You might also like
- STATE OF NEW MEXICO v. BRIAN ADAMSDocument22 pagesSTATE OF NEW MEXICO v. BRIAN ADAMSDaily TimesNo ratings yet
- Director, Office of Workers' Compensation Programs, U.S. Department of Labor v. William Siwiec, 894 F.2d 635, 3rd Cir. (1990)Document8 pagesDirector, Office of Workers' Compensation Programs, U.S. Department of Labor v. William Siwiec, 894 F.2d 635, 3rd Cir. (1990)Scribd Government DocsNo ratings yet
- Genetic Technologies v. GenelexDocument10 pagesGenetic Technologies v. GenelexPatent LitigationNo ratings yet
- D'arcy Full Text PDFDocument99 pagesD'arcy Full Text PDFRene MolinaNo ratings yet
- Manuel Mascarenas v. Director, Office of Workers' Compensation Programs, United States Department of Labor, Pittsburg & Midway Coal Mining Company, Real Party in Interest, 52 F.3d 338, 10th Cir. (1995)Document3 pagesManuel Mascarenas v. Director, Office of Workers' Compensation Programs, United States Department of Labor, Pittsburg & Midway Coal Mining Company, Real Party in Interest, 52 F.3d 338, 10th Cir. (1995)Scribd Government DocsNo ratings yet
- James Kenneth Gallagher v. National Transportation Safety Board and Administrator, Federal Aviation Administration, 953 F.2d 1214, 10th Cir. (1992)Document15 pagesJames Kenneth Gallagher v. National Transportation Safety Board and Administrator, Federal Aviation Administration, 953 F.2d 1214, 10th Cir. (1992)Scribd Government DocsNo ratings yet
- United States Court of Appeals, Third CircuitDocument5 pagesUnited States Court of Appeals, Third CircuitScribd Government DocsNo ratings yet
- Memo and OpinionDocument12 pagesMemo and OpinionMMA PayoutNo ratings yet
- Rule On Dna EvidenceDocument18 pagesRule On Dna EvidenceArmiNo ratings yet
- Alcohol Blood TestingDocument5 pagesAlcohol Blood TestingYusnida RahmawatiNo ratings yet
- Benson Hill Biosystems Vs The Broad Institute '490 CRISPR Institution DenialDocument21 pagesBenson Hill Biosystems Vs The Broad Institute '490 CRISPR Institution DenialTradeHawkNo ratings yet
- OPRA - 4.11.2022 - DOJ Subpoena, OCDocument10 pagesOPRA - 4.11.2022 - DOJ Subpoena, OCShore News NetworkNo ratings yet
- US7729440 OCredDocument369 pagesUS7729440 OCredsanilg81No ratings yet
- USA v. Stewart ParnellDocument40 pagesUSA v. Stewart ParnellUnited Press InternationalNo ratings yet
- Shekhawati Form - FDocument2 pagesShekhawati Form - FArchit ChampanekarNo ratings yet
- A.M. No. 06-11-5-SC Rules On DNA EvidenceDocument4 pagesA.M. No. 06-11-5-SC Rules On DNA EvidenceVida Urduja B. Liwag-CenaNo ratings yet
- Director, Office of Workers' Compensation Programs, United States Department of Labor v. August Mangifest, 826 F.2d 1318, 3rd Cir. (1987)Document27 pagesDirector, Office of Workers' Compensation Programs, United States Department of Labor v. August Mangifest, 826 F.2d 1318, 3rd Cir. (1987)Scribd Government DocsNo ratings yet
- United States Court of Appeals, Third CircuitDocument6 pagesUnited States Court of Appeals, Third CircuitScribd Government DocsNo ratings yet
- AO No. 2007-0025 PEME For Seafarers Related Documents PDFDocument26 pagesAO No. 2007-0025 PEME For Seafarers Related Documents PDFmariaNo ratings yet
- Blood Bank ManualDocument29 pagesBlood Bank ManualMarice Ferrufino SchmidtNo ratings yet
- Chapter 18 Path and Lab Set BDocument4 pagesChapter 18 Path and Lab Set BBernard Paul Guinto0% (1)
- Understanding Post Mortem Blood Testing Practices For Tissue Donation Complementary Information Received in The SurveyDocument45 pagesUnderstanding Post Mortem Blood Testing Practices For Tissue Donation Complementary Information Received in The SurveyMariana SeguraNo ratings yet
