You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Lampiran JurnalDocument3 pagesLampiran JurnalpebinscribdNo ratings yet
- Daftar Pustaka Bab IVDocument1 pageDaftar Pustaka Bab IVpebinscribdNo ratings yet
- Consumer BehaviorDocument11 pagesConsumer BehaviorpebinscribdNo ratings yet
- Lampiran JurnalDocument3 pagesLampiran JurnalpebinscribdNo ratings yet
- Dapus BAB IIDocument2 pagesDapus BAB IIpebinscribdNo ratings yet
- Vitamin D and Fracture Risk in Early ChildhoodDocument8 pagesVitamin D and Fracture Risk in Early ChildhoodpebinscribdNo ratings yet
- Scope and Meaning of Accounting 1: Accounting and Its Relationship To Shareholder Value and Business StructureDocument4 pagesScope and Meaning of Accounting 1: Accounting and Its Relationship To Shareholder Value and Business StructurepebinscribdNo ratings yet
- Lion Air Eticket Itinerary / ReceiptDocument2 pagesLion Air Eticket Itinerary / ReceiptpebinscribdNo ratings yet
- Cardiac ArrhytmiasDocument4 pagesCardiac ArrhytmiaspebinscribdNo ratings yet
- Alrubaiee PDFDocument25 pagesAlrubaiee PDFpebinscribdNo ratings yet
- Mikroekonomi Dan Kebijakan PublikDocument14 pagesMikroekonomi Dan Kebijakan PublikpebinscribdNo ratings yet
- MaternalandFetal Physiology - 111532Document3 pagesMaternalandFetal Physiology - 111532viannikkkyNo ratings yet
- Lanjutan Data Pasien DMDocument1 pageLanjutan Data Pasien DMpebinscribdNo ratings yet
- J Neurol Neurosurg Psychiatry 2016 Gonçalves JNNP 2016 313458Document7 pagesJ Neurol Neurosurg Psychiatry 2016 Gonçalves JNNP 2016 313458pebinscribdNo ratings yet
- Irdr 4 105Document3 pagesIrdr 4 105pebinscribdNo ratings yet
- J Neurol Neurosurg Psychiatry 2016 Noyce JNNP 2015 311890Document9 pagesJ Neurol Neurosurg Psychiatry 2016 Noyce JNNP 2015 311890pebinscribdNo ratings yet
- 3 KonjungtivaDocument42 pages3 KonjungtivapebinscribdNo ratings yet
- Head Computed Tomography: Subagia Santoso Sudjono Departement of Radiology Gatot Subroto Central Army HospitalDocument81 pagesHead Computed Tomography: Subagia Santoso Sudjono Departement of Radiology Gatot Subroto Central Army HospitalpebinscribdNo ratings yet
- Guidelines For Ambulatory Anesthesia and SurgeryDocument2 pagesGuidelines For Ambulatory Anesthesia and SurgerypebinscribdNo ratings yet
- J Neurol Neurosurg Psychiatry 2016 Dlouhy 402 13Document13 pagesJ Neurol Neurosurg Psychiatry 2016 Dlouhy 402 13pebinscribdNo ratings yet
- Case Report: Tubocutaneous FistulaDocument2 pagesCase Report: Tubocutaneous FistulapebinscribdNo ratings yet
- Irdr 4 105Document3 pagesIrdr 4 105pebinscribdNo ratings yet
- 2014 Article 369Document6 pages2014 Article 369pebinscribdNo ratings yet
- 2014 Article 369Document6 pages2014 Article 369pebinscribdNo ratings yet
- Paediatric Guidelines EUADocument47 pagesPaediatric Guidelines EUApebinscribdNo ratings yet
- Zooterapia JornalEthnobiologyDocument43 pagesZooterapia JornalEthnobiologyEdilene Coffaci de LimaNo ratings yet
- Estrogen Treatment Predisposes To Severe andDocument7 pagesEstrogen Treatment Predisposes To Severe andpebinscribdNo ratings yet
- ASA Status FisikDocument1 pageASA Status FisikpebinscribdNo ratings yet
- Kalaweit Gibbons and Siamang Conservation ProgrammeDocument3 pagesKalaweit Gibbons and Siamang Conservation ProgrammepebinscribdNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Electrical Power System Device Function NumberDocument2 pagesElectrical Power System Device Function Numberdan_teegardenNo ratings yet
- Full Download Short Term Financial Management 3rd Edition Maness Test BankDocument35 pagesFull Download Short Term Financial Management 3rd Edition Maness Test Bankcimanfavoriw100% (31)
