You might also like
- Watson and Raynor 1920Document9 pagesWatson and Raynor 1920ShaneLee10267% (3)
- Complete Storm of Vengeance Campaign PackDocument32 pagesComplete Storm of Vengeance Campaign PackLucas Zocco100% (1)
- Janis Feshbach (1953)Document15 pagesJanis Feshbach (1953)ShaneLee102No ratings yet
- Albert Bandura - Self-Efficacy - Toward A Unifying Theory of Behavioral Change 1977Document25 pagesAlbert Bandura - Self-Efficacy - Toward A Unifying Theory of Behavioral Change 1977Indrajaya KusnidaNo ratings yet
- ASCH - Opinions and Social PressureDocument8 pagesASCH - Opinions and Social PressureEaN100% (1)
- Hazelwood and Douglas (1980)Document6 pagesHazelwood and Douglas (1980)ShaneLee102No ratings yet
- Gillis Nafekh (2005)Document5 pagesGillis Nafekh (2005)ShaneLee102No ratings yet
- Advancing Knowledge About Co-Offending: Results From A Prospective Longitudinal Survey of London Males - Farrington Et Al., (1994)Document680 pagesAdvancing Knowledge About Co-Offending: Results From A Prospective Longitudinal Survey of London Males - Farrington Et Al., (1994)ShaneLee102No ratings yet
- Psych ReviewerDocument4 pagesPsych ReviewerAudrey AngNo ratings yet
- Proceedings of The Society For Medieval Logic & Metaphysics 3Document81 pagesProceedings of The Society For Medieval Logic & Metaphysics 3MeatredNo ratings yet
- Does Treatment of Subsyndromal Depression Improve Depression and Diabetes Related OutcomesDocument9 pagesDoes Treatment of Subsyndromal Depression Improve Depression and Diabetes Related OutcomesRenato ObregónNo ratings yet
- 2015 Article 118Document14 pages2015 Article 118Denisse DelgadoNo ratings yet
- Diabetes and DepresiDocument218 pagesDiabetes and DepresiDaslan ToruntjuNo ratings yet
- 1 PDFDocument8 pages1 PDFsufaNo ratings yet
- Jurnal Proposal 5Document5 pagesJurnal Proposal 5ArjunaPamungkasNo ratings yet
- ST2 1.1.3 Noroozi, Et Al. 2017Document7 pagesST2 1.1.3 Noroozi, Et Al. 2017JemarcusNo ratings yet
- Impaired Glucose Homeostasis in First-Episode Schizophrenia A Systematic Review and Meta-AnalysisDocument9 pagesImpaired Glucose Homeostasis in First-Episode Schizophrenia A Systematic Review and Meta-AnalysistatanmenaNo ratings yet
- Shalini Chawla, Nitin Kaushik, Narinder Pal Singh, Raktim Ghosh, Alpana SaxenaDocument41 pagesShalini Chawla, Nitin Kaushik, Narinder Pal Singh, Raktim Ghosh, Alpana Saxena88AKKNo ratings yet
- HUang, 2008 D-39Document12 pagesHUang, 2008 D-39Fadel TrianzahNo ratings yet
- Ass Knowledge and MaDocument1 pageAss Knowledge and MaB04-BALKIS SOLEHAHNo ratings yet
- Efficacy of Lifestyle Interventions in Patients With Type 2 Diabetes - A Systematic Review and Meta-AnalysisDocument11 pagesEfficacy of Lifestyle Interventions in Patients With Type 2 Diabetes - A Systematic Review and Meta-AnalysisDara Agusti MaulidyaNo ratings yet
- Nelson, 2011Document8 pagesNelson, 2011Silvinha LunaNo ratings yet
- Agnes Nogueira Gossenheimer The Power of The PlaceboDocument8 pagesAgnes Nogueira Gossenheimer The Power of The PlacebosoylahijadeunvampiroNo ratings yet
- Prevention of Recurrent Depression With Cognitive Behavioral TherapyDocument13 pagesPrevention of Recurrent Depression With Cognitive Behavioral TherapyImuzz Al GhassanNo ratings yet
- Depressive Symptoms in Patients With Subclinical Hypothyroidism The Effect of Treatment With Levothyroxine A Double Blind Randomized Clinical TrialDocument6 pagesDepressive Symptoms in Patients With Subclinical Hypothyroidism The Effect of Treatment With Levothyroxine A Double Blind Randomized Clinical TrialastrogliaNo ratings yet
- 25 OS OD: Progression of Diabetic Retinopathy in The Hypertension Intervention Nurse Telemedicine StudyDocument2 pages25 OS OD: Progression of Diabetic Retinopathy in The Hypertension Intervention Nurse Telemedicine Studyanisarahma718No ratings yet