- United States Court of Appeals, Fourth CircuitDocument7 pagesUnited States Court of Appeals, Fourth CircuitScribd Government DocsNo ratings yet
- Blood Centre RequirementsDocument12 pagesBlood Centre Requirementssanket.bera8642No ratings yet
- Rules On DNA EvidenceDocument35 pagesRules On DNA EvidenceCharina BalunsoNo ratings yet
- Joey Gareri, M.Sc. Response To Dr. Chatterton Witness StatementDocument11 pagesJoey Gareri, M.Sc. Response To Dr. Chatterton Witness StatementToronto StarNo ratings yet
- United States Court of Appeals, Third CircuitDocument12 pagesUnited States Court of Appeals, Third CircuitScribd Government DocsNo ratings yet
- Guidelines On Hospital Blood Bank DocumeDocument12 pagesGuidelines On Hospital Blood Bank DocumeGazzzeeNo ratings yet
- FDA Letter To 23andmeDocument10 pagesFDA Letter To 23andmeSarahNo ratings yet
- Specimen CollectionDocument66 pagesSpecimen Collectionadelmam55No ratings yet
- In The Supreme Court of Oklahoma: Case NoDocument11 pagesIn The Supreme Court of Oklahoma: Case NosnippyxNo ratings yet
- Specimen CollectionDocument20 pagesSpecimen Collectionnikh86100% (4)
- Michael Revak v. National Mines Corporation and Old Republic Companies, and Director, Office of Workers' Compensation Programs, Party-In-Interest, 808 F.2d 996, 3rd Cir. (1987)Document14 pagesMichael Revak v. National Mines Corporation and Old Republic Companies, and Director, Office of Workers' Compensation Programs, Party-In-Interest, 808 F.2d 996, 3rd Cir. (1987)Scribd Government DocsNo ratings yet
- GH PatentDocument24 pagesGH PatentCharles GrossNo ratings yet
- Lab Policy and ProceduresDocument8 pagesLab Policy and ProceduresvasanthrsciwiaNo ratings yet
- Kaiser Steel Corporation v. Director, Office of Workers' Compensation Programs, United States Department of Labor, and Jesse Sainz, 748 F.2d 1426, 10th Cir. (1984)Document7 pagesKaiser Steel Corporation v. Director, Office of Workers' Compensation Programs, United States Department of Labor, and Jesse Sainz, 748 F.2d 1426, 10th Cir. (1984)Scribd Government DocsNo ratings yet
- Kyle Bass Vs Acorda Therapeutics Ampyra Patent Claims IPR Final Written DecisionDocument56 pagesKyle Bass Vs Acorda Therapeutics Ampyra Patent Claims IPR Final Written DecisionTradeHawkNo ratings yet
- 8614 Notice of Filing of Application of Michael S Green For Access To Protected Information 2Document3 pages8614 Notice of Filing of Application of Michael S Green For Access To Protected Information 2dpsimswmNo ratings yet
- GRP Specimenhandbook en 2004122807Document16 pagesGRP Specimenhandbook en 2004122807AlibabarNo ratings yet
- Automated Medical Laboratories, Inc. v. Hillsborough County, Florida, and Hillsborough County Health Department, 722 F.2d 1526, 11th Cir. (1984)Document11 pagesAutomated Medical Laboratories, Inc. v. Hillsborough County, Florida, and Hillsborough County Health Department, 722 F.2d 1526, 11th Cir. (1984)Scribd Government DocsNo ratings yet
- Form B: Non-Invasive InvasiveDocument12 pagesForm B: Non-Invasive InvasiveSrikanth KanagasabapathyNo ratings yet
- Ernest Gutierrez v. Joseph A. Califano, JR., Secretary of Health, Education and Welfare, Defendant-Appellant, 612 F.2d 1247, 10th Cir. (1980)Document4 pagesErnest Gutierrez v. Joseph A. Califano, JR., Secretary of Health, Education and Welfare, Defendant-Appellant, 612 F.2d 1247, 10th Cir. (1980)Scribd Government DocsNo ratings yet
- Sperduti Court OrderDocument7 pagesSperduti Court OrderCarrie HodginNo ratings yet
- Form 41Document1 pageForm 41Grace C.No ratings yet
- Filed: Patrick FisherDocument7 pagesFiled: Patrick FisherScribd Government DocsNo ratings yet
