You might also like
- Cartoon Fundamentals: How To Draw A Cartoon Body - Envato Tuts+ Design & Illustration ArticleDocument21 pagesCartoon Fundamentals: How To Draw A Cartoon Body - Envato Tuts+ Design & Illustration ArticleAnonymous e49Vjy0100% (4)
- Board Exam PrimerDocument9 pagesBoard Exam PrimerEngr Jibril Naval Labiao67% (3)
- Tetanus Case PresentationDocument18 pagesTetanus Case PresentationDesiree Guerra100% (1)
- Blood Report TateDocument4 pagesBlood Report TateGina Watkins100% (2)
- Types of ImmunizationsDocument21 pagesTypes of Immunizationsmacmactongos100% (6)
- Intrusion With Mini ImplantDocument13 pagesIntrusion With Mini Implantdrzana78100% (1)
- Beary Bearnita. Winnie Pooh. WinnieDocument22 pagesBeary Bearnita. Winnie Pooh. Winniejosita100% (12)
- TetanusDocument31 pagesTetanusreresNo ratings yet
- Animal Testing StsDocument9 pagesAnimal Testing StsRona Mae Alcayaga Aringo100% (1)
- Expanded Program For Immunization (EPI)Document70 pagesExpanded Program For Immunization (EPI)Erwin Jake Taguba100% (1)
- 5 Free Knitted ToysDocument20 pages5 Free Knitted ToysMihaiCamelia0% (2)
- Ortodoncia Bishara 644 Pag-41Document604 pagesOrtodoncia Bishara 644 Pag-41pedro picapiedra100% (1)
- Tetanus - CDCDocument23 pagesTetanus - CDCPradita Sri MitasariNo ratings yet
- Tetanus - The DiseaseDocument6 pagesTetanus - The Diseasemanjunath mamathaNo ratings yet
- Tetanus Toxoid For Booster Use Only: (Not Recommended For Primary Immunization)Document5 pagesTetanus Toxoid For Booster Use Only: (Not Recommended For Primary Immunization)Ade PurnaNo ratings yet
- Diphtheria: Questions and Answers: Information About The Disease and VaccinesDocument3 pagesDiphtheria: Questions and Answers: Information About The Disease and VaccinesGlenn KristieNo ratings yet
- TetanusDocument18 pagesTetanusRohan TejaNo ratings yet
- Immunization EPI Huda 201212Document5 pagesImmunization EPI Huda 201212Aerish TupazNo ratings yet
- Fact Sheet TetanusDocument4 pagesFact Sheet TetanusSOMANATHAN UMAHSUTHANNo ratings yet
- Tetanus: HistoryDocument15 pagesTetanus: HistorydanielleNo ratings yet
- Chapter 21Document8 pagesChapter 21daniphilip777No ratings yet
- TetanusDocument4 pagesTetanusSneha SnehaNo ratings yet
- TetanusDocument34 pagesTetanusBintang Ruth Cecilia FebrinaNo ratings yet
- 2 Review Diphtheria Results April2017 Final Clean PDFDocument20 pages2 Review Diphtheria Results April2017 Final Clean PDFchameleonNo ratings yet
- DIPHTHERIADocument6 pagesDIPHTHERIAblack_knight118No ratings yet
- Tetanus Vaccine: Jump To Navigation Jump To SearchDocument6 pagesTetanus Vaccine: Jump To Navigation Jump To Searchnova puspitasariNo ratings yet
- TetanusDocument6 pagesTetanusImmelda Stella Medessoh DohoNo ratings yet
- Guidelines On TetanusDocument2 pagesGuidelines On Tetanusich4_28No ratings yet
- Expanded Program On Immunization CHNDocument4 pagesExpanded Program On Immunization CHNgeralynroseNo ratings yet
- Expanded Program On ImmunizationDocument4 pagesExpanded Program On ImmunizationMac Lester DumagNo ratings yet
- 54 TetanusDocument25 pages54 Tetanusghofran001997No ratings yet
