You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- HOSTEL FEE PAYMENT PROCEDURE FOR SY To FINAL YEARDocument2 pagesHOSTEL FEE PAYMENT PROCEDURE FOR SY To FINAL YEARAbhishek PawarNo ratings yet
- 32.kushtia (Life Old)Document6 pages32.kushtia (Life Old)Habib AliNo ratings yet
- Nutritional Status of Children With Autism Spectrum Disorders (Asds) : A Case-Control StudyDocument14 pagesNutritional Status of Children With Autism Spectrum Disorders (Asds) : A Case-Control StudyyeyesNo ratings yet
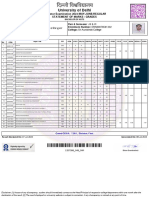
- University of Delhi: Semester Examination 2023-MAY-JUNE:REGULAR Statement of Marks / GradesDocument2 pagesUniversity of Delhi: Semester Examination 2023-MAY-JUNE:REGULAR Statement of Marks / GradesFit CollegeNo ratings yet
- Handbook Addendum: Student & ParentDocument42 pagesHandbook Addendum: Student & ParentExam PurposeNo ratings yet
- SpringDocument24 pagesSpringRiya IndukuriNo ratings yet
- IPLS Project Faculty ProspectusDocument11 pagesIPLS Project Faculty ProspectusMohan RaajNo ratings yet
- Jon Pumper Uttoradhikar PDFDocument56 pagesJon Pumper Uttoradhikar PDFArbanNo ratings yet
- 2004 - THOMPSON - The (Mis) Measurement of Body Image Ten Strategies To ImproveDocument8 pages2004 - THOMPSON - The (Mis) Measurement of Body Image Ten Strategies To ImproveCarolina RuasNo ratings yet
- Examination: Session: Course Title: Semester: Course Code: Max Marks: Date: 3/10/2020 Time: 12pm To 11:59amDocument2 pagesExamination: Session: Course Title: Semester: Course Code: Max Marks: Date: 3/10/2020 Time: 12pm To 11:59amsaqib aliNo ratings yet
- Opertti Et Al - Ibe Unesco 2021 Inclusion in EducDocument6 pagesOpertti Et Al - Ibe Unesco 2021 Inclusion in EducSergio RiquelmeNo ratings yet
- Ella Baker and The Black Freedom MovementDocument2 pagesElla Baker and The Black Freedom MovementslcozortNo ratings yet
- Spanish: Pearson Edexcel International GCSE 9-1Document4 pagesSpanish: Pearson Edexcel International GCSE 9-1Sharma DevNo ratings yet
- Progress Test 3Document8 pagesProgress Test 3Maria Agustina PirezNo ratings yet
- Alia Khoury Resume WeeblyDocument2 pagesAlia Khoury Resume Weeblyapi-221620521No ratings yet
- Knowledge Is WealthDocument100 pagesKnowledge Is WealthmustaqNo ratings yet
- Thaarinisudhakaran (4 3)Document1 pageThaarinisudhakaran (4 3)vineeth rockstar1999No ratings yet
- Grade 12 Q1 A1Document2 pagesGrade 12 Q1 A1Ma. Catherine PaternoNo ratings yet
- ACS Event Report 2Document2 pagesACS Event Report 2Chilamakuri M V TejaNo ratings yet
- Interview TipsDocument2 pagesInterview TipsIustina HaroianuNo ratings yet
- Verbs Worksheet 5th English Grammar NTSEDocument2 pagesVerbs Worksheet 5th English Grammar NTSESuvashreePradhanNo ratings yet
- NOSS Matrix - AssessorDocument2 pagesNOSS Matrix - AssessorFizan LaminNo ratings yet
- Mode of VerificationDocument15 pagesMode of VerificationVincent LibreaNo ratings yet
- The Effect of Mindset On Decision-MakingDocument27 pagesThe Effect of Mindset On Decision-MakingJessica PhamNo ratings yet
- Astronauts ScriptDocument3 pagesAstronauts ScriptakkurayhanNo ratings yet
- Iot Assignment 2Document8 pagesIot Assignment 2Meera SahooNo ratings yet
- Deca Full Proposal SchemeDocument3 pagesDeca Full Proposal SchemeAanuOluwapo EgberongbeNo ratings yet
- Demo K-12 Math Using 4a's Diameter of CircleDocument4 pagesDemo K-12 Math Using 4a's Diameter of CircleMichelle Alejo CortezNo ratings yet
- Discuss About TM Malaysia Balance Scrore CardDocument24 pagesDiscuss About TM Malaysia Balance Scrore CardSuzana Ithnain100% (2)
- SPH Sabbath and HealthDocument14 pagesSPH Sabbath and HealthFerdy LainsamputtyNo ratings yet