- Weight Loss Within First 2 Years of Treating Type 2 Diabetes Associated With RemissionDocument3 pagesWeight Loss Within First 2 Years of Treating Type 2 Diabetes Associated With RemissionManoj KumarNo ratings yet
- Patient Education and CounselingDocument6 pagesPatient Education and CounselingriadesnitaNo ratings yet
- Psychological Family Intervention For Poorly Controlled Type 2 DiabetesDocument7 pagesPsychological Family Intervention For Poorly Controlled Type 2 Diabetesluhseriastuti12No ratings yet
- Research Article: The Effect of Antidepressants On The Course of Inflammatory Bowel DiseaseDocument11 pagesResearch Article: The Effect of Antidepressants On The Course of Inflammatory Bowel DiseaseSangeeta BSRNo ratings yet
- Vilazodona GadDocument15 pagesVilazodona GadPablo FerrariNo ratings yet
- Bismillah Fix Hba1c3Document8 pagesBismillah Fix Hba1c3NsafifahNo ratings yet
- Yùquán WānDocument14 pagesYùquán Wānmiguelzhuangzi09No ratings yet
- TreatmentDocument3 pagesTreatmentAdriana RivettiNo ratings yet
- jmcp.2016.22.5.493 RupDocument23 pagesjmcp.2016.22.5.493 RupadninaninNo ratings yet
- Treatment of Bipolar DisorderDocument20 pagesTreatment of Bipolar DisorderShana Wl100% (1)
- Diabetic Medicine - 2017 - Perrin - The Prevalence of Diabetes Specific Emotional Distress in People With Type 2 DiabetesDocument13 pagesDiabetic Medicine - 2017 - Perrin - The Prevalence of Diabetes Specific Emotional Distress in People With Type 2 Diabetesnirmala amirNo ratings yet
- A Randomized Controlled Trial of Medication and Cognitive-Behavioral Therapy For HypochondriasisDocument9 pagesA Randomized Controlled Trial of Medication and Cognitive-Behavioral Therapy For HypochondriasisDewina Dyani Rosari IINo ratings yet
- Implications of The United Kingdom Prospective Diabetes StudyDocument5 pagesImplications of The United Kingdom Prospective Diabetes StudyAgustin MendezNo ratings yet
- Hypertension Article 1997Document9 pagesHypertension Article 1997iqra uroojNo ratings yet
- Alasan Ke ManusiaDocument12 pagesAlasan Ke ManusiaafiwahyuNo ratings yet
- Checklist DRPDocument16 pagesChecklist DRPPutri Kusuma WardaniNo ratings yet
- With Type 2 Diabetes: - Glucosidase Inhibitors For PatientsDocument10 pagesWith Type 2 Diabetes: - Glucosidase Inhibitors For PatientsNyayu Fitriani MuttaqienNo ratings yet
- Al Shehri 2008Document10 pagesAl Shehri 2008Dewi MaryamNo ratings yet
- Schmitt Et Al jpr2017 Depression-Related HyperglycaemiaDocument7 pagesSchmitt Et Al jpr2017 Depression-Related HyperglycaemiaTiToNo ratings yet
- Articulo Dislipidemias 2Document18 pagesArticulo Dislipidemias 2DANIELA CALDERON SAGAHONNo ratings yet
- Prevalence and Severity of DepressionDocument8 pagesPrevalence and Severity of DepressionWaheedullah AhmadiNo ratings yet
- Exercise For Type 2 Diabetes Mellitus - PubMed HealthDocument2 pagesExercise For Type 2 Diabetes Mellitus - PubMed Healthdr_zegarraNo ratings yet
- The Diabetes Self-Management QuestionnaireDocument14 pagesThe Diabetes Self-Management QuestionnaireRatna Nur ApitasariNo ratings yet
- Effect of Traditional Medicines On Diabetes Treatment: A Meta-AnalysisDocument14 pagesEffect of Traditional Medicines On Diabetes Treatment: A Meta-Analysisijmb333No ratings yet
- ESMON Study ArticleDocument7 pagesESMON Study ArticleAhmedaref EzrinNo ratings yet
- Efficacy and Safety of Initial Combination Therapy in Treatment-Naı Ve Type 2 Diabetes Patients: A Systematic Review and Meta-AnalysisDocument20 pagesEfficacy and Safety of Initial Combination Therapy in Treatment-Naı Ve Type 2 Diabetes Patients: A Systematic Review and Meta-AnalysisLyka MahrNo ratings yet