- Etonogestrel Subdermal Implant For The Management of Endometriosis-Associated Pain After Ovarian-Sparing SurgeryDocument3 pagesEtonogestrel Subdermal Implant For The Management of Endometriosis-Associated Pain After Ovarian-Sparing SurgeryArman Renz PauloNo ratings yet
- FEI1010894Document40 pagesFEI1010894gramirez2012No ratings yet
- United States Court of Appeals, Fourth CircuitDocument6 pagesUnited States Court of Appeals, Fourth CircuitScribd Government DocsNo ratings yet
- Lung Cancer Testing Request Form LatestDocument2 pagesLung Cancer Testing Request Form LatestHanafiah SematNo ratings yet
- Bloodcomponents: Screening of Single-Donor Apheresis Platelets For Bacterial Contamination: The PASSPORT Study ResultsDocument11 pagesBloodcomponents: Screening of Single-Donor Apheresis Platelets For Bacterial Contamination: The PASSPORT Study Resultsmy accountNo ratings yet
- 2015-07-08 Sample Motion To Preserve-1Document8 pages2015-07-08 Sample Motion To Preserve-1Justice CauseNo ratings yet
- Ex Parte Schulhauser 2016 - 04 - 28Document22 pagesEx Parte Schulhauser 2016 - 04 - 28Wartan WuNo ratings yet
- Elm Grove Coal Company v. Director, Office of Workers' Compensation Programs, United States Department of Labor Velma Blake, Widow of Ivan Randall Blake, 480 F.3d 278, 4th Cir. (2007)Document31 pagesElm Grove Coal Company v. Director, Office of Workers' Compensation Programs, United States Department of Labor Velma Blake, Widow of Ivan Randall Blake, 480 F.3d 278, 4th Cir. (2007)Scribd Government DocsNo ratings yet
- United States v. Katso, C.A.A.F. (2015)Document41 pagesUnited States v. Katso, C.A.A.F. (2015)Scribd Government DocsNo ratings yet
- Brief in Support of Motion For Daubert Hearing, Suppression and Dismissal (Sotoxa)Document7 pagesBrief in Support of Motion For Daubert Hearing, Suppression and Dismissal (Sotoxa)Jeffrey NewtonNo ratings yet
- Federal Register / Vol. 76, No. 248 / Tuesday, December 27, 2011 / NoticesDocument2 pagesFederal Register / Vol. 76, No. 248 / Tuesday, December 27, 2011 / NoticesDorje PhagmoNo ratings yet
- Stem Cell RegistrationDocument5 pagesStem Cell Registrationv9991 v9991No ratings yet
- United States v. Frank Klimek, 411 F.3d 50, 2d Cir. (2005)Document6 pagesUnited States v. Frank Klimek, 411 F.3d 50, 2d Cir. (2005)Scribd Government DocsNo ratings yet
- Kisting-Leung v. Cigna - Complaint in Lawsuit Re Algorithmic Denials of Health Insurance ClaimsDocument18 pagesKisting-Leung v. Cigna - Complaint in Lawsuit Re Algorithmic Denials of Health Insurance ClaimsKirk HartleyNo ratings yet
- Cooley Fee Petition - LTLDocument306 pagesCooley Fee Petition - LTLKirk HartleyNo ratings yet
- Detailed Account of The Gutting of The IRSDocument14 pagesDetailed Account of The Gutting of The IRSKirk HartleyNo ratings yet
- K&E Fee Statememt Aero Oct $3.93 MillionDocument238 pagesK&E Fee Statememt Aero Oct $3.93 MillionKirk HartleyNo ratings yet
- LTL 4-20-23 Hearing - Ruling - TR - Ex A To Docket 83Document28 pagesLTL 4-20-23 Hearing - Ruling - TR - Ex A To Docket 83Kirk HartleyNo ratings yet
- Brown Rudnick Fee Petition - LTLDocument313 pagesBrown Rudnick Fee Petition - LTLKirk HartleyNo ratings yet
- Massey & Gail Fee Petition - LTLDocument74 pagesMassey & Gail Fee Petition - LTLKirk HartleyNo ratings yet
- Imerys Disclosure Statement 1/28/21Document602 pagesImerys Disclosure Statement 1/28/21Kirk HartleyNo ratings yet
- Opinion Holding That Dominion Can Sue FoxDocument25 pagesOpinion Holding That Dominion Can Sue FoxKirk HartleyNo ratings yet
- Foster Wheeler (Ed Hugo) Petition For Cert Re California Limits On Deps by DefendantsDocument33 pagesFoster Wheeler (Ed Hugo) Petition For Cert Re California Limits On Deps by DefendantsKirk HartleyNo ratings yet
