You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Celta Application Form and Language Awareness Task - British Council Bangladesh 1Document7 pagesCelta Application Form and Language Awareness Task - British Council Bangladesh 1rehan3038No ratings yet
- k1 Grading Sheet Sy 2016 2017Document11 pagesk1 Grading Sheet Sy 2016 2017Vangie SalvacionNo ratings yet
- English: Weekly AssessmentDocument3 pagesEnglish: Weekly AssessmentVangie SalvacionNo ratings yet
- 21 - Addition Made Easy PDFDocument1 page21 - Addition Made Easy PDFVangie SalvacionNo ratings yet
- 15 Addition Made EasyDocument1 page15 Addition Made EasyVangie SalvacionNo ratings yet
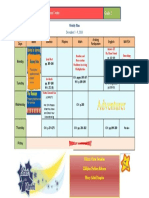
- Adventist Education Center Grade 2: December 5 - 9, 2016Document1 pageAdventist Education Center Grade 2: December 5 - 9, 2016Vangie SalvacionNo ratings yet
- 15 Addition Made EasyDocument1 page15 Addition Made EasyVangie SalvacionNo ratings yet
- Math AdditionDocument1 pageMath AdditionVangie SalvacionNo ratings yet
- Weekly Assessment: Grade 2Document2 pagesWeekly Assessment: Grade 2Vangie SalvacionNo ratings yet
- Adventist Education Center Grade 2: Weekly Plan & Pointers For The ExamDocument1 pageAdventist Education Center Grade 2: Weekly Plan & Pointers For The ExamVangie SalvacionNo ratings yet
- Additions made easy with number bondsDocument1 pageAdditions made easy with number bondsVangie SalvacionNo ratings yet
- 19 - Addition Made Easy PDFDocument1 page19 - Addition Made Easy PDFVangie SalvacionNo ratings yet
- 20 - Addition Made Easy PDFDocument1 page20 - Addition Made Easy PDFVangie SalvacionNo ratings yet
- 15 Addition Made EasyDocument1 page15 Addition Made EasyVangie SalvacionNo ratings yet
- 15 Addition Made EasyDocument1 page15 Addition Made EasyVangie SalvacionNo ratings yet
- Addition WorksheetDocument1 pageAddition WorksheetVangie SalvacionNo ratings yet
- 21 Addition Made EasyDocument1 page21 Addition Made EasyVangie SalvacionNo ratings yet
- 19 - Addition Made Easy PDFDocument1 page19 - Addition Made Easy PDFVangie SalvacionNo ratings yet
- Additions made easy with number bondsDocument1 pageAdditions made easy with number bondsVangie SalvacionNo ratings yet
- 15 Addition Made EasyDocument1 page15 Addition Made EasyVangie SalvacionNo ratings yet
- 15 Addition Made EasyDocument1 page15 Addition Made EasyVangie SalvacionNo ratings yet
- 13 - Addition Made Easy PDFDocument1 page13 - Addition Made Easy PDFVangie SalvacionNo ratings yet
- 15 Addition Made EasyDocument1 page15 Addition Made EasyVangie SalvacionNo ratings yet
- 10 - Addition Made Easy PDFDocument1 page10 - Addition Made Easy PDFVangie SalvacionNo ratings yet
- 15 Addition Made EasyDocument1 page15 Addition Made EasyVangie SalvacionNo ratings yet
- Math Addition WorksheetDocument1 pageMath Addition WorksheetVangie SalvacionNo ratings yet
- Swimming CertificateDocument1 pageSwimming CertificateVangie SalvacionNo ratings yet
- 14 Addition Made EasyDocument1 page14 Addition Made EasyVangie SalvacionNo ratings yet
- Addition WorksheetDocument1 pageAddition WorksheetVangie SalvacionNo ratings yet
- 9 - Addition Made Easy PDFDocument1 page9 - Addition Made Easy PDFVangie SalvacionNo ratings yet
- 10 Addition Made EasyDocument1 page10 Addition Made EasyVangie SalvacionNo ratings yet
