You might also like
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Burn Stabilization ProtocolDocument2 pagesBurn Stabilization ProtocolAli AftabNo ratings yet
- Abg Made EasyDocument24 pagesAbg Made EasynbvillarazoNo ratings yet
- Head To Toe Physical Assessment: College of NursingDocument4 pagesHead To Toe Physical Assessment: College of NursingMaicah ShaneNo ratings yet
- ABGDocument2 pagesABGSharon V. Guevara-AntonioNo ratings yet
- MedicalSurgical Nursing ReviewDocument86 pagesMedicalSurgical Nursing ReviewPopa D. SilviuNo ratings yet
- Jennifer Portillo Health Assessment VocabularyDocument9 pagesJennifer Portillo Health Assessment VocabularyJennifer PortilloNo ratings yet
- ABG InterpretationDocument11 pagesABG InterpretationertrggerNo ratings yet
- Renal & Urinary ATIDocument2 pagesRenal & Urinary ATIHelen Varela100% (1)
- What Is Respiratory Alkalosis?Document3 pagesWhat Is Respiratory Alkalosis?Lorenn AdarnaNo ratings yet
- Percentage BMI calculator helps determine patient weight statusDocument36 pagesPercentage BMI calculator helps determine patient weight statuskasonde.musonda8No ratings yet
- Q. Write Down The ECG Criteria of AF?: Atrial Fibrillation (D-470)Document5 pagesQ. Write Down The ECG Criteria of AF?: Atrial Fibrillation (D-470)DR.SANJOY GHOSHNo ratings yet
- Cs-Cardiac-023-Essential Cardiac LabsDocument2 pagesCs-Cardiac-023-Essential Cardiac LabsColeen YraolaNo ratings yet
- HESI LPN ADN ENTRANCE EXAM MOBILITY EXAMS A GRADED 100 VERIFIED - pdf-1-33Document33 pagesHESI LPN ADN ENTRANCE EXAM MOBILITY EXAMS A GRADED 100 VERIFIED - pdf-1-33erick kanyiNo ratings yet
- Nursing Care of PlanDocument16 pagesNursing Care of PlanDbyNo ratings yet
- IV PDFDocument63 pagesIV PDFelbagouryNo ratings yet
- Geometry Z PlastyDocument18 pagesGeometry Z PlastyYudi WijayaNo ratings yet
- The Nclex-Pn Cram Sheet: General Test Information Normal Lab ValuesDocument2 pagesThe Nclex-Pn Cram Sheet: General Test Information Normal Lab Valuesroboat96No ratings yet
- Acid Base DisordersDocument5 pagesAcid Base DisordersMillenial VoiceNo ratings yet
- Anti Neoplastic and Immunosupressant DrugsDocument29 pagesAnti Neoplastic and Immunosupressant DrugsAshraf Moby100% (1)
- Concept Map Et Al 11-04-15Document7 pagesConcept Map Et Al 11-04-15api-353656227No ratings yet
- Chapter 08: Injectable Medications Mulholland: The Nurse, The Math, The Meds, 3rd EditionDocument13 pagesChapter 08: Injectable Medications Mulholland: The Nurse, The Math, The Meds, 3rd EditionadenNo ratings yet
- Medical-Surgical Nursing Review: 315 Key ConceptsDocument15 pagesMedical-Surgical Nursing Review: 315 Key ConceptsJap Avila BernasNo ratings yet
- Carpal Tunnel Surgery, Hand Clinics, Volume 18, Issue 2, Pages 211-368 (May 2002)Document151 pagesCarpal Tunnel Surgery, Hand Clinics, Volume 18, Issue 2, Pages 211-368 (May 2002)alinutza_childNo ratings yet
- Check My Twitter Account @nursetopia or IG @nursetopia1 For More Nursing Test Banks, Sample Exam, Reviewers, and NotesDocument5 pagesCheck My Twitter Account @nursetopia or IG @nursetopia1 For More Nursing Test Banks, Sample Exam, Reviewers, and NotesNurse UtopiaNo ratings yet