- Facts About Tetanus DeseaseDocument1 pageFacts About Tetanus DeseasechaariaNo ratings yet
- TetanusDocument35 pagesTetanusAlkamis Rabiu UsmanNo ratings yet
- Vaksin DPTDocument5 pagesVaksin DPTali subchanNo ratings yet
- Tetanus Toxoid Immunization Schedule For WomenDocument4 pagesTetanus Toxoid Immunization Schedule For WomenEdwin Delos Reyes AbuNo ratings yet
- Patofisiologi DifteriDocument11 pagesPatofisiologi DifteriicorrrNo ratings yet
- Alberta TetanusDocument7 pagesAlberta TetanusranggaNo ratings yet
- Trachoma Tetanus LeprosyDocument40 pagesTrachoma Tetanus LeprosyOsama adel Mohamed SmadiNo ratings yet
- Infectious Pertusis-6 (Muhadharaty)Document5 pagesInfectious Pertusis-6 (Muhadharaty)dr.salam.hassaniNo ratings yet
- Tetanus: Information For Health Professionals.: HPA-CDSC November 2003Document6 pagesTetanus: Information For Health Professionals.: HPA-CDSC November 2003yaniNo ratings yet
- DR Swati Rajagopal - Adult VaccinationDocument50 pagesDR Swati Rajagopal - Adult VaccinationYabooNo ratings yet
- TB Guidance Chapter 2Document15 pagesTB Guidance Chapter 2dindaNo ratings yet
- Dis Tetanus Color OfficeDocument1 pageDis Tetanus Color Officejm_ftaaNo ratings yet
- ATLS-9e Elearn Tetanus.v1 PDFDocument2 pagesATLS-9e Elearn Tetanus.v1 PDFAdolfo Rfael Gomez EspinosaNo ratings yet
- Diphtheria: WHO Position PapersDocument2 pagesDiphtheria: WHO Position PaperssakuraleeshaoranNo ratings yet
- Tetanus CDC For ClinicianDocument5 pagesTetanus CDC For ClinicianAspen HOAnakNo ratings yet
- CDC Diphtheria Surveillance WorksheetDocument6 pagesCDC Diphtheria Surveillance WorksheetLuna WhiteNo ratings yet
- Tetanus: 1. Disease ReportingDocument6 pagesTetanus: 1. Disease ReportingTimi SupuNo ratings yet
- 2 MDW 204 Target Disease Vaccines & Cold ChainDocument34 pages2 MDW 204 Target Disease Vaccines & Cold ChainMaria Lejani TerencioNo ratings yet
- Tetanus Diseases BingDocument16 pagesTetanus Diseases Bingnurma jafarNo ratings yet
- TetanusDocument7 pagesTetanusallah akbarNo ratings yet
- Nursing Care For MeaslesDocument5 pagesNursing Care For MeaslesChristian Eduard de DiosNo ratings yet
- BCG Vaccine: Salk's Polio Vaccine "Inactivated Polio Vaccine" IPV InjectableDocument6 pagesBCG Vaccine: Salk's Polio Vaccine "Inactivated Polio Vaccine" IPV InjectableHandre PutraNo ratings yet
- DTap Info PDFDocument1 pageDTap Info PDFxxxNo ratings yet
- DTap Info PDFDocument1 pageDTap Info PDFxxxNo ratings yet
- Tetanus EmedicineDocument19 pagesTetanus EmedicineSapto SutardiNo ratings yet
- Brief: Tetanus Disease, Treatment, ManagementDocument5 pagesBrief: Tetanus Disease, Treatment, ManagementchindiaNo ratings yet
- Tetanus: Acute Communicable Disease Control Manual (B-73) Revision - February 2012Document2 pagesTetanus: Acute Communicable Disease Control Manual (B-73) Revision - February 2012Hisashi Ren MinamotoNo ratings yet
- Signs and SymptomsDocument6 pagesSigns and Symptomsdareine22No ratings yet
- VACCINESDocument8 pagesVACCINESzilikajainNo ratings yet
- Vaccination: Passive ImmunityDocument12 pagesVaccination: Passive ImmunityuouoNo ratings yet
- Primary Prevention: CDC: Immunization SchedulesDocument4 pagesPrimary Prevention: CDC: Immunization Schedulesjourey08No ratings yet