- Test English Skills Free Online Cambridge ESOLDocument5 pagesTest English Skills Free Online Cambridge ESOLEnrique GomezNo ratings yet
- Trabajo Aplicativo de InglesDocument7 pagesTrabajo Aplicativo de InglesKaren CA100% (1)
- Our Stories - FirstPeoplesinCanadaDocument223 pagesOur Stories - FirstPeoplesinCanadawitzaneyjNo ratings yet
- Hamdard Prospectus 2012-13Document126 pagesHamdard Prospectus 2012-13Dev KannuNo ratings yet
- Living Forever Lesson PlanDocument6 pagesLiving Forever Lesson Planapi-425637153No ratings yet
- CAS Ideas For ProjectsDocument18 pagesCAS Ideas For ProjectsDana PorterNo ratings yet
- Knox News June 2009Document18 pagesKnox News June 2009knoxacademyNo ratings yet
- Placement BrochureDocument21 pagesPlacement BrochureTechniworkNo ratings yet
- Analyzing EFL Teaching Challenges and Strategies in Rural SchoolsDocument55 pagesAnalyzing EFL Teaching Challenges and Strategies in Rural SchoolsIshak MalundaNo ratings yet
- Joanne Mae VDocument2 pagesJoanne Mae VAndrea Denise VillafuerteNo ratings yet
- The Natural ApproachDocument204 pagesThe Natural ApproachVal RibeiroNo ratings yet
- The Fun They HadDocument3 pagesThe Fun They Hadbethfelts100% (1)
- UT Dallas Syllabus For cs3305.501.09s Taught by Timothy Farage (Tfarage)Document6 pagesUT Dallas Syllabus For cs3305.501.09s Taught by Timothy Farage (Tfarage)UT Dallas Provost's Technology GroupNo ratings yet
- Local StudiesDocument12 pagesLocal StudiesJohn Christopher PalacioNo ratings yet
- Free Public Secondary Education ActDocument2 pagesFree Public Secondary Education ActJemaica TumulakNo ratings yet
- Harry Potter House Quiz Which Hogwarts House Do You Belong inDocument1 pageHarry Potter House Quiz Which Hogwarts House Do You Belong inaNo ratings yet
- Brittany Bowery Resume 2014Document2 pagesBrittany Bowery Resume 2014api-250607203No ratings yet
- Identifying ParallelogramsDocument6 pagesIdentifying ParallelogramsKheza Bohol Deliman DañasNo ratings yet
- Present Simple and Continuous TensesDocument5 pagesPresent Simple and Continuous Tensesjurgute2000No ratings yet
- Mahindra CSRDocument30 pagesMahindra CSRNirvi DesaiNo ratings yet
- FSC 1Document1 pageFSC 1Talha Rafique ChaudharyNo ratings yet
- Adibah Abd RahimDocument4 pagesAdibah Abd RahimALia NadhirahNo ratings yet
- The Enigma of Academics Revealing The Positive Effects of School Attendance Policies. FINAL. 2Document8 pagesThe Enigma of Academics Revealing The Positive Effects of School Attendance Policies. FINAL. 2Angelica CarreonNo ratings yet
- One Student One Sport - Sheikh Kamaruddin 01Document10 pagesOne Student One Sport - Sheikh Kamaruddin 01Zd ZaidiNo ratings yet
- Guidance Program GoalsDocument2 pagesGuidance Program GoalsMelcar BalabaNo ratings yet
- Isabela gov't backs DepEd programs with new classroom fundingDocument5 pagesIsabela gov't backs DepEd programs with new classroom fundingronalyn bustobaNo ratings yet
- Daily Instruction For Beginning ELLs (Excerpt From The ESL/ELL Teacher's Survival Guide)Document10 pagesDaily Instruction For Beginning ELLs (Excerpt From The ESL/ELL Teacher's Survival Guide)Jossey-Bass EducationNo ratings yet
- Collection PolicyDocument3 pagesCollection Policyapi-283167925No ratings yet
- Classroom Management Plan - Blank TemplateDocument3 pagesClassroom Management Plan - Blank Templateapi-300194441No ratings yet