You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Chapter 8: Multiple and Logistic Regression Learning ObjectivesDocument3 pagesChapter 8: Multiple and Logistic Regression Learning Objectivesrodicasept1967No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Data Mining - Lab 7 Using Weka For ClusteringDocument9 pagesData Mining - Lab 7 Using Weka For Clusteringrodicasept1967No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Fingolimoid - 2014Document9 pagesFingolimoid - 2014rodicasept1967No ratings yet
- MNJMNJDocument1 pageMNJMNJrodicasept1967No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Fvghgbhjghjyuhjnhyuufghgbnjkm,, HB JB HJBN M BGCFVB VV B J N Kmdjsa Lkdi LX - KMCJKN .Xmcc. BBHBNBHBNJDocument1 pageFvghgbhjghjyuhjnhyuufghgbnjkm,, HB JB HJBN M BGCFVB VV B J N Kmdjsa Lkdi LX - KMCJKN .Xmcc. BBHBNBHBNJrodicasept1967No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Statement of IntentDocument8 pagesStatement of Intentnineteen91No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- GE7-Ethics Module-7Document6 pagesGE7-Ethics Module-7Jess Sy GooNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Safety and Accident Investigation Short Courses 2020Document21 pagesSafety and Accident Investigation Short Courses 2020Jose A. HerreraNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- 96 330 1 PBDocument13 pages96 330 1 PBPredic PlaysNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Fidia Oktarisa, 2023Document14 pagesFidia Oktarisa, 2023AUFA DIAZ CAMARANo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Research On Minimal-Pair DrillsDocument54 pagesResearch On Minimal-Pair DrillsYuri IssangNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Questions About My PapersDocument2 pagesQuestions About My Papersapi-548918153No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Draft of Synopsis AJKUDocument19 pagesDraft of Synopsis AJKUMasood ur Rehman Khan100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Fingerprint and Face Recognition System Using A Feed-Forward Artificial Neural Network ParadigmDocument12 pagesFingerprint and Face Recognition System Using A Feed-Forward Artificial Neural Network ParadigmInternational Journal of Innovative Science and Research TechnologyNo ratings yet
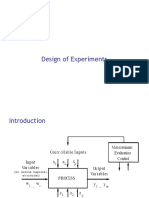
- Design of ExperimentDocument49 pagesDesign of ExperimentMuhammad Insan KamilNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Methods of Research-Lession 4Document57 pagesMethods of Research-Lession 4Renj LoiseNo ratings yet
- MPT CvtsDocument42 pagesMPT CvtsSudarshan100% (1)
- The Scanlon Plan Involved Two SystemsDocument3 pagesThe Scanlon Plan Involved Two SystemsJehanzeb SiddiquiNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Module in Elementary Statistics and Probability With LaboratoryDocument15 pagesModule in Elementary Statistics and Probability With LaboratoryMonec JalandoniNo ratings yet
- E-Tech Q3 Module4Document23 pagesE-Tech Q3 Module4Ebb Tenebroso JudillaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Conception of A Manual Brick Machine PDFDocument57 pagesConception of A Manual Brick Machine PDFamanuel admasuNo ratings yet
- BullyingDocument19 pagesBullyingPia SottoNo ratings yet
- Data Inspection Using BiplotDocument16 pagesData Inspection Using BiplotNadya NovitaNo ratings yet
- Summer Internship ProjectDocument70 pagesSummer Internship ProjectNitin SahniNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Baby Thesis Title SampleDocument5 pagesBaby Thesis Title Samplezpxoymief100% (1)
- Design of Experiments, Principles and ApplicationsDocument350 pagesDesign of Experiments, Principles and ApplicationsJamille Vargas100% (1)
- Pengaruh Kompetensi Terhadap Kinerja Pegawai Pada Dinas Perhubungan, Komunikasi Dan Informatika Kabupaten Mamuju UtaraDocument9 pagesPengaruh Kompetensi Terhadap Kinerja Pegawai Pada Dinas Perhubungan, Komunikasi Dan Informatika Kabupaten Mamuju UtaraEricson SembiringNo ratings yet
- Multicategory Logit ModelsDocument49 pagesMulticategory Logit ModelsRegine del RosarioNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Political Cycle - Alberto AlesinaDocument3 pagesPolitical Cycle - Alberto AlesinayumicintaNo ratings yet
- Patient Satisfaction and Benefts of Music Therapy Services To Manage Stress and Pain in The Hospital Emergency DepartmentDocument25 pagesPatient Satisfaction and Benefts of Music Therapy Services To Manage Stress and Pain in The Hospital Emergency DepartmentBapak Sunaryo SPBU100% (1)
- Concrete Canoe Using Light Weight Aggregate: Ab Ul Saleem .K, Prashob C, Sooraj M, Mohamme NishamDocument4 pagesConcrete Canoe Using Light Weight Aggregate: Ab Ul Saleem .K, Prashob C, Sooraj M, Mohamme NishamHARISHMA RAVEENDRANNo ratings yet
- Vapor Corrosion Inhibitors For Tank Bottom Corrosion Control - Pavan K Shukla, Jerry DewittDocument12 pagesVapor Corrosion Inhibitors For Tank Bottom Corrosion Control - Pavan K Shukla, Jerry DewittmindbagNo ratings yet
- Pie DiabeticoDocument7 pagesPie DiabeticoMauro Adrianzen HernaniNo ratings yet
- Building Demand and Supply For Evaluation in Africa Vol 1 PDFDocument80 pagesBuilding Demand and Supply For Evaluation in Africa Vol 1 PDFMakhue KhumzzNo ratings yet
- 343snowdenl Essay3Document5 pages343snowdenl Essay3api-414035660No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)