You might also like
- Chikungunya Virus Disease: Ii. Clinical InformationDocument2 pagesChikungunya Virus Disease: Ii. Clinical Informationkbl27No ratings yet
- Medical Examination: Subang Polyclinic SDN BHDDocument5 pagesMedical Examination: Subang Polyclinic SDN BHDSubang polylinicNo ratings yet
- Anthrax CifDocument2 pagesAnthrax CifMary Anne Grace GarridoNo ratings yet
- Case Investigation Form - Measles-RubellaDocument2 pagesCase Investigation Form - Measles-Rubellaclaverialc10No ratings yet
- Multi Disciplinary Hosp Discharge PlanDocument4 pagesMulti Disciplinary Hosp Discharge PlanDewi Angel BertNo ratings yet
- Otorhinolaryngology, Head & Neck Surgery Department Cornwall Regional Hospital (W.R.H.A)Document1 pageOtorhinolaryngology, Head & Neck Surgery Department Cornwall Regional Hospital (W.R.H.A)Giovanni HenryNo ratings yet
- Notifiable Conditions FormDocument3 pagesNotifiable Conditions FormDarius DeeNo ratings yet
- WK4Assgn1 1Document11 pagesWK4Assgn1 1G29T44Z69No ratings yet
- Influenza FormDocument2 pagesInfluenza FormDipendra PoudelNo ratings yet
- COVID-19 Patient Reporting Form: Reporter InformationDocument2 pagesCOVID-19 Patient Reporting Form: Reporter InformationShinta Devianti100% (1)
- Mortality Aaudit FormatDocument6 pagesMortality Aaudit FormatCOO TOP STARNo ratings yet
- Revised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Document3 pagesRevised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)テレビスマートNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Document8 pagesPhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Chrysanthus HerreraNo ratings yet
- 01.17bmQT10 Health Examination ReportDocument6 pages01.17bmQT10 Health Examination ReportKita 09No ratings yet
- Centro Escolar University Hospital: Patient'S Medical RecordDocument9 pagesCentro Escolar University Hospital: Patient'S Medical RecordjeyjeyNo ratings yet
- Mortality & Death Audit FormatsDocument6 pagesMortality & Death Audit FormatsAnindya BiswasNo ratings yet
- Health Examination Report SECTION 1 (To Be Completed by Candidate) (PART A)Document5 pagesHealth Examination Report SECTION 1 (To Be Completed by Candidate) (PART A)Fifi AinNo ratings yet
- D ReportDocument2 pagesD ReportHihiNo ratings yet
- Medical CertDocument1 pageMedical CertCharan JaganNo ratings yet
- CIF PertussisDocument2 pagesCIF PertussisDan Joseph AguilarNo ratings yet
- Guidelines To Fill in Health Examination ReportDocument6 pagesGuidelines To Fill in Health Examination ReportNurman HidayatNo ratings yet
- Case Report Form For HFMDDocument2 pagesCase Report Form For HFMDMendez RhuNo ratings yet
- CRF HFMD AsmghDocument2 pagesCRF HFMD AsmghRyeowook RyeNo ratings yet
- Measles CIF 2014Document2 pagesMeasles CIF 2014RionaMarieMagbutayNo ratings yet
- Articulo 3-EritemaDocument4 pagesArticulo 3-EritemaMariuxi CastroNo ratings yet
- Medical Examination FormDocument2 pagesMedical Examination FormSigit Sugiyanto0% (1)
- Lesson 13. Pediatric UnitDocument21 pagesLesson 13. Pediatric UnitPaola ChaconNo ratings yet
- DengueDocument2 pagesDengueTherence Marie LacsonNo ratings yet
- Kolej Teknologi Darulnaim: Darulnaim College of TechnologyDocument5 pagesKolej Teknologi Darulnaim: Darulnaim College of TechnologyDaryanto SutejiNo ratings yet
