You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Chamberlain S Symptoms and Signs in Clinical Medicine 13th Medibos Blogspot Com (1) PDFDocument504 pagesChamberlain S Symptoms and Signs in Clinical Medicine 13th Medibos Blogspot Com (1) PDFSwarnadeep ManiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Step On To Paediatrics 4th EditionDocument376 pagesStep On To Paediatrics 4th EditionTawhid Zihad100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- ECMO-Extracorporeal+Life+Support+in+Adul (Estudio)Document475 pagesECMO-Extracorporeal+Life+Support+in+Adul (Estudio)Christian Espinoza Silva100% (1)
- KyphiDocument4 pagesKyphiPhlegisNo ratings yet
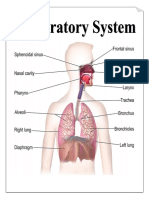
- Parts & Function of Respiratory SystemDocument4 pagesParts & Function of Respiratory SystemLucille Ballares83% (6)
- Blood Gas HandbookDocument112 pagesBlood Gas HandbookNuno Silva100% (1)
- Rheumatic FeverDocument81 pagesRheumatic FeverMobin Ur Rehman KhanNo ratings yet
- Resume For WebsiteDocument2 pagesResume For Websiteapi-350983586No ratings yet
- Acute Appendicitis UltrasonographyDocument5 pagesAcute Appendicitis Ultrasonographyharrinson89No ratings yet
- Approach To The Diagnosis of Congenital Myopathies PIIS0960896613009942Document20 pagesApproach To The Diagnosis of Congenital Myopathies PIIS0960896613009942ElcklymNo ratings yet
- MEDISEP Hospital ListDocument3 pagesMEDISEP Hospital ListQ8123No ratings yet
- Student Guide: SourceDocument82 pagesStudent Guide: Sourcewaraney palitNo ratings yet
- Rare Rheumatic Diseases: Springer Books Available As Printed BookDocument1 pageRare Rheumatic Diseases: Springer Books Available As Printed BookYUSHANo ratings yet
- U.S. Army Medical Service Corps Fact SheetDocument6 pagesU.S. Army Medical Service Corps Fact SheetU.S. Army Medical Department (AMEDD)No ratings yet
- Topics On Prosthetics & Orthotics - PDF CreDocument4 pagesTopics On Prosthetics & Orthotics - PDF CreSuprit MahakudNo ratings yet
- Class IV KhodaryDocument7 pagesClass IV KhodaryelshihaweyNo ratings yet
- Teeth in A Day Nys deDocument4 pagesTeeth in A Day Nys deSatyendra KumarNo ratings yet
- Use of Umbrella Graft For Nasal Tip ProjectionDocument4 pagesUse of Umbrella Graft For Nasal Tip ProjectionbsBanNo ratings yet
- PhimosisDocument4 pagesPhimosisHelvia Septarini TanjungNo ratings yet
- Knee Injury and Osteoarthritis Outcome Score Koos: A User's Guide ToDocument9 pagesKnee Injury and Osteoarthritis Outcome Score Koos: A User's Guide ToQina Nugroho, pts.No ratings yet
- SBP PNP Analysis PDFDocument3 pagesSBP PNP Analysis PDFAlexavier DylanNo ratings yet
- 3 PDFDocument9 pages3 PDFrahmawati aliwarmanNo ratings yet
- Hospital Pharmacist PDFDocument5 pagesHospital Pharmacist PDFMuhammad YamnainNo ratings yet
- Plan of Care For: .: Ineffective Health ManagementDocument5 pagesPlan of Care For: .: Ineffective Health Managementapi-544185261No ratings yet
- Article Balanced ScorecardDocument2 pagesArticle Balanced ScorecardJi YuNo ratings yet
- Size Matters A Review of The Effect of Pellet Size On Animal Behaviour and DigestionDocument6 pagesSize Matters A Review of The Effect of Pellet Size On Animal Behaviour and DigestionHerald Scholarly Open AccessNo ratings yet
- Court RecordsDocument11 pagesCourt RecordsFircrest CrusaderNo ratings yet
- This Month in Pediatric UrologyDocument2 pagesThis Month in Pediatric UrologyAswad AffandiNo ratings yet
- Factors Influencing Permanent Teeth Eruption. Part One - General FactorsDocument6 pagesFactors Influencing Permanent Teeth Eruption. Part One - General FactorsestherNo ratings yet
- Globus PharyngusDocument10 pagesGlobus PharyngusamalNo ratings yet