- Output 1 Electrolytes - DraftDocument16 pagesOutput 1 Electrolytes - Draftallanrnmanaloto100% (1)
- Patient Education for Ileal Conduit CareDocument11 pagesPatient Education for Ileal Conduit CareICa MarlinaNo ratings yet
- IV Lab Practice Problems Answers SP 2013 PALDocument2 pagesIV Lab Practice Problems Answers SP 2013 PALjmraczynskiNo ratings yet
- HTNDocument54 pagesHTNapi-232466940No ratings yet
- Main drug therapy for ulcerative colitis is sulfa for one yearDocument4 pagesMain drug therapy for ulcerative colitis is sulfa for one yearcathyNo ratings yet
- CardiacDocument10 pagesCardiacMarcus Reynolds100% (1)
- MedSurgATI1Document97 pagesMedSurgATI1LeelanRamphal100% (1)
- 1538 Exam 4 Cell Reg & GriefDocument35 pages1538 Exam 4 Cell Reg & GriefJade EdanoNo ratings yet
- TXTDocument356 pagesTXTJec AmracNo ratings yet
- Adams4e Tif Ch23Document25 pagesAdams4e Tif Ch23fbernis1480_11022046No ratings yet
- HESI MED SURG STUDY GUIDE: SHOCKDocument1 pageHESI MED SURG STUDY GUIDE: SHOCKGeorgeNo ratings yet
- Shock Types 141009102815 Conversion Gate01Document41 pagesShock Types 141009102815 Conversion Gate01Samjaisheel SamsonNo ratings yet
- ABG InterpretationDocument10 pagesABG InterpretationNisha MathewNo ratings yet
- Medsurg 2007Document15 pagesMedsurg 2007WisdomIsMisery100% (1)
- Report PDFDocument7 pagesReport PDFBrayla WoolfolkNo ratings yet
- ATI Practice CodesDocument1 pageATI Practice Codesvanassa johnson100% (4)
- The Basics of Ekg: Presented byDocument31 pagesThe Basics of Ekg: Presented bypekpekNo ratings yet
- Paeds Handbook Class2021 1568487638Document30 pagesPaeds Handbook Class2021 1568487638kafosidNo ratings yet
- Chapter 25heart Failure and Inflammatory DysfunctionDocument10 pagesChapter 25heart Failure and Inflammatory DysfunctionNurse UtopiaNo ratings yet
- Lab Values and Vital SignsDocument4 pagesLab Values and Vital SignsWole Olaluwoye100% (1)
- My Cheat SheetDocument3 pagesMy Cheat SheetTenzin KyizomNo ratings yet
- Adams4e Tif Ch38Document19 pagesAdams4e Tif Ch38fbernis1480_11022046No ratings yet
- Pharm Finalspring16 PDFDocument9 pagesPharm Finalspring16 PDFMNo ratings yet
- Quiz 2 Study Guide - SHOCK!!! 25 Questions READ BOOK!!! Know Charts Esp. Stages of Shock ChartDocument1 pageQuiz 2 Study Guide - SHOCK!!! 25 Questions READ BOOK!!! Know Charts Esp. Stages of Shock Chartjenn1722No ratings yet
- Hematology 101: Hematology/Oncology PG 1 of 11Document12 pagesHematology 101: Hematology/Oncology PG 1 of 11esther100% (1)
- Newborn Hal ManualDocument74 pagesNewborn Hal ManualPedz RomanoNo ratings yet
- DRUGS AND DEFIBRILLATION IN CARDIAC ARRESTDocument20 pagesDRUGS AND DEFIBRILLATION IN CARDIAC ARRESTAfrida Sahestina100% (1)
- Care PlanDocument11 pagesCare PlanAlyssa CardinalNo ratings yet
- Drug CalculationsDocument32 pagesDrug CalculationsNisha Vats100% (1)
- Medical Surgical Nursing - DiabetesDocument4 pagesMedical Surgical Nursing - Diabetestripj33100% (2)
- Ch. 1, Lesson 1: What Is The Next Gen NCLEXDocument4 pagesCh. 1, Lesson 1: What Is The Next Gen NCLEXChantelNo ratings yet
