You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Disorders of Coagulation and Fibrinolysis: Presented By: Toyco, Psyche Earl Monserrat Rojo, Kyzsa FranzDocument58 pagesDisorders of Coagulation and Fibrinolysis: Presented By: Toyco, Psyche Earl Monserrat Rojo, Kyzsa FranzFearless AngelNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Nattokinase PDFDocument9 pagesNattokinase PDFAnton SorinNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Physiology of CoagulationDocument44 pagesPhysiology of CoagulationXee JayNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Yumizen G FIB 5: Ibrinogen EagentDocument2 pagesYumizen G FIB 5: Ibrinogen EagentNAKANWAGI JOSLYLINENo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- ACUTE PHASE PROTEINS FinalDocument29 pagesACUTE PHASE PROTEINS FinalMorgan100% (1)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Contemporary Management of Major Haemorrhage in Critical CareDocument13 pagesContemporary Management of Major Haemorrhage in Critical CareYo MeNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Coagulopathy in Cardiac Surgery1Document63 pagesCoagulopathy in Cardiac Surgery1Mohammed Abdul ShafiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Blood and Blood ProductsDocument52 pagesBlood and Blood Productswellawalalasith100% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Automated Blood Coagulation Analyzer CA-50: Basic Data Sheet - (Fibrinogen)Document8 pagesAutomated Blood Coagulation Analyzer CA-50: Basic Data Sheet - (Fibrinogen)Aahsan Iqbal احسن اقبالNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Phleb LabDocument18 pagesPhleb LabMikee Patricia TrinidadNo ratings yet
- Management of Bleeding PDFDocument25 pagesManagement of Bleeding PDFGlory Owens AgbonkpoloNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Disorders of Coagulation FactorsDocument35 pagesDisorders of Coagulation FactorsMelesNo ratings yet
- Abordaje Niño Que Sangra Hematologia de OskyDocument13 pagesAbordaje Niño Que Sangra Hematologia de OskyivanNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Pre-Analytical Variables in Coagulation TestingDocument20 pagesPre-Analytical Variables in Coagulation TestingTaylorNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Nicola Maffulli (Eds.) - Platelet Rich Plasma in Musculoskeletal Practice-Springer-Verlag London (2016) PDFDocument256 pagesNicola Maffulli (Eds.) - Platelet Rich Plasma in Musculoskeletal Practice-Springer-Verlag London (2016) PDFedbraga-1No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Disseminated Intravascular Coagulation (DIC)Document24 pagesDisseminated Intravascular Coagulation (DIC)Atiya HajjajNo ratings yet
- Reptilase: Haemocoagulase 1 NIH UnitDocument21 pagesReptilase: Haemocoagulase 1 NIH UnitkyawkyawhtayNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Thrombin Time - GRP 5Document14 pagesThrombin Time - GRP 5Joyce LeeNo ratings yet
- 4 EpistaxisDocument51 pages4 EpistaxisNicNo ratings yet
- Blood A Connective Tissue in Fluid FormDocument3 pagesBlood A Connective Tissue in Fluid Formjacc_282No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Soal Ulangan Harian Sistem Sirkulasi (Tanggapan)Document65 pagesSoal Ulangan Harian Sistem Sirkulasi (Tanggapan)Dortje Pili RoboNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 136 Management of Major Haemorrhage Part 1Document6 pages136 Management of Major Haemorrhage Part 1fitrah fajrianiNo ratings yet
- Serum Protein Electrophoresis: Edited by RaniDocument66 pagesSerum Protein Electrophoresis: Edited by RaniMustakim DuharingNo ratings yet
- Acquired Coagulation AbnormalitiesDocument6 pagesAcquired Coagulation AbnormalitiesDrMohammad MoyassarNo ratings yet
- Hematology: Presented by Alyazeed Hussein, BSCDocument96 pagesHematology: Presented by Alyazeed Hussein, BSCMONFOLANo ratings yet
- At 13450Document2 pagesAt 13450dr_joe23No ratings yet
- Humaclot JuniorDocument40 pagesHumaclot JuniorJonatan Rolong Ibáñez100% (3)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
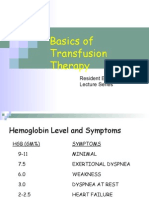
- Basics of Transfusion TherapyDocument43 pagesBasics of Transfusion TherapyMuhammad Afyudin DjumhuriNo ratings yet
- Hemostasis ReviewerDocument14 pagesHemostasis ReviewerDayledaniel SorvetoNo ratings yet
- DIC in PregnancyDocument41 pagesDIC in PregnancytapayanaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)