You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- CPG Management of Diabetic FootDocument64 pagesCPG Management of Diabetic Footapalaginih100% (2)
- CancerDocument81 pagesCancerCodered Review100% (1)
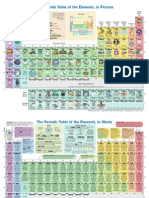
- The Periodic Table of Elements, in PicturesDocument2 pagesThe Periodic Table of Elements, in Picturesrustyy88100% (1)
- Microbiology Lab BookDocument83 pagesMicrobiology Lab BookLavina D'costa100% (6)
- Gross Anatomy and AcupunctureDocument18 pagesGross Anatomy and AcupunctureMiddioPNo ratings yet
- Salter Harris Classification of Growth Plate FracturesDocument13 pagesSalter Harris Classification of Growth Plate FracturesAarón E. CaríasNo ratings yet
- Welcome Speech For Seminar in College 2Document4 pagesWelcome Speech For Seminar in College 2Niño Jay C. GastonesNo ratings yet
- Aplio I700,800,9000 Product DataMPDUS0068EAT - V3.1 - LowDocument28 pagesAplio I700,800,9000 Product DataMPDUS0068EAT - V3.1 - LowAsim Ali100% (1)
- Cytology I - Techniques and Application: Peter NG Cyto Lab Ic, MT, PYNEHDocument201 pagesCytology I - Techniques and Application: Peter NG Cyto Lab Ic, MT, PYNEHbusiness onlyyouNo ratings yet
- Ultrasound in Gynecology and ObstetricsDocument197 pagesUltrasound in Gynecology and ObstetricsAli Murtaza AbbasNo ratings yet
- Physics of Mammography PDFDocument307 pagesPhysics of Mammography PDFBriane Bandeira100% (1)
- 40768-Article Text-143534-1-10-20190327Document3 pages40768-Article Text-143534-1-10-20190327nakibosmanNo ratings yet
- E-Return Filing Sowftware E Env Ii WBQG: (BZZB GKVD U Lvjvi C×WZ)Document10 pagesE-Return Filing Sowftware E Env Ii WBQG: (BZZB GKVD U Lvjvi C×WZ)nakibosmanNo ratings yet
- Pharmaceutical Applications of Isopropyl Alcohol. I. As A Solvent in Pharmaceutical ManufacturingDocument6 pagesPharmaceutical Applications of Isopropyl Alcohol. I. As A Solvent in Pharmaceutical ManufacturingnakibosmanNo ratings yet
- Renewable Ethanol For Beverage and Industrial Uses: A Versatile and High Quality ProductDocument2 pagesRenewable Ethanol For Beverage and Industrial Uses: A Versatile and High Quality ProductnakibosmanNo ratings yet
- Bangabandhu Sheikh Mujib Industrial CityDocument150 pagesBangabandhu Sheikh Mujib Industrial CitynakibosmanNo ratings yet
- Accessing Google Classroom - Student View: Click The + Sign To Join A ClassDocument1 pageAccessing Google Classroom - Student View: Click The + Sign To Join A ClassnakibosmanNo ratings yet
- Argumenta 22 Talia Morag The Tracking Dogma in The Philosophy of EmotionDocument21 pagesArgumenta 22 Talia Morag The Tracking Dogma in The Philosophy of EmotionnakibosmanNo ratings yet
- The Digital Twin Paradigm For Future NASA and U.S. Air Force VehiclesDocument14 pagesThe Digital Twin Paradigm For Future NASA and U.S. Air Force VehiclesnakibosmanNo ratings yet
- Everything You Need To Know About Scientific PublishingDocument11 pagesEverything You Need To Know About Scientific PublishingnakibosmanNo ratings yet
- Yamaha MT-125 OMDocument96 pagesYamaha MT-125 OMnakibosmanNo ratings yet
- Transworld Mercantile Corporation: For Simplified It Solutions!Document6 pagesTransworld Mercantile Corporation: For Simplified It Solutions!nakibosmanNo ratings yet
- Rules of BusinessDocument36 pagesRules of BusinessnakibosmanNo ratings yet
- Daily Productivity ListDocument1 pageDaily Productivity ListnakibosmanNo ratings yet
- National Blockchain Strategy - BangladeshDocument49 pagesNational Blockchain Strategy - BangladeshnakibosmanNo ratings yet
- APPL Company ProfileDocument26 pagesAPPL Company ProfilenakibosmanNo ratings yet
- Khepa NortokDocument98 pagesKhepa NortoknakibosmanNo ratings yet
- CA - Rnip Process Map English PDFDocument1 pageCA - Rnip Process Map English PDFnakibosmanNo ratings yet
- SRO164 Law 2016 26 Customs Passenger (NonTourist) Baggage (Import) Rules 2016AmendedInJune2017Document10 pagesSRO164 Law 2016 26 Customs Passenger (NonTourist) Baggage (Import) Rules 2016AmendedInJune2017ferdous98No ratings yet
- Masud Rana - Beduin Konya PDFDocument100 pagesMasud Rana - Beduin Konya PDFzakaria200811060No ratings yet