- Fundamentals Quizzing TIPSDocument41 pagesFundamentals Quizzing TIPSmelissamichellleNo ratings yet
- How To Mix InsulinDocument2 pagesHow To Mix InsulinchareneadamsNo ratings yet
- King Rush MoreDocument1 pageKing Rush MoreawuahbohNo ratings yet
- Oop Say You Know MeDocument1 pageOop Say You Know MeawuahbohNo ratings yet
- Pharm NclexDocument9 pagesPharm NclexawuahbohNo ratings yet
- Article For CET CHFDocument5 pagesArticle For CET CHFawuahbohNo ratings yet
- Article For JournalDocument6 pagesArticle For JournalawuahbohNo ratings yet
- PolypharmacyDocument24 pagesPolypharmacySurina Zaman HuriNo ratings yet
- HandOff SampleToolsDocument9 pagesHandOff SampleToolsOllie EvansNo ratings yet
- The BSN Job Search: Interview Preparation: Telling Your StoryDocument25 pagesThe BSN Job Search: Interview Preparation: Telling Your StoryawuahbohNo ratings yet
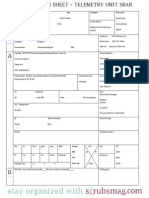
- Nurse Brain Sheet Telemetry Unit SBARDocument1 pageNurse Brain Sheet Telemetry Unit SBARvsosa624No ratings yet
- NCLEX Random FactsDocument34 pagesNCLEX Random FactsLegnaMary100% (8)
- Probability of A or B and A and B-1Document2 pagesProbability of A or B and A and B-1awuahbohNo ratings yet
- Middle Age Adult Health History Assignment Guidelines N315 Fall 2013Document23 pagesMiddle Age Adult Health History Assignment Guidelines N315 Fall 2013awuahbohNo ratings yet
- EBP Article 1Document11 pagesEBP Article 1awuahbohNo ratings yet
- Massachusetts Department of Public HealthDocument24 pagesMassachusetts Department of Public HealthawuahbohNo ratings yet
- Drugs NclexDocument30 pagesDrugs Nclexawuahboh100% (1)
- EBP Article 3Document6 pagesEBP Article 3awuahbohNo ratings yet
- Tips On Answering NclexDocument4 pagesTips On Answering NclexawuahbohNo ratings yet
- Random FactsDocument338 pagesRandom Factscyram81100% (1)
- Critical Thinking StrategiesDocument3 pagesCritical Thinking StrategiesawuahbohNo ratings yet
- Therapeutic CommunicationDocument1 pageTherapeutic CommunicationawuahbohNo ratings yet
- Does Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorDocument24 pagesDoes Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorawuahbohNo ratings yet
- ENT Throat and EsophagusDocument41 pagesENT Throat and EsophagusMUHAMMAD HASAN NAGRANo ratings yet
- Debate 3 Youth Incarceration in Adult PrisonsDocument6 pagesDebate 3 Youth Incarceration in Adult PrisonsawuahbohNo ratings yet
- STDA VaricealDocument8 pagesSTDA VaricealDeisy de JesusNo ratings yet
- Article For CET CHFDocument5 pagesArticle For CET CHFawuahbohNo ratings yet
- Article For Jouranal 2 (498P)Document5 pagesArticle For Jouranal 2 (498P)awuahbohNo ratings yet
- Patient Report FormDocument1 pagePatient Report FormawuahbohNo ratings yet
- Article For Journal 4-18-14Document8 pagesArticle For Journal 4-18-14awuahbohNo ratings yet
- Article For JournalDocument6 pagesArticle For JournalawuahbohNo ratings yet
- Thai Yoga Massage Beginners Course Berlin 2011Document66 pagesThai Yoga Massage Beginners Course Berlin 2011SabaiSabaiNuadthai100% (2)
- Carl Rogers - Person-Centered Theory PDFDocument21 pagesCarl Rogers - Person-Centered Theory PDFAiden Lee50% (2)
