You might also like
- Crisis Intervention SummaryDocument7 pagesCrisis Intervention Summarydennis8113100% (2)
- The Integrated Case Management Manual: Value-Based Assistance to Complex Medical and Behavioral Health PatientsFrom EverandThe Integrated Case Management Manual: Value-Based Assistance to Complex Medical and Behavioral Health PatientsNo ratings yet
- Module 2. Health Systems Framework (Section A)Document5 pagesModule 2. Health Systems Framework (Section A)Gian Rei MangcucangNo ratings yet
- HI12!64!73 PatientBehavior R8Document10 pagesHI12!64!73 PatientBehavior R8David IoanaNo ratings yet
- Nur 467 Portfolio Scholarly Work 1 02 17 14Document8 pagesNur 467 Portfolio Scholarly Work 1 02 17 14api-247935508No ratings yet
- Person Centred Care Literature ReviewDocument8 pagesPerson Centred Care Literature Reviewnidokyjynuv2100% (1)
- Efficacy, Effectiveness And Efficiency In The Management Of Health SystemsFrom EverandEfficacy, Effectiveness And Efficiency In The Management Of Health SystemsNo ratings yet
- Narrative ScriptDocument8 pagesNarrative ScriptNaftali WambaloNo ratings yet
- Case ManagementDocument37 pagesCase Managementmousa derhemNo ratings yet
- ASS134 FeDocument6 pagesASS134 Febright osakweNo ratings yet
- 14 Supporting Prevention and Chronic Condition Self-ManagementDocument8 pages14 Supporting Prevention and Chronic Condition Self-Managementilham apriadiNo ratings yet
- Integrated Health Services - What and Why ?: Main MessagesDocument8 pagesIntegrated Health Services - What and Why ?: Main MessageslewisbrealNo ratings yet
- Collaborative CareDocument16 pagesCollaborative CareArdhani IrfanNo ratings yet
- The Common Threads in ProgramDocument5 pagesThe Common Threads in Programdate6No ratings yet
- Health Seeking BehaviourDocument27 pagesHealth Seeking BehaviourRommel IrabagonNo ratings yet
- Coordinating Health ServicesDocument25 pagesCoordinating Health ServicesbdivanNo ratings yet
- Patient Empowerment BMC Health Services Research2012Document8 pagesPatient Empowerment BMC Health Services Research2012Constantino SantosNo ratings yet
- Praktik Bahasa InggrisDocument5 pagesPraktik Bahasa InggrisApdalNo ratings yet
- Assignment 5 Public Health Preparedness 1579051Document9 pagesAssignment 5 Public Health Preparedness 1579051Ravi KumawatNo ratings yet
- Module 1Document4 pagesModule 1ronald tadicNo ratings yet
- Week 1 1Document8 pagesWeek 1 1R-jeyn TorresNo ratings yet
- Evidence Based RUADocument12 pagesEvidence Based RUAAsma AliNo ratings yet
- Dissertation Funding Public HealthDocument5 pagesDissertation Funding Public HealthWriteMyPaperCanadaUK100% (1)
- Fall Prevention Research PaperDocument8 pagesFall Prevention Research Paperorlfgcvkg100% (1)
- Dissertation Examples in Public HealthDocument6 pagesDissertation Examples in Public HealthProfessionalPaperWriterCanada100% (1)
- Primary Health Care Literature ReviewDocument4 pagesPrimary Health Care Literature Reviewafdtbluwq100% (1)
- Case StudyDocument38 pagesCase StudyJurryNo ratings yet
- Order 941 - EconomicinfluencesDocument9 pagesOrder 941 - EconomicinfluencesVenus Marie Real-CatubayNo ratings yet
- Approach To The Patient - UpToDateDocument35 pagesApproach To The Patient - UpToDateAmrutesh KhodkeNo ratings yet
- Wissow 2017Document20 pagesWissow 2017Mhd. izzan naserNo ratings yet
- At Mod 3 InfoDocument119 pagesAt Mod 3 InfoDave KokNo ratings yet
- Dissertation On Community Health NursingDocument6 pagesDissertation On Community Health NursingBuyCollegePapersClearwater100% (1)
- Thesis Hospital AdministrationDocument8 pagesThesis Hospital Administrationjanaclarkbillings100% (1)
- A Concept Analysis On Patient-Centered Care: BSN 1 - D Submitted To: Mrs. Marianne G. SoteloDocument15 pagesA Concept Analysis On Patient-Centered Care: BSN 1 - D Submitted To: Mrs. Marianne G. SoteloJan Karl PreciosoNo ratings yet