- LTL Brown Rudnik Fee Petition Feb 2022Document143 pagesLTL Brown Rudnik Fee Petition Feb 2022Kirk HartleyNo ratings yet
- STAT News - The ADA Covers Addiction. Now The U.S. Is Enforcing The Law (To Protect Former Addicts) - STATDocument13 pagesSTAT News - The ADA Covers Addiction. Now The U.S. Is Enforcing The Law (To Protect Former Addicts) - STATKirk HartleyNo ratings yet
- Courthouse News Serv. v. Forman - 2022 U.S. Dist. LEXISDocument9 pagesCourthouse News Serv. v. Forman - 2022 U.S. Dist. LEXISKirk HartleyNo ratings yet
- First Amendment Action Filed Against Columbus Clerk Over Access Blackout - Courthouse News ServiceDocument4 pagesFirst Amendment Action Filed Against Columbus Clerk Over Access Blackout - Courthouse News ServiceKirk HartleyNo ratings yet
- Justice NewsDocument2 pagesJustice NewsKirk HartleyNo ratings yet
- DOJ 2022 Article Re Civil Rights EnforcementDocument295 pagesDOJ 2022 Article Re Civil Rights EnforcementKirk HartleyNo ratings yet
- US Judge Enjoins Florida's E-Filing Authority On 1st Amendment Grounds - Courthouse News ServiceDocument5 pagesUS Judge Enjoins Florida's E-Filing Authority On 1st Amendment Grounds - Courthouse News ServiceKirk HartleyNo ratings yet
- Paxton Disc Pet Judicial Assignment 052522Document6 pagesPaxton Disc Pet Judicial Assignment 052522Kirk HartleyNo ratings yet
- Insurers' Motion To Intervene in Opposition To Narco Motion To Redact 4-28-2022Document100 pagesInsurers' Motion To Intervene in Opposition To Narco Motion To Redact 4-28-2022Kirk HartleyNo ratings yet
- My Pillow Sanctions OrderDocument31 pagesMy Pillow Sanctions OrderKirk HartleyNo ratings yet
- Gilson Declaration in Support - Lohmann - Plaintiffs Motion For Protective Order Regarding Pathology Testing and Genetic TestingDocument6 pagesGilson Declaration in Support - Lohmann - Plaintiffs Motion For Protective Order Regarding Pathology Testing and Genetic TestingKirk HartleyNo ratings yet
- Lohmann - Plaintiff's Motion For Protective Order Re Pathology and Genetic TestingDocument16 pagesLohmann - Plaintiff's Motion For Protective Order Re Pathology and Genetic TestingKirk HartleyNo ratings yet
- Purdue Chapter 11-Part 1 Notice of Appeal of Confirmation Order and Order Approving Disclosure StatementDocument4 pagesPurdue Chapter 11-Part 1 Notice of Appeal of Confirmation Order and Order Approving Disclosure StatementKirk HartleyNo ratings yet
- Purdue Chapter 11-Part 2.1 Notice of Appeal of Confirmation Order and Order Approving Disclosure Statement-2-2Document120 pagesPurdue Chapter 11-Part 2.1 Notice of Appeal of Confirmation Order and Order Approving Disclosure Statement-2-2Kirk HartleyNo ratings yet
- Purdue Chapter 11-Memo Re Expedited Stay MotionDocument45 pagesPurdue Chapter 11-Memo Re Expedited Stay MotionKirk HartleyNo ratings yet
- Purdue Chapter 11-Part 2.0 Notice of Appeal of Confirmation Order and Order Approving Disclosure Statement-2Document99 pagesPurdue Chapter 11-Part 2.0 Notice of Appeal of Confirmation Order and Order Approving Disclosure Statement-2Kirk HartleyNo ratings yet
- Purdue Chapter 11-Expedited Motion Re Stay of Confirmation OrderDocument12 pagesPurdue Chapter 11-Expedited Motion Re Stay of Confirmation OrderKirk HartleyNo ratings yet
- 1414-Electric Room 1 Calculation Report Rev.02Document28 pages1414-Electric Room 1 Calculation Report Rev.02zakariaelrayesusaNo ratings yet
- Electrical Inspections: Infrared ThermographyDocument28 pagesElectrical Inspections: Infrared ThermographyManish RajNo ratings yet
- The Effective SpanDocument4 pagesThe Effective SpanMohamed FarahNo ratings yet
