You might also like
- QuickStudy - Lymphatic SystemDocument2 pagesQuickStudy - Lymphatic SystemEmina Borovac100% (2)
- Astringent Herbs Stambhana KarmaDocument4 pagesAstringent Herbs Stambhana Karmaqueencel100% (1)
- Complications of FracturesDocument13 pagesComplications of FracturesmilananandNo ratings yet
- Acute compartment syndrome after blood gas analysis in patient thrombolyzed for PEDocument4 pagesAcute compartment syndrome after blood gas analysis in patient thrombolyzed for PEsalamsibiuNo ratings yet
- HOMEOSTASIS - Lecture (Human Biology)Document22 pagesHOMEOSTASIS - Lecture (Human Biology)dokteraanNo ratings yet
- Superficial Parotidectomy TRZDocument20 pagesSuperficial Parotidectomy TRZdokteraan100% (3)
- Acute Compartment SyndromeDocument15 pagesAcute Compartment SyndromeDea Sella SabrinaNo ratings yet
- Argument Essay - Measles VaccinationsDocument12 pagesArgument Essay - Measles VaccinationsTom BeaulieuNo ratings yet
- Glomus TumourDocument50 pagesGlomus TumourPratibha Goswami100% (1)
- Martin Zenker-Noonan Syndrome and Related Disorders - A Matter of Deregulated Ras Signaling (Monographs in Human Genetics Vol 17) - S. Karger AG (Switzerland) (2009)Document178 pagesMartin Zenker-Noonan Syndrome and Related Disorders - A Matter of Deregulated Ras Signaling (Monographs in Human Genetics Vol 17) - S. Karger AG (Switzerland) (2009)Lupu AndreeaNo ratings yet
- Compartment Syndrome: Return To TopDocument3 pagesCompartment Syndrome: Return To TopSania Kamal BalweelNo ratings yet
- Acute Limb Ischemia SiteDocument23 pagesAcute Limb Ischemia Sitedokteraan100% (2)
- Compartment SyndromeDocument36 pagesCompartment SyndromeHaziq MarsNo ratings yet
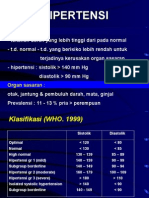
- HipertensiDocument28 pagesHipertensidokteraanNo ratings yet
- Compartemen Syndrome: Nur Asiah MustariDocument16 pagesCompartemen Syndrome: Nur Asiah MustariirsanNo ratings yet
- Anticipatory GuidanceDocument26 pagesAnticipatory GuidanceSanti Sri HartiniNo ratings yet
- Equine Abdominal Surgery ProceduresDocument76 pagesEquine Abdominal Surgery ProceduresasheneyNo ratings yet
- CV-Prof-MulyadiDocument69 pagesCV-Prof-MulyadityesNo ratings yet
- Abdomen Test QuestionsDocument20 pagesAbdomen Test QuestionsRuth AlooNo ratings yet
- Communicable Disease NursingDocument41 pagesCommunicable Disease NursingBJ DUQUESA100% (2)
- Kompartemen SindromDocument9 pagesKompartemen SindromPutri PratiwiNo ratings yet
- Compartment SyndromeDocument4 pagesCompartment SyndromePravina PospanathanNo ratings yet
- Compartment SyndromeDocument13 pagesCompartment SyndromebismahNo ratings yet
- Bayi Baru Lahir: UPTD Pukesmas Tampa Marlina Susana, S.Kep,.MM NIP. 18731013 199203 2 002Document3 pagesBayi Baru Lahir: UPTD Pukesmas Tampa Marlina Susana, S.Kep,.MM NIP. 18731013 199203 2 002sherly veronicaNo ratings yet
- Background: ParotitisDocument23 pagesBackground: ParotitisifahInayah100% (1)
- Symptoms and Signs: Compartment SyndromeDocument4 pagesSymptoms and Signs: Compartment SyndromeajeikoNo ratings yet
- Acute Compartment Syndrome - StatPearls - NCBI BookshelfDocument9 pagesAcute Compartment Syndrome - StatPearls - NCBI BookshelfSahra FadillahNo ratings yet
- Fasciotomy Procedure OverviewDocument16 pagesFasciotomy Procedure OverviewNatalia Ossa RodríguezNo ratings yet
- Volkmann Contracture: Historical AspectsDocument2 pagesVolkmann Contracture: Historical AspectsMohammadAwitNo ratings yet
