You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Arabic Language For Alarm Clock 2.0Document3 pagesArabic Language For Alarm Clock 2.0zeddy3No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- CCMN279-D10 F14 Course OutlineDocument4 pagesCCMN279-D10 F14 Course Outlinezeddy3No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Creative Suite 4 Master Collection Read MeDocument9 pagesCreative Suite 4 Master Collection Read MemwendiNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
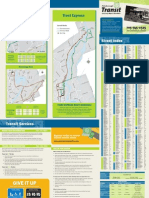
- Trent University August 2012 Transit MapDocument2 pagesTrent University August 2012 Transit Mapzeddy3No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Graph Paper 1mmDocument1 pageGraph Paper 1mmzeddy3No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- GRADES 1 To 12 Daily Lesson Log 7 Mapeh/Arts 4 MEETINGS/1hour Per Week 4 Quarter I. Objectives Session1 Session2 Session3 Session4Document4 pagesGRADES 1 To 12 Daily Lesson Log 7 Mapeh/Arts 4 MEETINGS/1hour Per Week 4 Quarter I. Objectives Session1 Session2 Session3 Session4Kirs Mrey100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Techniques de Rédaction de Texte PDFDocument8 pagesTechniques de Rédaction de Texte PDFAnonymous OG8ApT4goNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Agba Et AlDocument8 pagesAgba Et AlDiana CentaurusNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Couturat Chap2 PDFDocument10 pagesCouturat Chap2 PDFMari VojvodovicNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Markee Module 1 Session 1 Activity 2Document4 pagesMarkee Module 1 Session 1 Activity 2Markee JoyceNo ratings yet
- Following Are The Characteristics of Management:-: Umbrella Term MindDocument7 pagesFollowing Are The Characteristics of Management:-: Umbrella Term MindPrashi JainNo ratings yet
- Dynamics PsychologyDocument19 pagesDynamics PsychologyArvella AlbayNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Drawing Assessment CriteriaDocument1 pageDrawing Assessment Criteriaapi-254314751No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Syllabus English 8180: Composition TheoryDocument10 pagesSyllabus English 8180: Composition TheoryAshley HolmesNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Chapter 1 - 2Document11 pagesChapter 1 - 2Kyle Haunter0% (1)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- M Ed 1st Year Question Papers PsychologyDocument13 pagesM Ed 1st Year Question Papers PsychologyVIJAY KUMAR HEER100% (13)
- Rules, Reproducibility, and The Brief Frenzy of Animal Magnetism: Epistemological Foundations of Trust in French Enlightenment MedicineDocument32 pagesRules, Reproducibility, and The Brief Frenzy of Animal Magnetism: Epistemological Foundations of Trust in French Enlightenment MedicineMark TitlemanNo ratings yet
- 20161214221246predicates and QuantifiersDocument68 pages20161214221246predicates and QuantifiersIrfan FazailNo ratings yet
- Effective Basic Calculus DAMATH Strategy Improves STEM Students' PerformanceDocument17 pagesEffective Basic Calculus DAMATH Strategy Improves STEM Students' PerformanceHannah Beatrice A. Tamayo0% (1)
- Journalofphiloso07lancuoft BWDocument736 pagesJournalofphiloso07lancuoft BWPantheon PantheonNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Psikologi Belajar 1Document9 pagesPsikologi Belajar 1Gabriel Brilland HollandNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- PhilosophyDocument37 pagesPhilosophyLA LA LA LA LA MiniNo ratings yet
- Being Logical 4Document27 pagesBeing Logical 4heidi_olson09No ratings yet
- Reading StrategiesDocument78 pagesReading StrategiesSquirmy Cape9097No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Griffin 1-Understanding The Manager JobDocument13 pagesGriffin 1-Understanding The Manager JobMatiLilNo ratings yet
- New Framework of Intrinsic/Extrinsic and Integrative/Instrumental Motivation in Second Language AcquisitionDocument26 pagesNew Framework of Intrinsic/Extrinsic and Integrative/Instrumental Motivation in Second Language AcquisitionFarrah MohammedNo ratings yet
- Teaching Strategies Gold - Slide ShowDocument16 pagesTeaching Strategies Gold - Slide Showapi-301357311No ratings yet
- MGMT 650 Critical ReviewDocument3 pagesMGMT 650 Critical ReviewlaurenNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Sbar Mini Case StudiesDocument2 pagesSbar Mini Case Studiesapi-367705934No ratings yet
- Creative Project Rubric-Hero's Journey/Quarterly Reading BooksDocument1 pageCreative Project Rubric-Hero's Journey/Quarterly Reading BooksmaeydelNo ratings yet
- 177738e PDFDocument205 pages177738e PDFJonalyn LastimadoNo ratings yet
- Theology as the Foundation of MetaphysicsDocument20 pagesTheology as the Foundation of MetaphysicsHaris MacićNo ratings yet
- GAME Theory by (M.A.K. Pathan)Document12 pagesGAME Theory by (M.A.K. Pathan)M.A.K. S. PathanNo ratings yet
- Philosophical Semantics: (Oscar Wild, The Remarkable Rocket', 1888)Document10 pagesPhilosophical Semantics: (Oscar Wild, The Remarkable Rocket', 1888)Prevoditeljski studijNo ratings yet
- Ferguson, Stephen C. 2007 'Social Contract As Bourgeois Ideology' Cultural Logic (19 PP.)Document19 pagesFerguson, Stephen C. 2007 'Social Contract As Bourgeois Ideology' Cultural Logic (19 PP.)voxpop88No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)