- Case PresentationDocument31 pagesCase PresentationYogaPratayogaMNo ratings yet
- NCP AppendectomyDocument6 pagesNCP Appendectomymahmoud fuqahaNo ratings yet
- Tongue Placement and Dental AlignmentDocument3 pagesTongue Placement and Dental AlignmentStella PapadopoulouNo ratings yet
- WL-UU551 User Manual: Multi-Function RF Cavitation DeviceDocument10 pagesWL-UU551 User Manual: Multi-Function RF Cavitation DeviceCata GodoyNo ratings yet
- Sciatica ExercisesDocument14 pagesSciatica ExercisesEric Chambers100% (2)
- Chiro Guidelines WHODocument51 pagesChiro Guidelines WHOMinh MinhNo ratings yet
- Handbook of Digestive DiseasesDocument561 pagesHandbook of Digestive DiseasesOdiet RevenderNo ratings yet
- Nirali Final Synopsis PDFDocument31 pagesNirali Final Synopsis PDFNIRALI MISTRYNo ratings yet
- Shoulder Special Tests and Rotator Cuff AssessmentDocument5 pagesShoulder Special Tests and Rotator Cuff AssessmentTomáš KrajíčekNo ratings yet
- Cardio 1stSemSY2014-15 Course SyllabusDocument6 pagesCardio 1stSemSY2014-15 Course SyllabusBeryl Ben MergalNo ratings yet
- 1-Safe-Comfortable PlaceDocument2 pages1-Safe-Comfortable Placeapi-273614596No ratings yet
- TevaDocument4 pagesTevaKarthikeya SaiNo ratings yet
- PDF Takayasu Arteritis 2 PDFDocument5 pagesPDF Takayasu Arteritis 2 PDFPadmaja PriyadarshiniNo ratings yet
- Therapeutic Potential of Stem Cells in Regenerative Dentistry A Review of LiteratureDocument9 pagesTherapeutic Potential of Stem Cells in Regenerative Dentistry A Review of LiteratureAamir BugtiNo ratings yet
- Reinforcement in The Classroom Improves Student Motivation and PerformanceDocument4 pagesReinforcement in The Classroom Improves Student Motivation and PerformancePassmore DubeNo ratings yet
- 5 Stages of Counseling ProsesDocument16 pages5 Stages of Counseling ProsesAraby Alfandani100% (1)
- Study of Hamam - A Regimental Therapy: Omme Salma & Nazeer HussainDocument6 pagesStudy of Hamam - A Regimental Therapy: Omme Salma & Nazeer HussainSher KhanNo ratings yet
- VWC Writing A Case ConceptualizationDocument3 pagesVWC Writing A Case ConceptualizationTiến ThànhNo ratings yet
- Gamma CameraDocument26 pagesGamma CameraNishtha TanejaNo ratings yet
- Prismaflex TrainingDocument37 pagesPrismaflex TrainingSarah Al-Qadri100% (4)
- Interventions Homework RefusalDocument5 pagesInterventions Homework Refusalafetvdqbt100% (1)
- HER CCB in Crisis HypertensionDocument22 pagesHER CCB in Crisis HypertensionHandi Wijaya HasanNo ratings yet
- IMCI Chart BookletDocument66 pagesIMCI Chart Bookletnorwin_033875No ratings yet
- Retinoblastoma - EyeWikiDocument11 pagesRetinoblastoma - EyeWikimay171989No ratings yet
- Nine Essential Oils Everyday Use Barb LemkeDocument31 pagesNine Essential Oils Everyday Use Barb LemkeWalaa ElleithyNo ratings yet
- Case Presentation Output Checklist and Format and Master OutputDocument18 pagesCase Presentation Output Checklist and Format and Master OutputVenRussAbestaNo ratings yet
- Novorapid Product Monograph PDFDocument50 pagesNovorapid Product Monograph PDFAtid AmandaNo ratings yet
- BMJ k2693 FullDocument9 pagesBMJ k2693 FullFirman SyahNo ratings yet