- Care Map FinalDocument18 pagesCare Map Finalapi-311540850No ratings yet
- AHA Patient Centered Medical HomeDocument21 pagesAHA Patient Centered Medical Homein678No ratings yet
- Labelle 1978 Nursing AuthorityDocument11 pagesLabelle 1978 Nursing AuthorityAhmad JamaluddinNo ratings yet
- Disease Management (Health)Document6 pagesDisease Management (Health)Gabriela CodinăNo ratings yet
- IdentidadDocument12 pagesIdentidadEdgarsito AyalaNo ratings yet
- Flinders Program Information PaperDocument9 pagesFlinders Program Information PaperIbheenk WMNo ratings yet
- Community Health - Chapter 2Document21 pagesCommunity Health - Chapter 2Kyla MoretoNo ratings yet
- Person Centered Care Literature ReviewDocument4 pagesPerson Centered Care Literature Reviewafdtaeczo100% (1)
- Self-Management, Patient Activation and Health Literacy: Section 5Document14 pagesSelf-Management, Patient Activation and Health Literacy: Section 5Andrew WongNo ratings yet
- What Is Person-Centred Health Care A Literature ReviewDocument4 pagesWhat Is Person-Centred Health Care A Literature ReviewcmppcmwgfNo ratings yet
- Copy 1Document5 pagesCopy 1Abdullah SakhiNo ratings yet
- NRES Thesis - Chapter 1 3Y3-7Document16 pagesNRES Thesis - Chapter 1 3Y3-7acorpuz_4No ratings yet
- Understanding The Nursing ProcessDocument7 pagesUnderstanding The Nursing ProcessAbdul HakeemNo ratings yet
- Literature Review Developing Competencies For Health Promotion Deliverable 3bDocument10 pagesLiterature Review Developing Competencies For Health Promotion Deliverable 3bxfeivdsifNo ratings yet
- 2019 LeapfrogToValue PDFDocument57 pages2019 LeapfrogToValue PDFJamey DAVIDSONNo ratings yet
- Hospital Administration Research PapersDocument6 pagesHospital Administration Research Papersafmcbmoag100% (1)
- Meeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformFrom EverandMeeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformAmy S. KelleyNo ratings yet
- Declaration of Vienna ArticleDocument6 pagesDeclaration of Vienna ArticleDwi SurantoNo ratings yet
- tmpDA48 TMPDocument6 pagestmpDA48 TMPFrontiersNo ratings yet
- Osborne+et+al +the+health+education+impact+questionnaireDocument10 pagesOsborne+et+al +the+health+education+impact+questionnairesandrine.abellarNo ratings yet
- Jurnal Retensi 2Document20 pagesJurnal Retensi 2tasyaNo ratings yet
- Theories to Inform Superior Health Informatics Research and PracticeFrom EverandTheories to Inform Superior Health Informatics Research and PracticeNo ratings yet
- Team Base Research (Assignment)Document3 pagesTeam Base Research (Assignment)Frank IbiokNo ratings yet
- Thesis Related To Community Health NursingDocument8 pagesThesis Related To Community Health Nursingtfwysnikd100% (1)
- Case ManagementDocument7 pagesCase ManagementDev RNo ratings yet
- Elements of Effective Palliative Care Models: A Rapid ReviewDocument22 pagesElements of Effective Palliative Care Models: A Rapid ReviewInggrit SuniNo ratings yet
- Dr. MohammedDocument1 pageDr. MohammedSatya Putra LencanaNo ratings yet
- Abstrak EnglishDocument1 pageAbstrak EnglishSatya Putra LencanaNo ratings yet
- Abstrak EnglishDocument1 pageAbstrak EnglishSatya Putra LencanaNo ratings yet
- Effect of Counseling Demonstration and Lecture Method On The Level of Knowledge in Breast Care About Postpartum at Rsud Kota SalatigaDocument1 pageEffect of Counseling Demonstration and Lecture Method On The Level of Knowledge in Breast Care About Postpartum at Rsud Kota SalatigaSatya Putra LencanaNo ratings yet
- Dosen Pembimbing: Abas Lukman Alfiandi M11.01.0001Document1 pageDosen Pembimbing: Abas Lukman Alfiandi M11.01.0001Satya Putra LencanaNo ratings yet
- Hubungan Persalinan Kala I Memanjang Dengan Kesejahteraan JaninDocument6 pagesHubungan Persalinan Kala I Memanjang Dengan Kesejahteraan JaninSatya Putra LencanaNo ratings yet