- Compartment SyndromeDocument67 pagesCompartment SyndromeashokNo ratings yet
- Compartment SynDocument51 pagesCompartment SynFIYINFOLUWA ESTHER AYODELENo ratings yet
- CS-Abdominal and Extremity Compartment SyndromeDocument17 pagesCS-Abdominal and Extremity Compartment SyndromeBudiono Gunawan SutantoNo ratings yet
- Compartment Syndrome Is The Compression of NervesDocument2 pagesCompartment Syndrome Is The Compression of NervesHelen Ann John RomelNo ratings yet
- Complications of Extremeitiy TraumaDocument11 pagesComplications of Extremeitiy TraumaGilang Kurnia HirawatiNo ratings yet
- Compartment Syndrome: - DiscussionDocument11 pagesCompartment Syndrome: - DiscussionatrisniaNo ratings yet
- Compartment Syndrome Diagnosis and TreatmentDocument3 pagesCompartment Syndrome Diagnosis and TreatmentTantyo Adi P100% (2)
- Litrev Trauma MuskuloskeletalDocument26 pagesLitrev Trauma Muskuloskeletaldedyalkarni08No ratings yet
- Articulo AnaDocument5 pagesArticulo AnaPaulina Marquez RojasNo ratings yet
- complicationsoffractures-120127084025-phpapp02-convertedDocument62 pagescomplicationsoffractures-120127084025-phpapp02-convertedAaliyah ShaikhNo ratings yet
- Compartmental Syndromes: Understanding and Treating Pressure-Induced Circulatory CompromiseDocument72 pagesCompartmental Syndromes: Understanding and Treating Pressure-Induced Circulatory CompromiseDaniel PaterninaNo ratings yet
- C S: O E: Ompartment Yndrome AN Rthopedic MergencyDocument5 pagesC S: O E: Ompartment Yndrome AN Rthopedic MergencyAndreew SoscueNo ratings yet
- COMPARTMENT SYNDROMEv finalDocument56 pagesCOMPARTMENT SYNDROMEv finalbhavikaagarwal07No ratings yet
- Causes, Symptoms and Treatment of Compartment SyndromeDocument4 pagesCauses, Symptoms and Treatment of Compartment SyndromeAngie LimNo ratings yet
- Chronic Critical Limb Ischemia Diagnosis, Treatment and PrognosisDocument14 pagesChronic Critical Limb Ischemia Diagnosis, Treatment and PrognosisHelena A. K. CantikaNo ratings yet
- Acute Limb Ischemia: Clinical PracticeDocument9 pagesAcute Limb Ischemia: Clinical PracticeIndah MaulidawatiNo ratings yet
- Acute Limb Ischemia: Clinical PracticeDocument9 pagesAcute Limb Ischemia: Clinical PracticeKezia TambunanNo ratings yet
- Fascio To MyDocument9 pagesFascio To MydwiNo ratings yet
- Compartment Syndrome AndreDocument40 pagesCompartment Syndrome AndreOlivia Christy KaihatuNo ratings yet
- Musculoskeletal TraumaDocument19 pagesMusculoskeletal Traumamunazzarehman37No ratings yet
- Challenge 2010 Lecture Notes: PathophysiologyDocument14 pagesChallenge 2010 Lecture Notes: PathophysiologyPrince AhmedNo ratings yet
- Pathophysiology Worksheet MIDocument2 pagesPathophysiology Worksheet MIpjbedelNo ratings yet
- Complications of Multiple FracturesDocument35 pagesComplications of Multiple Fractureshello from the other sideNo ratings yet
- Complications of Fractures and ManagementDocument65 pagesComplications of Fractures and ManagementSemestaNo ratings yet
- Compartment SyndromeDocument2 pagesCompartment Syndromeanis perdana ansyariNo ratings yet
- Pathophysiology For Surgery FinalDocument270 pagesPathophysiology For Surgery FinalWaqas HaleemNo ratings yet
- Anatomy: Compartment SyndromeDocument4 pagesAnatomy: Compartment SyndromeRahAlitNo ratings yet
- Compartment Syndrome Diagnosis and TreatmentDocument14 pagesCompartment Syndrome Diagnosis and Treatmentfatimah putriNo ratings yet