- Zika IcifDocument2 pagesZika IcifMarav SymbNo ratings yet
- Reliance Health Insurance Pre Authorisation FormDocument4 pagesReliance Health Insurance Pre Authorisation FormM/s MicrotechNo ratings yet
- Form G Health Examination Report International StudentDocument6 pagesForm G Health Examination Report International StudentVictor OjukwuNo ratings yet
- COVID-19 Test Request Form: Reporter InformationDocument1 pageCOVID-19 Test Request Form: Reporter InformationduckoduckNo ratings yet
- New Axa FormDocument2 pagesNew Axa FormAzrul Azuar Azrul Azuar100% (1)
- 'NEXtCARE Egypt - Reimbursement FormDocument1 page'NEXtCARE Egypt - Reimbursement FormMohyee Eldin RagebNo ratings yet
- Review InflamDocument17 pagesReview Inflamlovelove DayoNo ratings yet
- 2017 Certificate of Health 1Document2 pages2017 Certificate of Health 1herman syahNo ratings yet
- Discharge Summary: Diagnosis: Operative Procedure (If Any)Document2 pagesDischarge Summary: Diagnosis: Operative Procedure (If Any)Natasha BhasinNo ratings yet
- Maklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Document9 pagesMaklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Syazwi BaharuddinNo ratings yet
- Claim - Form - 001Document2 pagesClaim - Form - 001nitinmisra77No ratings yet
- Reimbursement Form: DD /MM /yyyyDocument1 pageReimbursement Form: DD /MM /yyyyfadi713No ratings yet
- Medical Claim - Doctor'S Statement: Patient's Personal DetailsDocument3 pagesMedical Claim - Doctor'S Statement: Patient's Personal DetailsWeng Meng VISTANo ratings yet
- ISARIC COVID-19 CRF V1.3 24feb2020Document12 pagesISARIC COVID-19 CRF V1.3 24feb2020ARINTA DWI KOMALANo ratings yet
- Contoh CV Untuk Nursing MalaysiaDocument4 pagesContoh CV Untuk Nursing MalaysiaWahyudin Aziz100% (1)
- Home WorkDocument6 pagesHome WorkChristina MurphyNo ratings yet
- New Query LetterDocument13 pagesNew Query LettersyawalNo ratings yet
- AFP FormDocument1 pageAFP FormSerenity Zay'sNo ratings yet
- CIF-MR 2022 Ver1Document2 pagesCIF-MR 2022 Ver1Ivy marie BonNo ratings yet
- (Delta Cluster) Pre-Employment Medical ChecklistDocument1 page(Delta Cluster) Pre-Employment Medical ChecklistwawanNo ratings yet
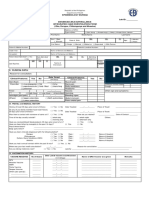
- Pidsr CifDocument17 pagesPidsr CifAbraham Asto100% (4)
- Fourth Year Logbook: Hawler Medical University College of Medicine Department of Medicine 2019-2020Document9 pagesFourth Year Logbook: Hawler Medical University College of Medicine Department of Medicine 2019-2020asia groupNo ratings yet
- Medical Examinations Form PANAMADocument4 pagesMedical Examinations Form PANAMADany David-Diculescu56% (9)
- Godavari College of Nursing, Jalgaon: Daily Clinical Dairy ReportDocument6 pagesGodavari College of Nursing, Jalgaon: Daily Clinical Dairy ReportbuntyNo ratings yet
- C105a Pre-Sea and Periodic Medical Fitness Examinations For SeafarersDocument4 pagesC105a Pre-Sea and Periodic Medical Fitness Examinations For SeafarersAbu ShabeelNo ratings yet
- Proforma For Sample Submission of A Suspected Case of Zika Virus DiseaseDocument1 pageProforma For Sample Submission of A Suspected Case of Zika Virus DiseaseGSPNo ratings yet