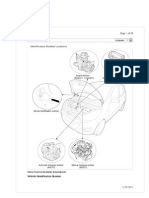
- I10 Workshop Manual - ADocument292 pagesI10 Workshop Manual - ANorthstartechnology Company82% (11)
- Proyector SNF 111Document3 pagesProyector SNF 111Liliana Patricia PederneraNo ratings yet
- Transformation of Modern Library in To Green Library For Sustaining FutureDocument7 pagesTransformation of Modern Library in To Green Library For Sustaining FutureHardik AnandNo ratings yet
- Fundamental and Technical Analysis of Iron and Steel SIP PROJECTDocument34 pagesFundamental and Technical Analysis of Iron and Steel SIP PROJECThaveuever910No ratings yet
- Gayatri Mantras of Several GodDocument10 pagesGayatri Mantras of Several GodAnup KashyapNo ratings yet
- Hipertensiunea Arteriala - Cauze Si TratamenteDocument25 pagesHipertensiunea Arteriala - Cauze Si TratamenteClaudia MurguNo ratings yet
- Origami PapiroflexiaDocument6 pagesOrigami PapiroflexiaBraulio RomeroNo ratings yet
- C.4. Quiz Conservation of BiodiversityDocument2 pagesC.4. Quiz Conservation of Biodiversitylaura pongutaNo ratings yet
- NEET MADE EJEE Complete Handwritten Formulae Chemistry NEET andDocument90 pagesNEET MADE EJEE Complete Handwritten Formulae Chemistry NEET andliyanderNo ratings yet
- 1-Theory of Metal Cutting PDFDocument144 pages1-Theory of Metal Cutting PDFNithinArvindNo ratings yet
- Labangon Elementary School Diagbostic Test in Epp/Tle 6 Directions: Multiple Choice. Choose The Correct The Letter of The Correct AnswerDocument4 pagesLabangon Elementary School Diagbostic Test in Epp/Tle 6 Directions: Multiple Choice. Choose The Correct The Letter of The Correct AnswerJulianFlorenzFalconeNo ratings yet
- Fighting The Sixth Mass ExtinctionDocument25 pagesFighting The Sixth Mass ExtinctionRichard J. MarksNo ratings yet
- 4 TH Sem UG Osmoregulation in Aquatic VertebratesDocument6 pages4 TH Sem UG Osmoregulation in Aquatic VertebratesBasak ShreyaNo ratings yet
- Instrumentation & Measurement SystemsDocument7 pagesInstrumentation & Measurement SystemsAnkit KumarNo ratings yet
- CCNP 300 410 ENARSI NetworkTUT 26 5 2021Document104 pagesCCNP 300 410 ENARSI NetworkTUT 26 5 2021Olga BradyNo ratings yet
- 4.dole Regulations On Safety Standards in ConstrDocument31 pages4.dole Regulations On Safety Standards in Constrmacky02 sorenatsacNo ratings yet
- Bugreport Dandelion - Eea QP1A.190711.020 2022 02 15 07 45 54Document9,715 pagesBugreport Dandelion - Eea QP1A.190711.020 2022 02 15 07 45 54João Carlos Pereira ChoinasNo ratings yet
- Energy and FluctuationDocument10 pagesEnergy and Fluctuationwalid Ait MazouzNo ratings yet
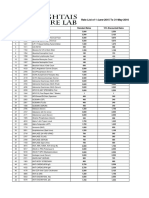
- Rate List of 1-June-2015 To 31-May-2016: S.No Code Test Name Standard Rates 15% Discounted RatesDocument25 pagesRate List of 1-June-2015 To 31-May-2016: S.No Code Test Name Standard Rates 15% Discounted RatesMirza BabarNo ratings yet
- The CyclotronDocument10 pagesThe CyclotronSupriya DuttaNo ratings yet
- Kasuti of KarnatakaDocument2 pagesKasuti of KarnatakarhlkNo ratings yet
- Grade 7 Information Writing: The Bulldog: A Dog Like No OtherDocument5 pagesGrade 7 Information Writing: The Bulldog: A Dog Like No Otherapi-202727113No ratings yet
- Kyocera 1800Document2 pagesKyocera 1800gendoetzNo ratings yet
- Deutz Fahr Rear Axle T 7100 Workshop ManualDocument22 pagesDeutz Fahr Rear Axle T 7100 Workshop Manualcindybennettmd040595jbw100% (133)
- Roles and Responsibilities of ASHADocument3 pagesRoles and Responsibilities of ASHAmohanpskohli8310No ratings yet
- SC607 Assignment2Document2 pagesSC607 Assignment2Tirthankar AdhikariNo ratings yet
- 3 Particle Nature of Matter PDFDocument4 pages3 Particle Nature of Matter PDFAtheer AlaniNo ratings yet