You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Clinical BacteriologyDocument123 pagesClinical Bacteriologykurotsukki todoroki100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Igenex PricesDocument2 pagesIgenex Pricesapi-316589352No ratings yet
- Inform LetterDocument2 pagesInform LetterMc Suan75% (4)
- Peter's Atlas of Tropical Medicine and Parasitology 7th EdDocument363 pagesPeter's Atlas of Tropical Medicine and Parasitology 7th EdMarcus MvmNo ratings yet
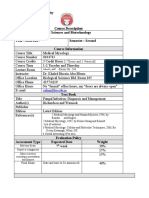
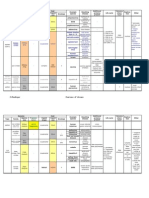
- The Hashemite University Faculty of Science: Salma@hu - Edu.joDocument3 pagesThe Hashemite University Faculty of Science: Salma@hu - Edu.joOdurNo ratings yet
- Nosocomial InfectionDocument31 pagesNosocomial InfectionDr. Ashish Jawarkar0% (1)
- Pelestarian Tari Tradisional Di Masa Pandemi Melalui Media SosialDocument8 pagesPelestarian Tari Tradisional Di Masa Pandemi Melalui Media SosialJasmine ELanouzieNo ratings yet
- Bioactivity, in Vitro Antimicrobial Properties and Chemical Composition of Selected Bryophytes of BangladeshDocument26 pagesBioactivity, in Vitro Antimicrobial Properties and Chemical Composition of Selected Bryophytes of BangladeshDr. Shaikh Bokhtear UddinNo ratings yet
- IMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSDocument5 pagesIMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSjavelezhNo ratings yet
- Tuberculosis Dissertation TopicsDocument5 pagesTuberculosis Dissertation TopicsCollegePapersWritingServiceWashington100% (1)
- LegionellaDocument17 pagesLegionellaShubham Pareshkumar KadiwalaNo ratings yet
- IcdDocument180 pagesIcdFitri MoraNo ratings yet
- Form 5 ScienceDocument27 pagesForm 5 ScienceNg Lay HoonNo ratings yet
- Human Papillomavirus: Divine Word College of Laoag School of Basic Education High SchoolDocument10 pagesHuman Papillomavirus: Divine Word College of Laoag School of Basic Education High SchoolYzabel MacadangdangNo ratings yet
- Human DiseaseDocument13 pagesHuman DiseaseAvnish BhasinNo ratings yet
- SOP For Validation of Sterility Test Record FormDocument13 pagesSOP For Validation of Sterility Test Record FormSolomonNo ratings yet
- Infectious Diseases of Oral CavityDocument21 pagesInfectious Diseases of Oral CavityhunarsandhuNo ratings yet
- Hepatitis B PDFDocument8 pagesHepatitis B PDFponekNo ratings yet
- Microbiology: OrthomyxovirusDocument3 pagesMicrobiology: OrthomyxovirusJustin TayabanNo ratings yet
- Press Release - Cholera in KampalaDocument2 pagesPress Release - Cholera in KampalaEmma Laura KisaNo ratings yet
- Povidone Iodine Use in Hand Disinfectionskin Preparation and Antiseptic IrrigationDocument12 pagesPovidone Iodine Use in Hand Disinfectionskin Preparation and Antiseptic Irrigationpendekar bodohNo ratings yet
- Communicable Diseases PhilippinesDocument11 pagesCommunicable Diseases Philippinessisjing88510No ratings yet
- Virus TableDocument3 pagesVirus TableFrozenManNo ratings yet
- All About Covid: Daniel Ken Diamante, MDDocument40 pagesAll About Covid: Daniel Ken Diamante, MDDanNo ratings yet
- In Vitro Antimicrobial Potential of Extracts and PDocument14 pagesIn Vitro Antimicrobial Potential of Extracts and PWilliam VolmerNo ratings yet
- Rapha Exam (35 MKS)Document2 pagesRapha Exam (35 MKS)TumabangNo ratings yet
- Livhb 001Document2 pagesLivhb 001alkaNo ratings yet
- Streptococcus ThermophilusDocument4 pagesStreptococcus ThermophilusMeyta Chita II0% (1)
- Summary Notes - Topic 6 Microbiology, Immunity and Forensics - Edexcel (IAL) Biology A-LevelDocument11 pagesSummary Notes - Topic 6 Microbiology, Immunity and Forensics - Edexcel (IAL) Biology A-LevelsalmaNo ratings yet
- Cell Phone Germs Article WORDDocument2 pagesCell Phone Germs Article WORDJack LangstonNo ratings yet