- A Case of Haemochromatosis and Diabetes A Missed OpportunityDocument111 pagesA Case of Haemochromatosis and Diabetes A Missed Opportunitymimran1974No ratings yet
- Proton-Pump Inhibitors Therapy and Blood Pressure ControlDocument6 pagesProton-Pump Inhibitors Therapy and Blood Pressure ControlTeky WidyariniNo ratings yet
- ManiaDocument2 pagesManiajopet8180No ratings yet
- Metabolic StressDocument3 pagesMetabolic StressRoberto MartineNo ratings yet
- Heijden2013 Article EffectsOfExerciseTrainingOnQuaDocument16 pagesHeijden2013 Article EffectsOfExerciseTrainingOnQuaALberta YosheNo ratings yet
- Quality Improvement Project.Document7 pagesQuality Improvement Project.rhinoNo ratings yet
- ANNALS-Diabetes Tipo IIDocument16 pagesANNALS-Diabetes Tipo IIewb100% (2)
- Health and Quality of Life OutcomesDocument11 pagesHealth and Quality of Life OutcomesAoikiji KuzanNo ratings yet
- Health Locus of Control and Diabetes Adherence 2161 0487.S3 E002Document2 pagesHealth Locus of Control and Diabetes Adherence 2161 0487.S3 E002iulianaNo ratings yet
- Characteristics of Depression in Hemodialysis Patients: Symptoms, Quality of Life and Mortality RiskDocument7 pagesCharacteristics of Depression in Hemodialysis Patients: Symptoms, Quality of Life and Mortality RiskMirza RisqaNo ratings yet
- Stress Management Improves Long-Term Glycemic Control in Type 2 DiabetesDocument5 pagesStress Management Improves Long-Term Glycemic Control in Type 2 DiabetesRodel SumiranNo ratings yet
- Journal of Psychosomatic ResearchDocument6 pagesJournal of Psychosomatic ResearchAryaldy ZulkarnainiNo ratings yet
- ADA - UKPD StudyDocument5 pagesADA - UKPD StudyMagdalena MercyanaNo ratings yet
- Dia Care 2002 Pastors 608 13Document6 pagesDia Care 2002 Pastors 608 13Isnar Nurul AlfiyahNo ratings yet
- My Nature CureDocument16 pagesMy Nature Curehemraj.koiralaNo ratings yet
- A Randomized, Double-Blind, Placebo-Controlled Trial of Quetiapine in The Treatment of Bipolar I or II DepressionDocument10 pagesA Randomized, Double-Blind, Placebo-Controlled Trial of Quetiapine in The Treatment of Bipolar I or II DepressionSyifa FadyaNo ratings yet
- Diabetes Risks from Prescription and Nonprescription Drugs: Mechanisms and Approaches to Risk ReductionFrom EverandDiabetes Risks from Prescription and Nonprescription Drugs: Mechanisms and Approaches to Risk ReductionNo ratings yet
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionFrom EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionNo ratings yet
- Pubhealthrep00142 0062Document10 pagesPubhealthrep00142 0062chakri1089No ratings yet
- Kanner (1981)Document39 pagesKanner (1981)ShaneLee1020% (1)
- Effects of Physical Attractiveness of The Plaintiff and Defendant in Sexual Harassment JudgmentsDocument16 pagesEffects of Physical Attractiveness of The Plaintiff and Defendant in Sexual Harassment JudgmentsShaneLee102No ratings yet
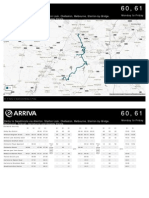
- Derby To Swadlincote Via Allenton, Shelton Lock, Chellaston, Melbourne, Stanton-by-Bridge, Melbourne, Ticknall, Hartshorne and Goseley EstateDocument7 pagesDerby To Swadlincote Via Allenton, Shelton Lock, Chellaston, Melbourne, Stanton-by-Bridge, Melbourne, Ticknall, Hartshorne and Goseley EstateShaneLee102No ratings yet
- Derby To Swadlincote Via Allenton, Shelton Lock, Chellaston, Melbourne, Stanton-by-Bridge, Melbourne, Ticknall, Hartshorne and Goseley EstateDocument3 pagesDerby To Swadlincote Via Allenton, Shelton Lock, Chellaston, Melbourne, Stanton-by-Bridge, Melbourne, Ticknall, Hartshorne and Goseley EstateShaneLee102No ratings yet
- Canter Et Al (2004)Document48 pagesCanter Et Al (2004)ShaneLee102100% (2)
- Mann Et Al 2004Document42 pagesMann Et Al 2004ShaneLee102No ratings yet