- Toorthj 8 185Document10 pagesToorthj 8 185fatimah putriNo ratings yet
- Sd. Compartimental y AR A CL 2022Document19 pagesSd. Compartimental y AR A CL 2022Alejandra SanchezNo ratings yet
- Laporan PBL Modul Vaskular Blok KardiovaskularDocument38 pagesLaporan PBL Modul Vaskular Blok KardiovaskularMuhammad FakhriNo ratings yet
- Compartment Syndrome Diagnosis and TreatmentDocument38 pagesCompartment Syndrome Diagnosis and Treatmentloya4everNo ratings yet
- CrushDocument12 pagesCrushJamila AragonNo ratings yet
- Acute Limb IschemiaDocument21 pagesAcute Limb IschemiajuanpbagurNo ratings yet
- Vascular trauma principles and managementDocument36 pagesVascular trauma principles and managementGordana UzelacNo ratings yet
- Fat Embolism and Compartment SyndromeDocument19 pagesFat Embolism and Compartment SyndromeAbdulsalam DostNo ratings yet
- Venous Thoracic Outlet SyndromeDocument9 pagesVenous Thoracic Outlet SyndromeAkhmad HidayatNo ratings yet
- Acute Compartment Syndrome: A Literature Review and UpdatesDocument5 pagesAcute Compartment Syndrome: A Literature Review and UpdatesasclepiuspdfsNo ratings yet
- Fracture ManagementDocument17 pagesFracture ManagementMazvita Maz MatipiraNo ratings yet
- Kelompok 15 Skenario 3Document42 pagesKelompok 15 Skenario 313calcitoninNo ratings yet
- Dr.E.Kaizar EnnisDocument29 pagesDr.E.Kaizar EnnisKaizar EnnisNo ratings yet
- Acute Compartment Syndrome of The Extremities - UpToDateDocument29 pagesAcute Compartment Syndrome of The Extremities - UpToDateluisaNo ratings yet
- Crush InjuryDocument8 pagesCrush Injuryfadhil03No ratings yet
- Aula de ChoqueDocument16 pagesAula de Choqueapi-3726545100% (1)
- TRIGONUM RevisiDocument5 pagesTRIGONUM RevisidokteraanNo ratings yet
- Barrett Farm FoodDocument1 pageBarrett Farm FooddokteraanNo ratings yet
- 12 DHF DRDocument56 pages12 DHF DRdokteraanNo ratings yet
- TRIGONUM RevisiDocument5 pagesTRIGONUM RevisidokteraanNo ratings yet
- Bonefos PM Eng 22feb2007 112121Document27 pagesBonefos PM Eng 22feb2007 112121dokteraanNo ratings yet
- A B S T R A C TDocument2 pagesA B S T R A C TdokteraanNo ratings yet
- Guide to Head and Neck Physical ExamDocument39 pagesGuide to Head and Neck Physical ExamdokteraanNo ratings yet
- TRIGONUM RevisiDocument5 pagesTRIGONUM RevisidokteraanNo ratings yet
- Pelvic Fracture-Related Injuries of The Bladder Neck andDocument12 pagesPelvic Fracture-Related Injuries of The Bladder Neck anddokteraanNo ratings yet
- Hotchkiss 2013Document13 pagesHotchkiss 2013dokteraanNo ratings yet
- Zometa PI Nov2004Document23 pagesZometa PI Nov2004dokteraanNo ratings yet
- Abdominal Anatomy For GIST: The Peritoneum and RetroperitoneumDocument5 pagesAbdominal Anatomy For GIST: The Peritoneum and RetroperitoneumdokteraanNo ratings yet
- PneumothoraxDocument17 pagesPneumothoraxRizal FadhlurrahmanNo ratings yet
- Inguinal HerniaDocument14 pagesInguinal HerniaSakinah Mar'ie SanadNo ratings yet
- Cancer Is An Abnormal Disorganised Growth of Cells in The: PrintDocument1 pageCancer Is An Abnormal Disorganised Growth of Cells in The: Printshailesh284No ratings yet
- Guide to Decompressive Craniectomy for Severe Head InjuryDocument8 pagesGuide to Decompressive Craniectomy for Severe Head InjurydokteraanNo ratings yet
- Cuci Tangan, Sarung Tangan, Gaun Dan Mask 05.06Document18 pagesCuci Tangan, Sarung Tangan, Gaun Dan Mask 05.06Dewi Ayu Puspitasari TwinNo ratings yet