- A Study On SME Banking System and Procedure of BRAC Bank LimitedDocument82 pagesA Study On SME Banking System and Procedure of BRAC Bank LimitedShowkatul IslamNo ratings yet
- Significance of Marketing Activities in Garments Industry - A Case Study of BangladeshDocument10 pagesSignificance of Marketing Activities in Garments Industry - A Case Study of BangladeshnakibosmanNo ratings yet
- Argumenta 22 Talia Morag The Tracking Dogma in The Philosophy of EmotionDocument21 pagesArgumenta 22 Talia Morag The Tracking Dogma in The Philosophy of EmotionnakibosmanNo ratings yet
- Dui NumberDocument201 pagesDui NumbernakibosmanNo ratings yet
- Vet Pathol-2004-Nusbaum-453 PDFDocument1 pageVet Pathol-2004-Nusbaum-453 PDFnakibosmanNo ratings yet
- BatDocument14 pagesBatnakibosmanNo ratings yet
- Indian RailwaysDocument19 pagesIndian RailwaysnakibosmanNo ratings yet
- SubwayDocument6 pagesSubwaySteven ChewNo ratings yet
- Demoklin Week 11Document2 pagesDemoklin Week 11Mhaturi Sitti RaoNo ratings yet
- Allegra BrochureDocument14 pagesAllegra BrochureHoracio GomezNo ratings yet
- SOMATOM Definition AS 20 Open - Syngo 2011ADocument28 pagesSOMATOM Definition AS 20 Open - Syngo 2011ASergeyKuznetsovNo ratings yet
- A Glossary: of Key Brain Science TermsDocument24 pagesA Glossary: of Key Brain Science TermscadulemosNo ratings yet
- Evaluation of Ascites and Its Etiology Using Ultrasonography JRD 119 PDFDocument4 pagesEvaluation of Ascites and Its Etiology Using Ultrasonography JRD 119 PDFEstu Paramadina PratamaNo ratings yet
- Lumify EBrochure FNL LR Oct16Document4 pagesLumify EBrochure FNL LR Oct16heryNo ratings yet
- Uk Guidelines SarcomaDocument21 pagesUk Guidelines Sarcomachu_chiang_3No ratings yet
- Informative Essay On My CareerDocument5 pagesInformative Essay On My Careerapi-241280029No ratings yet
- SYSC 4810: Introduction To Network and Software Security Module 2 AssignmentDocument13 pagesSYSC 4810: Introduction To Network and Software Security Module 2 AssignmentAmbar MendezNo ratings yet
- Reiser DBTDocument10 pagesReiser DBTMelanie DascăluNo ratings yet
- WISONIC Ultrasonic Diagnostic System/ 4D Portable Laptop Ultrasound For Obgyn 3 Probe/ Clover 60Document1 pageWISONIC Ultrasonic Diagnostic System/ 4D Portable Laptop Ultrasound For Obgyn 3 Probe/ Clover 60Ririn Dwi LestariNo ratings yet
- REQUISITION: 512-B71017: Qty Item Description Luminos Agile MaxDocument15 pagesREQUISITION: 512-B71017: Qty Item Description Luminos Agile MaxEric MedinaNo ratings yet
- DICOM Conformance Statement FCR Xg1: October, 2000 1st EditionDocument27 pagesDICOM Conformance Statement FCR Xg1: October, 2000 1st EditionNelson J Silva ANo ratings yet
- Sesi 1-Philips-Cecilia MarianaDocument18 pagesSesi 1-Philips-Cecilia MarianaAnonymous I9DsvoSInNo ratings yet
- KaizenDocument19 pagesKaizenJuan David López CifuentesNo ratings yet
- Etiology and Diagnosis of Ascites of Undetermined Origin in A Developing Country: A Prospective StudyDocument9 pagesEtiology and Diagnosis of Ascites of Undetermined Origin in A Developing Country: A Prospective StudyIJAR JOURNALNo ratings yet
- (1479683X - European Journal of Endocrinology) ENDOCRINOLOGY and ADOLESCENCE - Osteoporosis in Children - Diagnosis and ManagementDocument13 pages(1479683X - European Journal of Endocrinology) ENDOCRINOLOGY and ADOLESCENCE - Osteoporosis in Children - Diagnosis and Managementtamaz takidzeNo ratings yet
- The Technologist's Role in CT Protocol Reviews: James M. Kofler, Ph.D. Radiology Mayo Clinic Rochester, MinnesotaDocument33 pagesThe Technologist's Role in CT Protocol Reviews: James M. Kofler, Ph.D. Radiology Mayo Clinic Rochester, MinnesotaNoureddine BenarifaNo ratings yet
- Personal Leadership PhilosophyDocument9 pagesPersonal Leadership PhilosophyNamrah SattarNo ratings yet
- Ms Syllabus Apece DuDocument12 pagesMs Syllabus Apece DuShaikh Hassan AtikNo ratings yet
- EUR 16260 EN European Guidelines On Quality Criteria For Diagnostic Radiographic ImagesDocument98 pagesEUR 16260 EN European Guidelines On Quality Criteria For Diagnostic Radiographic ImagesIKNo ratings yet