- One Page Modified Surveillance FormDocument1 pageOne Page Modified Surveillance FormAli FrhdNo ratings yet
- CovidreportformDocument1 pageCovidreportformapi-460314063No ratings yet
- CIF DiphDocument2 pagesCIF DiphIvy marie BonNo ratings yet
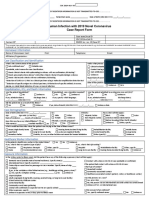
- Human Infection With 2019 Novel Coronavirus Case Report FormDocument2 pagesHuman Infection With 2019 Novel Coronavirus Case Report FormRicardo F. BernardinelliNo ratings yet
- Sgna Stand of Infection Control 0812 FINAL PDFDocument23 pagesSgna Stand of Infection Control 0812 FINAL PDFMarvin BautistaNo ratings yet
- Driver ContractDocument2 pagesDriver ContractMarvin Bautista100% (1)
- 5th JCI Monitoring Tool - Copy05052017Document8 pages5th JCI Monitoring Tool - Copy05052017Marvin BautistaNo ratings yet
- Antimicrobial Stewardship PCarling 062713Document58 pagesAntimicrobial Stewardship PCarling 062713Marvin BautistaNo ratings yet
- PIDAC Cleaning Disinfection and Sterilization 2013 PDFDocument117 pagesPIDAC Cleaning Disinfection and Sterilization 2013 PDFMarvin BautistaNo ratings yet
- Apple Developer AgreementDocument6 pagesApple Developer AgreementRaamRajaNo ratings yet
- 1practice Test Haad Prometrics DHA and MOH SamplerDocument48 pages1practice Test Haad Prometrics DHA and MOH SamplerMarvin Bautista100% (1)
- Volume 4.4 Nursing Service Facility PDFDocument23 pagesVolume 4.4 Nursing Service Facility PDFRhod Bernaldez EstaNo ratings yet
- 4.5 Routine Practices Formerly Infection ControlDocument4 pages4.5 Routine Practices Formerly Infection ControlMarvin BautistaNo ratings yet
- Bacterial Meningitis: (ICD 10 Code: A87)Document2 pagesBacterial Meningitis: (ICD 10 Code: A87)Marvin BautistaNo ratings yet
- Generic and Trade Name of AntibioticsDocument1 pageGeneric and Trade Name of AntibioticsMarvin BautistaNo ratings yet
- Pricelist LegalsizeDocument2 pagesPricelist LegalsizeMarvin BautistaNo ratings yet
- RD DFA AuthenticationDocument2 pagesRD DFA AuthenticationMarvin BautistaNo ratings yet
- 1practice Test Haad Prometrics DHA and MOH SamplerDocument48 pages1practice Test Haad Prometrics DHA and MOH SamplerMarvin Bautista100% (1)
- DARDocument4 pagesDARfritzroseNo ratings yet
- Inspection DrugtestingDocument29 pagesInspection DrugtestingMarvin BautistaNo ratings yet
- Monitoring and MovementDocument10 pagesMonitoring and MovementMarvin BautistaNo ratings yet
- Health Care Waste Management Manual 3rd EdDocument216 pagesHealth Care Waste Management Manual 3rd Edhgciso50% (2)
- HAAD RequirementsDocument2 pagesHAAD RequirementscloydmarvinpsegundoNo ratings yet
- Infection Control Assessment Tool User ManualDocument30 pagesInfection Control Assessment Tool User ManualMarvin BautistaNo ratings yet
- Practice Quiz Answers Unit 1Document5 pagesPractice Quiz Answers Unit 1Marvin BautistaNo ratings yet
- 6 14 13 New Long SRP PriceDocument2 pages6 14 13 New Long SRP PriceMarvin BautistaNo ratings yet
- Editor'S Forum: Paul Byrne, MB, CHB, FRCPCDocument12 pagesEditor'S Forum: Paul Byrne, MB, CHB, FRCPCMarvin BautistaNo ratings yet
- The Care of Surgical Instruments PDFDocument38 pagesThe Care of Surgical Instruments PDFMarvin BautistaNo ratings yet
- Imogen Powerpoint DesignDocument29 pagesImogen Powerpoint DesignArthur100% (1)