- Diphtheria, Tetanus and PoliomyelitisDocument11 pagesDiphtheria, Tetanus and PoliomyelitisPriyanka SinghNo ratings yet
- AIP BP Tetanus PEPDocument3 pagesAIP BP Tetanus PEPSatrio WicaksonoNo ratings yet
- Health Advice and Immunizations for TravelersFrom EverandHealth Advice and Immunizations for TravelersNo ratings yet
- Good Health in the Tropics: Advice to Travellers and SettlersFrom EverandGood Health in the Tropics: Advice to Travellers and SettlersNo ratings yet
- Maternal Mortality Among Women Seeking Health Care Services in Kisii Level 5 HospitalDocument6 pagesMaternal Mortality Among Women Seeking Health Care Services in Kisii Level 5 HospitalDaphne Ongbit JaritoNo ratings yet
- ProposalDocument14 pagesProposalDaphne Ongbit JaritoNo ratings yet
- Banco de Oro (BDO) - Online Bills Payment: Credit ScheduleDocument1 pageBanco de Oro (BDO) - Online Bills Payment: Credit ScheduleDaphne Ongbit JaritoNo ratings yet
- WHO Dengue Guidelines 2013Document160 pagesWHO Dengue Guidelines 2013Jason MirasolNo ratings yet
- 3rd Paragraph PDFDocument36 pages3rd Paragraph PDFDaphne Ongbit JaritoNo ratings yet
- Gold in IRA - May6Document5 pagesGold in IRA - May6Daphne Ongbit JaritoNo ratings yet
- 14 146 v13n6 2014 RiskCarcinogenesisDocument8 pages14 146 v13n6 2014 RiskCarcinogenesisDaphne Ongbit JaritoNo ratings yet
- Acute Diare WHO 2005Document50 pagesAcute Diare WHO 2005Boby Abdul RahmanNo ratings yet
- CholeDocument4 pagesCholeDaphne Ongbit JaritoNo ratings yet
- CholeDocument4 pagesCholeDaphne Ongbit JaritoNo ratings yet
- 2014 Evidence-Based Guideline For The Management HypertensionDocument14 pages2014 Evidence-Based Guideline For The Management HypertensionEganata NugrahaNo ratings yet
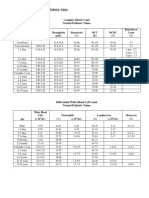
- 30a2131 Complete Blood Count Normal Pediatric Values PDFDocument1 page30a2131 Complete Blood Count Normal Pediatric Values PDFReziel Basilan Manalo100% (2)
- Worksheet Hp03Document8 pagesWorksheet Hp03Daphne Ongbit JaritoNo ratings yet
- Southwestern University Matias H. Aznar Memorial College of Medicine Urgello ST., Cebu City, PhilippinesDocument1 pageSouthwestern University Matias H. Aznar Memorial College of Medicine Urgello ST., Cebu City, PhilippinesDaphne Ongbit JaritoNo ratings yet
- CHED ) Region 7 Forum 5514Document7 pagesCHED ) Region 7 Forum 5514Daphne Ongbit JaritoNo ratings yet
- ORL Interns NotesDocument15 pagesORL Interns NotesDaphne Ongbit JaritoNo ratings yet
- Clinician Rated Severity of Oppositional Defiant DisorderDocument2 pagesClinician Rated Severity of Oppositional Defiant DisorderDaphne Ongbit JaritoNo ratings yet
- SSC Bundle PDFDocument1 pageSSC Bundle PDFBramantyo NugrahaNo ratings yet
- 4 Computer System LecDocument9 pages4 Computer System LecDaphne Ongbit JaritoNo ratings yet
- A Lectin With Antifungal and Mitogenic Activities From Capsicum FrutescensDocument7 pagesA Lectin With Antifungal and Mitogenic Activities From Capsicum FrutescensDaphne Ongbit JaritoNo ratings yet
- A Brief History of Organic ChemistryDocument5 pagesA Brief History of Organic ChemistryDaphne Ongbit JaritoNo ratings yet