- Handbook of PEDIATRIC SURGERY PDFDocument43 pagesHandbook of PEDIATRIC SURGERY PDFPETERNo ratings yet
- Output PathDocument4 pagesOutput PathdokteraanNo ratings yet
- CUPS Pediatric Trauma EvaluationDocument2 pagesCUPS Pediatric Trauma EvaluationdokteraanNo ratings yet
- Good Surgical PracticeDocument10 pagesGood Surgical PracticedokteraanNo ratings yet
- Gastroscizis IngDocument1 pageGastroscizis IngdokteraanNo ratings yet
- Good Surgical PracticeDocument10 pagesGood Surgical PracticedokteraanNo ratings yet
- Lay Out LT 2Document1 pageLay Out LT 2dokteraanNo ratings yet
- A Rabbit Once Lived in A Forest With A LionDocument1 pageA Rabbit Once Lived in A Forest With A LionheriNo ratings yet
- Document 3Document2 pagesDocument 3Berta EliesNo ratings yet
- GGL Pelvis DelimitareDocument12 pagesGGL Pelvis DelimitareStefan AnaNo ratings yet
- Improving Goat Production in The Tropics: A Manual For Development WorkersDocument22 pagesImproving Goat Production in The Tropics: A Manual For Development WorkersOxfamNo ratings yet
- Getting Out of ItDocument36 pagesGetting Out of ItNavneet ChaubeyNo ratings yet
- Oral RevalidaDocument98 pagesOral RevalidaJay ArNo ratings yet
- Abdominal Mass Differential PresentationDocument42 pagesAbdominal Mass Differential Presentationdeb haartNo ratings yet
- Procedures Used in The Management of DystociaDocument17 pagesProcedures Used in The Management of DystociaVeterinary Online InstituteNo ratings yet
- Willard 2007 GastroenterologíaDocument65 pagesWillard 2007 GastroenterologíaHazel.No ratings yet
- Li̇mi̇t Tyt 15 Matemati̇k DenemeDocument151 pagesLi̇mi̇t Tyt 15 Matemati̇k Denemejibolok563No ratings yet
- Skin and Its Applied AnatomyDocument56 pagesSkin and Its Applied AnatomyShailesh PatilNo ratings yet
- Study Questions: CHAPTER 8 Microscopic Examination of Urine SedimentDocument7 pagesStudy Questions: CHAPTER 8 Microscopic Examination of Urine SedimentTiara YantaNo ratings yet
- Homeostasis and Higher Brain FunctionsDocument84 pagesHomeostasis and Higher Brain Functionsbodeadumitru9261No ratings yet
- Health Declaration Form: (Buong Pangalan) (Petsa) (Oras) (Kasa/ukuyang Tirahan) : (Numero NG Telepono)Document1 pageHealth Declaration Form: (Buong Pangalan) (Petsa) (Oras) (Kasa/ukuyang Tirahan) : (Numero NG Telepono)Reichmond LegaspiNo ratings yet
- Causes of Foamy UrineDocument12 pagesCauses of Foamy UrineAishwariyaaAngelinaStephenNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakayunyhafitryNo ratings yet
- For Cardiopulmonary Resuscitation and Emergency Cardiovascular CareDocument21 pagesFor Cardiopulmonary Resuscitation and Emergency Cardiovascular CareJoaco96No ratings yet
- Echolation: Echolation Is Recognized As A Method Utilized by A Variety of Aquatic, Nocturnal, and CaveDocument9 pagesEcholation: Echolation Is Recognized As A Method Utilized by A Variety of Aquatic, Nocturnal, and CaveJaimin K PatelNo ratings yet
- Parvoviruses: Structure, Replication, DiseasesDocument8 pagesParvoviruses: Structure, Replication, DiseasesAldila safitriNo ratings yet
- Csi - Glenda LongoriaDocument11 pagesCsi - Glenda Longoriaapi-302707617No ratings yet
- Cell Culture PDFDocument12 pagesCell Culture PDFSherwann Vergara Delos ReyesNo ratings yet
- LECTURE 1 - Respiratory SystemDocument1 pageLECTURE 1 - Respiratory SystemJeremiah AndalNo ratings yet