- B. Inggris Narrative TeksDocument11 pagesB. Inggris Narrative TeksDew FitriNo ratings yet
- Churches That Have Left RCCG 0722 PDFDocument2 pagesChurches That Have Left RCCG 0722 PDFKadiri JohnNo ratings yet
- 1634313583!Document24 pages1634313583!Joseph Sanchez TalusigNo ratings yet
- Personal Training Program Design Using FITT PrincipleDocument1 pagePersonal Training Program Design Using FITT PrincipleDan DanNo ratings yet
- Nikulin D. - Imagination and Mathematics in ProclusDocument20 pagesNikulin D. - Imagination and Mathematics in ProclusannipNo ratings yet
- GemDocument135 pagesGemZelia GregoriouNo ratings yet
- ITC Green Centre: Gurgaon, IndiaDocument19 pagesITC Green Centre: Gurgaon, IndiaAgastya Dasari100% (2)
- Conductivity MeterDocument59 pagesConductivity MeterMuhammad AzeemNo ratings yet
- Tour Guiding and Escort Services - 301Document95 pagesTour Guiding and Escort Services - 301Zane 19531No ratings yet
- Group 4 - Regional and Social DialectDocument12 pagesGroup 4 - Regional and Social DialectazizaNo ratings yet
- TestDocument56 pagesTestFajri Love PeaceNo ratings yet
- Pediatric ECG Survival Guide - 2nd - May 2019Document27 pagesPediatric ECG Survival Guide - 2nd - May 2019Marcos Chusin MontesdeocaNo ratings yet
- SET UP Computer ServerDocument3 pagesSET UP Computer ServerRicHArdNo ratings yet
- Crime Scene Drawing January Incident 10501-10600Document100 pagesCrime Scene Drawing January Incident 10501-10600columbinefamilyrequest100% (2)
- Narrative ReportDocument6 pagesNarrative ReportAlyssa Marie AsuncionNo ratings yet
- Rebecca Young Vs CADocument3 pagesRebecca Young Vs CAJay RibsNo ratings yet
- Nandurbar District S.E. (CGPA) Nov 2013Document336 pagesNandurbar District S.E. (CGPA) Nov 2013Digitaladda IndiaNo ratings yet
- DLP No. 10 - Literary and Academic WritingDocument2 pagesDLP No. 10 - Literary and Academic WritingPam Lordan83% (12)
- Nursing Education and Nursing Service ProgramsDocument10 pagesNursing Education and Nursing Service ProgramsLevy DuranNo ratings yet
- Feuerhahn Funeral Bullet 17 March 2015Document12 pagesFeuerhahn Funeral Bullet 17 March 2015brandy99No ratings yet
- Test AmeeshDocument7 pagesTest AmeeshUdit DravidNo ratings yet
- 23 East 4Th Street NEW YORK, NY 10003 Orchard Enterprises Ny, IncDocument2 pages23 East 4Th Street NEW YORK, NY 10003 Orchard Enterprises Ny, IncPamelaNo ratings yet
- Conrad John's ResumeDocument1 pageConrad John's ResumeTraining & OD HRODNo ratings yet
- PT - Science 5 - Q1Document4 pagesPT - Science 5 - Q1Jomelyn MaderaNo ratings yet
- Abramson, Glenda (Ed.) - Oxford Book of Hebrew Short Stories (Oxford, 1996) PDFDocument424 pagesAbramson, Glenda (Ed.) - Oxford Book of Hebrew Short Stories (Oxford, 1996) PDFptalus100% (2)
- Logic of English - Spelling Rules PDFDocument3 pagesLogic of English - Spelling Rules PDFRavinder Kumar80% (15)
- Trần Phương Mai - Literature - Irony in "Letter to a Funeral Parlor" by Lydia DavisDocument2 pagesTrần Phương Mai - Literature - Irony in "Letter to a Funeral Parlor" by Lydia DavisTrần Phương MaiNo ratings yet
- FIREXDocument2 pagesFIREXPausNo ratings yet
- Echeverria Motion For Proof of AuthorityDocument13 pagesEcheverria Motion For Proof of AuthorityIsabel SantamariaNo ratings yet