You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ashton Manual English PDFDocument58 pagesAshton Manual English PDFMalissa Bowen100% (2)
- Adolescentes BFM HyperCVAD Alacacioglu2015Document5 pagesAdolescentes BFM HyperCVAD Alacacioglu2015erickmattosNo ratings yet
- BFM 2009 Colombia 0120-0011-Rfmun-64-03-00417Document9 pagesBFM 2009 Colombia 0120-0011-Rfmun-64-03-00417erickmattosNo ratings yet
- LMA BFM 2004 1-S2.0-S0006497119422519-MainDocument3 pagesLMA BFM 2004 1-S2.0-S0006497119422519-MainerickmattosNo ratings yet
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author ManuscripterickmattosNo ratings yet
- Navy Heritage Video: General Military Training-Drug and Alcohol Abuse 1-2-1Document63 pagesNavy Heritage Video: General Military Training-Drug and Alcohol Abuse 1-2-1Kallepalli Somalingeswara RaoNo ratings yet
- Drug Scenario in The PhilippinesDocument15 pagesDrug Scenario in The PhilippinesCalix GonzalesNo ratings yet
- Pre-Filled Syringes 2014-2024 PDFDocument24 pagesPre-Filled Syringes 2014-2024 PDFVisiongainGlobal0% (1)
- Pharmaceutical Jurisprudence Sessional November 21 BP-505TDocument4 pagesPharmaceutical Jurisprudence Sessional November 21 BP-505TLloyd Institute of Management & Technology Pharm.No ratings yet
- TamsulosinDocument27 pagesTamsulosinAnna WidiaNo ratings yet
- Opioids For Acute Pancreatitis Pain (Review) : Basurto Ona X, Rigau Comas D, Urrútia GDocument49 pagesOpioids For Acute Pancreatitis Pain (Review) : Basurto Ona X, Rigau Comas D, Urrútia GYave Aro RodriguezNo ratings yet
- SYDocument54 pagesSYDimos MastroNo ratings yet
- Tapering BenzodiazepinesDocument3 pagesTapering BenzodiazepineslgiuzfgukuzfglufzNo ratings yet
- EvalGrants Letrozole Case Study Report FINALDocument66 pagesEvalGrants Letrozole Case Study Report FINALKanav GuptaNo ratings yet
- HPLC Calculation SpreadsheetDocument2 pagesHPLC Calculation SpreadsheetUmer Al-FaisalNo ratings yet
- Pharma Parenteral Dosage CalculationDocument3 pagesPharma Parenteral Dosage CalculationMaxinne RoseñoNo ratings yet
- Drugs 3Document43 pagesDrugs 3IonuțHerpeșNo ratings yet
- PCOL Maps PDFDocument11 pagesPCOL Maps PDFZinc YuloNo ratings yet
- Drugs in Ovulation InductionDocument8 pagesDrugs in Ovulation InductionJeevs Music100% (1)
- Bspha C1 Las 1Document41 pagesBspha C1 Las 1Muhammad Haroon RazaNo ratings yet
- SS II.1.1 Update On Typhoid Management - Dr. Adityo Susilo, SpPD-KPTI PDFDocument34 pagesSS II.1.1 Update On Typhoid Management - Dr. Adityo Susilo, SpPD-KPTI PDFWisnu Yudho HNo ratings yet
- PHARMACEUTICAL PLANT DESIGN ACCORDING TO CGMP GUIDELINESDocument12 pagesPHARMACEUTICAL PLANT DESIGN ACCORDING TO CGMP GUIDELINESRezwan Ahmed MahediNo ratings yet
- CLSI Pak-Antibiotic Sensitivity Panels Feb 2017-NasrullahDocument18 pagesCLSI Pak-Antibiotic Sensitivity Panels Feb 2017-NasrullahIhtisham Ul HaqNo ratings yet
- DrugsDocument155 pagesDrugsAkankshaNo ratings yet
- Accidental Epidural Injection of Atropine: Case ReportDocument2 pagesAccidental Epidural Injection of Atropine: Case ReportAida TantriNo ratings yet
- DIURETICSDocument40 pagesDIURETICSNiña Jean Tormis AldabaNo ratings yet
- Grandi 2019. Hormonal Contraception in Women With Endometriosis - A Systematic ReviewDocument11 pagesGrandi 2019. Hormonal Contraception in Women With Endometriosis - A Systematic ReviewcespersiNo ratings yet
- NPDS2011Document254 pagesNPDS2011A JWNo ratings yet
- Drug SheetDocument3 pagesDrug Sheetavause2No ratings yet
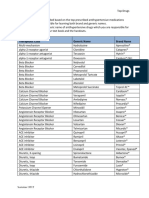
- Top Antihypertensive Drugs Generic-Brand Names PDFDocument1 pageTop Antihypertensive Drugs Generic-Brand Names PDFvidbala0% (1)
- Anticancer DrugDocument29 pagesAnticancer DrugAnjana PaudelNo ratings yet
- Final Drug StudyDocument4 pagesFinal Drug StudyBasema HashhashNo ratings yet
- Azithromycin (Zithromycin)Document2 pagesAzithromycin (Zithromycin)Adrianne Bazo100% (1)
- Part No Product Name Location Batch No Expired Date QTY OnhandDocument6 pagesPart No Product Name Location Batch No Expired Date QTY OnhandRatih SafrianiNo ratings yet