- Main Stops Monday To Friday 60 61Document7 pagesMain Stops Monday To Friday 60 61ShaneLee102No ratings yet
- McCloskey Wible Cohen (1988)Document11 pagesMcCloskey Wible Cohen (1988)ShaneLee102No ratings yet
- Bioscience Horizons 2011 Webber 165 73Document9 pagesBioscience Horizons 2011 Webber 165 73ShaneLee102No ratings yet
- Difference Between Transactional and Transformational LeadershipDocument4 pagesDifference Between Transactional and Transformational LeadershipReen Zaza Zareen100% (1)
- ExampleApp Functional SpecificationDocument119 pagesExampleApp Functional SpecificationmilosvarakNo ratings yet
- Erotic CultDocument6 pagesErotic Cultmallikai_1No ratings yet
- Sport, Race and Ethnicity: Coakley CHP 9Document16 pagesSport, Race and Ethnicity: Coakley CHP 9Arief MoertopoNo ratings yet
- Literature Review: Pengaruh Pendidikan Kesehatan Menggunakan Media Audiovisual Tentang Menarche Terhadap Kesiapan Siswi SD Menghadapi MenarcheDocument10 pagesLiterature Review: Pengaruh Pendidikan Kesehatan Menggunakan Media Audiovisual Tentang Menarche Terhadap Kesiapan Siswi SD Menghadapi Menarcheangghi oktavianiNo ratings yet
- Paraphrasing ExercisesDocument4 pagesParaphrasing ExercisesPaulinaNo ratings yet
- Neural AssignmentDocument76 pagesNeural AssignmentMustaQeem AhmadNo ratings yet
- Critiques of Mixed Methods Research StudiesDocument18 pagesCritiques of Mixed Methods Research Studiesmysales100% (1)
- Huge Land Swap OK'd: Seattle Post-IntelligencerDocument3 pagesHuge Land Swap OK'd: Seattle Post-IntelligencerCCWebClientsNo ratings yet
- Expert Guide To Cognos Audit DataDocument30 pagesExpert Guide To Cognos Audit Dataleonardo russoNo ratings yet
- Joseph Cote WeeblyDocument2 pagesJoseph Cote Weeblyapi-232220181No ratings yet
- 50 Affirmations For A Fertile Mind, Heart & SoulDocument104 pages50 Affirmations For A Fertile Mind, Heart & SoulKarishma SethNo ratings yet
- Unit 4 Review Worksheet APDocument12 pagesUnit 4 Review Worksheet APphantomofthekeysNo ratings yet
- Eng9 Q1mod7 Communicative Styles Geraldine Sumipit Bgo For UploadingDocument25 pagesEng9 Q1mod7 Communicative Styles Geraldine Sumipit Bgo For UploadingJeni Liangna100% (1)
- 022482-2508a Sps855 Gnss Modular Receiver Ds 0513 LRDocument2 pages022482-2508a Sps855 Gnss Modular Receiver Ds 0513 LRJames Earl CubillasNo ratings yet
- Venue and Timetabling Details Form: Simmonsralph@yahoo - Co.inDocument3 pagesVenue and Timetabling Details Form: Simmonsralph@yahoo - Co.inCentre Exam Manager VoiceNo ratings yet
- Chap R SMDocument50 pagesChap R SMElisabeteNo ratings yet
- An Introduction To Genre Theory: January 1997Document16 pagesAn Introduction To Genre Theory: January 1997pratolectusNo ratings yet
- Studio D A1 WorkbookDocument4 pagesStudio D A1 WorkbookZubyr Bhatty0% (1)
- Bit Sub and Float ChartDocument16 pagesBit Sub and Float ChartRobert KilgoreNo ratings yet
- Specific Volume, M /KG Internal Energy, KJ/KG Temp. Press. Sat. Liquid Evap. Sat. Vapor Sat. Liquid Evap. Sat. Vapor (C) (Kpa)Document6 pagesSpecific Volume, M /KG Internal Energy, KJ/KG Temp. Press. Sat. Liquid Evap. Sat. Vapor Sat. Liquid Evap. Sat. Vapor (C) (Kpa)sidhartha dasNo ratings yet
- BS en 00246-2003Document20 pagesBS en 00246-2003Shan Sandaruwan AbeywardeneNo ratings yet
- Beyond GrammarDocument184 pagesBeyond Grammaryazadn100% (2)
- (YDM) Ambo University Phy ExamDocument8 pages(YDM) Ambo University Phy ExamYdm DmaNo ratings yet
- ADMINLAW1Document67 pagesADMINLAW1FeEdithOronicoNo ratings yet
- U KH51 Kubota D950-BH (1987-1991)Document3 pagesU KH51 Kubota D950-BH (1987-1991)Joe StadlerNo ratings yet
- Things Go Bump in The Night Case StudyDocument5 pagesThings Go Bump in The Night Case StudyShelton D'mello100% (1)