty Bostwick-Taylor, Florence-Darlington Technical CollegeNicole NipasNo ratings yet
- Ch.12 Getting the measure of hormones講義Document7 pagesCh.12 Getting the measure of hormones講義邱小瀧No ratings yet
- แนวข้อสอบ National license - Hematology PDFDocument7 pagesแนวข้อสอบ National license - Hematology PDFTanawat SingboonNo ratings yet
- Histological Characteristics of the Lingual FrenulumDocument1 pageHistological Characteristics of the Lingual FrenulumajudNo ratings yet
- 12 White Blood Cell Counting Techniques in BirdsDocument5 pages12 White Blood Cell Counting Techniques in BirdsPablo LópezNo ratings yet
- PsychSim 5 Quizzing - Chapter 6-Sensation and PerceptionDocument5 pagesPsychSim 5 Quizzing - Chapter 6-Sensation and Perceptionneecee126100% (1)
- Cerebral EdemaDocument5 pagesCerebral EdemaAdilah AdeebNo ratings yet
- Cell Biology Test - 70 Possible Points: Prokaryotic and Eukaryotic Cells (2 Points Per Question)Document3 pagesCell Biology Test - 70 Possible Points: Prokaryotic and Eukaryotic Cells (2 Points Per Question)Vienne MonroidNo ratings yet
- Ent Diseases of The Oral and Pharynx Dr. UyDocument7 pagesEnt Diseases of The Oral and Pharynx Dr. UyAileen EmyNo ratings yet
- MedulloblastomaDocument2 pagesMedulloblastomaMohammadAwitNo ratings yet
- Physiology Previous Year PDFDocument129 pagesPhysiology Previous Year PDFmina mounirNo ratings yet