- Not Angka Just Give Me A ReasonDocument2 pagesNot Angka Just Give Me A ReasonAshaNo ratings yet
- Harapanku Berhenti Pada DirimuDocument3 pagesHarapanku Berhenti Pada DirimuSatya Putra LencanaNo ratings yet
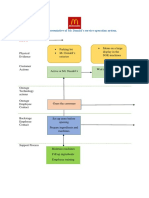
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocument2 pagesBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênNo ratings yet
- Arsenal Strength Catalog 6.2-1Document41 pagesArsenal Strength Catalog 6.2-1Mohammed NavedNo ratings yet
- Topic of Assignment: Health Wellness and Yoga AssignmentDocument12 pagesTopic of Assignment: Health Wellness and Yoga AssignmentHarsh XNo ratings yet
- Report in Per Dev CorrectedDocument34 pagesReport in Per Dev CorrectedJosh lyan RiveraNo ratings yet
- Project Management A Technicians Guide Staples TOCDocument5 pagesProject Management A Technicians Guide Staples TOCAnonymous NwnJNO0% (3)
- 'Bubble Kid' Success Puts Gene Therapy Back On TrackDocument5 pages'Bubble Kid' Success Puts Gene Therapy Back On TrackAbby Grey Lopez100% (1)
- EIL Document On Motor, PanelDocument62 pagesEIL Document On Motor, PanelArindam Samanta100% (1)
- Health Promotion Officers - CPD Booklet Schedule PDFDocument5 pagesHealth Promotion Officers - CPD Booklet Schedule PDFcharles KadzongaukamaNo ratings yet
- Birding The Gulf Stream: Inside This IssueDocument5 pagesBirding The Gulf Stream: Inside This IssueChoctawhatchee Audubon SocietyNo ratings yet
- VPD RashchrtDocument2 pagesVPD RashchrtMarco Ramos JacobNo ratings yet
- Sustainable Development at British Petroleum: Presented by Amardeep Kulshrestha 09BS0000172 Section-EDocument20 pagesSustainable Development at British Petroleum: Presented by Amardeep Kulshrestha 09BS0000172 Section-EAmar KulshresthaNo ratings yet
- Unit 8 Packet KeyDocument21 pagesUnit 8 Packet KeyHiddenNo ratings yet
- Pip-Elsmt01 P66 Midstream Projects 0 1/02/18: Document Number S & B Job Number Rev Date SheetDocument11 pagesPip-Elsmt01 P66 Midstream Projects 0 1/02/18: Document Number S & B Job Number Rev Date SheetAjay BaggaNo ratings yet
- 10 2005 Dec QDocument6 pages10 2005 Dec Qspinster40% (1)
- BMJ 40 13Document8 pagesBMJ 40 13Alvin JiwonoNo ratings yet
- Sample SWMSDocument4 pagesSample SWMSJuma KavesuNo ratings yet
- Neuro M Summary NotesDocument4 pagesNeuro M Summary NotesNishikaNo ratings yet
- Answers To Your Questions About Circumcision and HIV/AIDSDocument2 pagesAnswers To Your Questions About Circumcision and HIV/AIDSAlex BrownNo ratings yet
- PolydactylyDocument43 pagesPolydactylyWara Samsarga GedeNo ratings yet
- Benzil PDFDocument5 pagesBenzil PDFAijaz NawazNo ratings yet
- Penilaian Akhir TahunDocument4 pagesPenilaian Akhir TahunRestu Suci UtamiNo ratings yet
- Guides To The Freshwater Invertebrates of Southern Africa Volume 2 - Crustacea IDocument136 pagesGuides To The Freshwater Invertebrates of Southern Africa Volume 2 - Crustacea IdaggaboomNo ratings yet
- Mushrooms and Religion: Amanita MuscariaDocument8 pagesMushrooms and Religion: Amanita MuscariaGummyCola50% (2)
- Scope: Procter and GambleDocument30 pagesScope: Procter and GambleIrshad AhamedNo ratings yet
- High Speed DoorsDocument64 pagesHigh Speed DoorsVadimMedooffNo ratings yet
- Food Processing NC II - SAGDocument4 pagesFood Processing NC II - SAGNylmazdahr Sañeud DammahomNo ratings yet
- General Chemistry 2 Quarter 4 - Week 4 Module 4: PH of Buffer SolutionsDocument12 pagesGeneral Chemistry 2 Quarter 4 - Week 4 Module 4: PH of Buffer SolutionsHazel EncarnacionNo ratings yet
- Neopuff PDFDocument4 pagesNeopuff PDFoechimNo ratings yet
- Pioneer PDP 5071 5070pu Arp 3354Document219 pagesPioneer PDP 5071 5070pu Arp 3354Dan Prewitt100% (1)
- Engineering Project ListDocument25 pagesEngineering Project ListSyed ShaNo ratings yet