- Biologically Active Compounds From Hops and Prospects For Their Use - Karabín 2016Document26 pagesBiologically Active Compounds From Hops and Prospects For Their Use - Karabín 2016Micheli Legemann MonteNo ratings yet
- Kwasaki ZX10R 16Document101 pagesKwasaki ZX10R 16OliverNo ratings yet
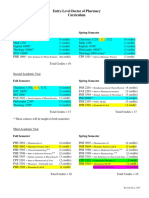
- Pharmd CurriculumDocument18 pagesPharmd Curriculum5377773No ratings yet
- 09.tracheostomy Management by Speech Language Pathologists in SwedenDocument12 pages09.tracheostomy Management by Speech Language Pathologists in SwedenCarlonchaCáceresNo ratings yet
- 40 RT-flex Control-System Rev01Document68 pages40 RT-flex Control-System Rev01Mayvon Botelho100% (2)
- The Joy Luck Club Book 1Document12 pagesThe Joy Luck Club Book 1loronalicelNo ratings yet
- Stanley B. Alpern - Amazons of Black Sparta - The Women Warriors of Dahomey-New York University Press (2011)Document308 pagesStanley B. Alpern - Amazons of Black Sparta - The Women Warriors of Dahomey-New York University Press (2011)georgemultiplusNo ratings yet
- Accsap 10 VHDDocument94 pagesAccsap 10 VHDMuhammad Javed Gaba100% (2)
- Vehicle Intercom Systems (VIS)Document4 pagesVehicle Intercom Systems (VIS)bbeisslerNo ratings yet
- Adaptive Cruise ControlDocument5 pagesAdaptive Cruise ControlIJIRSTNo ratings yet
- Fentanyl - Wikipedia, The Free EncyclopediaDocument13 pagesFentanyl - Wikipedia, The Free EncyclopediaKeren SingamNo ratings yet
- Genie GS-1930 Parts ManualDocument194 pagesGenie GS-1930 Parts ManualNestor Matos GarcíaNo ratings yet
- Energy Transfer in Cell During Exercise and Oxygen Metabolism and Transport - PalakDocument85 pagesEnergy Transfer in Cell During Exercise and Oxygen Metabolism and Transport - Palakpalooo4No ratings yet
- Application of PCA-CNN (Principal Component Analysis - Convolutional Neural Networks) Method On Sentinel-2 Image Classification For Land Cover MappingDocument5 pagesApplication of PCA-CNN (Principal Component Analysis - Convolutional Neural Networks) Method On Sentinel-2 Image Classification For Land Cover MappingIJAERS JOURNALNo ratings yet
- Math 202 Syllabus-Spring18 PDFDocument2 pagesMath 202 Syllabus-Spring18 PDFvonacoc49No ratings yet
- (G. Lakshmi Narasaiah) Finite Element Analysis PDFDocument349 pages(G. Lakshmi Narasaiah) Finite Element Analysis PDFmoljaime1326No ratings yet
- Easergy PS100 48VDC Power SupplyDocument2 pagesEasergy PS100 48VDC Power SupplyRichard SyNo ratings yet
- LPG GasDocument39 pagesLPG Gasv prasanthNo ratings yet
- Imbinari Teava Fibra de Sticla PDFDocument1 pageImbinari Teava Fibra de Sticla PDFplex015No ratings yet
- CAC Bubble DiagramsDocument12 pagesCAC Bubble Diagramsangst6250No ratings yet
- 412 X 7 Va CJ CSDocument1 page412 X 7 Va CJ CSRajesh KumarNo ratings yet
- Unnatural Selection BiologyDocument2 pagesUnnatural Selection BiologyAlexa ChaviraNo ratings yet
- 3.1 - Sequences and SeriesxbxhhdDocument92 pages3.1 - Sequences and SeriesxbxhhdHelloNo ratings yet
- 39ED3050CT - RT49S - AP Service ManualDocument31 pages39ED3050CT - RT49S - AP Service Manualبوند بوند100% (1)
- Rac Question PaperDocument84 pagesRac Question PaperibrahimNo ratings yet
- DCS YokogawaDocument17 pagesDCS Yokogawasswahyudi100% (1)
- Factors Affecting Physical FitnessDocument7 pagesFactors Affecting Physical FitnessMary Joy Escanillas Gallardo100% (2)
- Exercise 9 Two Factor Factorial Experiments and Derivation of Expected Mean SquaresDocument14 pagesExercise 9 Two Factor Factorial Experiments and Derivation of Expected Mean SquaresHasmaye PintoNo ratings yet