- VedanadhyayaDocument2 pagesVedanadhyayaAlapati Vinod KumarNo ratings yet
- Cruelty's Rewards - The Gratifications of Perpetrators and Spectators Victor NellDocument48 pagesCruelty's Rewards - The Gratifications of Perpetrators and Spectators Victor NellTernassNo ratings yet
- CnidariaDocument50 pagesCnidariacalvinleow1205No ratings yet
- Anatomy Unit 4 Skin and Body MembranesDocument45 pagesAnatomy Unit 4 Skin and Body MembranesJaren BalbalNo ratings yet
- Muscles-Pelvic Limb 6-Craniolateral CrusDocument2 pagesMuscles-Pelvic Limb 6-Craniolateral CrusR1pTid3No ratings yet
- Struma Nodosa 2Document10 pagesStruma Nodosa 2dewi rositaNo ratings yet
- Kejang Pada Gigitan Ular Berbisa: Laporan KasusDocument10 pagesKejang Pada Gigitan Ular Berbisa: Laporan KasusHerlina Sabe HaringNo ratings yet
- Fauna Paraguay Handbook of The Mammals of Paraguay IIDocument120 pagesFauna Paraguay Handbook of The Mammals of Paraguay IIportalguaraniNo ratings yet
- Druid Handbook Part 3 Druid Spells ExaminedDocument30 pagesDruid Handbook Part 3 Druid Spells Examinedvtz06966No ratings yet
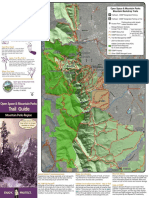
- Trail Guide: Open Space & Mountain ParksDocument2 pagesTrail Guide: Open Space & Mountain ParksKeith GruberNo ratings yet
- Osteology - Anatomical Orientations, Planes, DirectionsDocument74 pagesOsteology - Anatomical Orientations, Planes, DirectionsCagatay BarutNo ratings yet
- An Duong Vuong High School - Mock Test K1006 Full Name - 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11Document5 pagesAn Duong Vuong High School - Mock Test K1006 Full Name - 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11KIMTHOANo ratings yet
- Harvest Moon The Tale of Two Towns (Walkthrough)Document23 pagesHarvest Moon The Tale of Two Towns (Walkthrough)Diki Roy Nirwansyah0% (1)
- (Hong Et Al 2012) Effects of Fermented Black Soybean Pulp On Lipid and Bone Metabolism in Ovariectomized RatsDocument7 pages(Hong Et Al 2012) Effects of Fermented Black Soybean Pulp On Lipid and Bone Metabolism in Ovariectomized RatsSie ningsihNo ratings yet
- Evolutionary Relationship in Kingdom Plantae: Dependence of Gametophyte and Sporophyte Water Dependence in FertilizationDocument4 pagesEvolutionary Relationship in Kingdom Plantae: Dependence of Gametophyte and Sporophyte Water Dependence in FertilizationAida AisyahNo ratings yet
- Bitch Emaning - Google SearchDocument1 pageBitch Emaning - Google Search15. Kang, Hyunah 7DNo ratings yet
- Null 1Document41 pagesNull 1ايمن عادلNo ratings yet
- What Is Retained PlacentaDocument1 pageWhat Is Retained PlacentaKitkat Aquino CabugwasNo ratings yet
- To Be Accomplished by The Licensed Manning Agency.: Repatriation Information Sheet 2Document1 pageTo Be Accomplished by The Licensed Manning Agency.: Repatriation Information Sheet 2ian clark MarinduqueNo ratings yet
- Golgi ComplexDocument8 pagesGolgi ComplexvmshanesNo ratings yet
- AnalogyDocument94 pagesAnalogyRizwan KhanNo ratings yet
- EL 2021 PRELIM 4E5N P2 InsertDocument4 pagesEL 2021 PRELIM 4E5N P2 InsertLeng RyanNo ratings yet
- 4BI1 1BR Que 20190515Document32 pages4BI1 1BR Que 20190515crocusozan92% (12)