You might also like
- Medicine Revision - Neurology TableDocument10 pagesMedicine Revision - Neurology TableUnomoshNo ratings yet
- Severity Assessment Tools For Predicting Mortality in Hospitalised Patients With Community-Acquired Pneumonia. Systematic Review and Meta-AnalysisDocument7 pagesSeverity Assessment Tools For Predicting Mortality in Hospitalised Patients With Community-Acquired Pneumonia. Systematic Review and Meta-AnalysisUnomoshNo ratings yet
- Short-Term Mortality of Adult Inpatients With Community-Acquired Pneumonia - External Validation of A Modified CURB-65 ScoreDocument7 pagesShort-Term Mortality of Adult Inpatients With Community-Acquired Pneumonia - External Validation of A Modified CURB-65 ScoreUnomoshNo ratings yet
- Severity Assessment in Community-Acquired Pneumonia - A ReviewDocument10 pagesSeverity Assessment in Community-Acquired Pneumonia - A ReviewUnomoshNo ratings yet
- Journal of Critical CareDocument5 pagesJournal of Critical CareUnomoshNo ratings yet
- 1 s2.0 S0883944117317537 MainDocument6 pages1 s2.0 S0883944117317537 MainUnomoshNo ratings yet
- Journal of Critical Care: Clinical PotpourriDocument7 pagesJournal of Critical Care: Clinical PotpourriUnomoshNo ratings yet
- Prognostic Value of Pneumonia Severity Index, CURB-65, CRB-65, and Procalcitonin in Community-Acquired Pneumonia in SingaporeDocument9 pagesPrognostic Value of Pneumonia Severity Index, CURB-65, CRB-65, and Procalcitonin in Community-Acquired Pneumonia in SingaporeUnomoshNo ratings yet
- Comparison of Clinical Characteristics and Performance of Pneumonia Severity Score and CURB-65 Among Younger Adults, Elderly and Very Old SubjectsDocument8 pagesComparison of Clinical Characteristics and Performance of Pneumonia Severity Score and CURB-65 Among Younger Adults, Elderly and Very Old SubjectsUnomoshNo ratings yet
- s41598 018 22188 XDocument7 pagess41598 018 22188 XUnomoshNo ratings yet
- Liberalism and Its CriticsDocument13 pagesLiberalism and Its CriticsUnomoshNo ratings yet
- The Cardiac CycleDocument1 pageThe Cardiac CycleUnomoshNo ratings yet
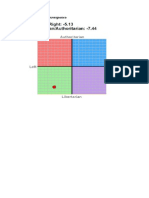
- Political CompassDocument1 pagePolitical CompassUnomoshNo ratings yet
- Terrorism Justification and IllusionDocument16 pagesTerrorism Justification and IllusionUnomoshNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Periodic Test in MAPEHDocument5 pagesPeriodic Test in MAPEHRudyard MoranteNo ratings yet
- Isolasi Fungi EndofitDocument15 pagesIsolasi Fungi EndofitZayyin WardiahNo ratings yet
- Rabies Health TalkDocument10 pagesRabies Health TalkAmit Ranjan100% (1)
- Mh-Somatic Symptom Disorders - 2Document9 pagesMh-Somatic Symptom Disorders - 2martinNo ratings yet
- What Is Evidence Based PracticeDocument5 pagesWhat Is Evidence Based PracticessppNo ratings yet
- CHAPTER 25 (Ergogenic Aids)Document44 pagesCHAPTER 25 (Ergogenic Aids)Muhammad AidibNo ratings yet
- Sip - RanhsDocument4 pagesSip - RanhsimpromtouNo ratings yet
- First Aid in the Chemistry LabDocument2 pagesFirst Aid in the Chemistry LabFrancisJanDillaNo ratings yet
- Health Sectors Governing Healthcare SystemDocument67 pagesHealth Sectors Governing Healthcare SystemSJO1 G6- Escaro,Shaira JoyNo ratings yet
- 90% Nutrition Quiz ScoreDocument4 pages90% Nutrition Quiz ScorextremedaysNo ratings yet
- Tonsillitis Treatment and Home RemediesDocument6 pagesTonsillitis Treatment and Home RemediesAnonymous UzWZrQU2kNNo ratings yet
- Complementary and supplementary feeding essentialsDocument23 pagesComplementary and supplementary feeding essentialsArchana100% (1)
- Order of DrawDocument1 pageOrder of Drawimmuno ser100% (3)
- Diabetes Mellitus e ComplicaçõesDocument12 pagesDiabetes Mellitus e ComplicaçõesDouglas OliveiraNo ratings yet
- Circular Covid-19 Measures: INCO International Fz. Co. ح م ش ﺔﯾﻟودﻟا وﻛﻧاDocument2 pagesCircular Covid-19 Measures: INCO International Fz. Co. ح م ش ﺔﯾﻟودﻟا وﻛﻧاErin JohnsonNo ratings yet
- QuestionsDocument19 pagesQuestionsFatma AlbakoushNo ratings yet
- List of Important Medicinal Plants - Uses of Medicinal PlantDocument5 pagesList of Important Medicinal Plants - Uses of Medicinal PlantmusafirwandererNo ratings yet
- Seminar: Epidemiology and Disease BurdenDocument15 pagesSeminar: Epidemiology and Disease BurdenLuis Miguel Murcia CastilloNo ratings yet
- The Psychological Aspects of "A Beautiful Mind"Document12 pagesThe Psychological Aspects of "A Beautiful Mind"Azba Butt0% (1)
- Case Presentation OB - GYNDocument14 pagesCase Presentation OB - GYNRaidah Ayesha RazackNo ratings yet
- Medicin All Nov, Sep, OctDocument98 pagesMedicin All Nov, Sep, OctMohammad BanisalmanNo ratings yet
- 02AdvancedThinkAhead3 Term2 TL2Document4 pages02AdvancedThinkAhead3 Term2 TL2natachaNo ratings yet
- ENGLISHDocument22 pagesENGLISHears bonifacioNo ratings yet
- The Rules of The Cancer Patient Diet and Dr. Hammer GNMDocument71 pagesThe Rules of The Cancer Patient Diet and Dr. Hammer GNMshivapuja100% (1)
- MSQ. Oral Pathology. Dr. Hiwa KareemDocument13 pagesMSQ. Oral Pathology. Dr. Hiwa KareemAmmar YasirNo ratings yet
- 2010 Nigeria Federal Budget ProposalDocument69 pages2010 Nigeria Federal Budget ProposalDon Pim PimNo ratings yet
- WHO EHC 240 Eng PDFDocument752 pagesWHO EHC 240 Eng PDFopenid_mRbxHxDC100% (1)
- Papilloma Skuamosa: Laporan Kasus Dan Tinjauan PustakaDocument4 pagesPapilloma Skuamosa: Laporan Kasus Dan Tinjauan PustakarizkyayuarristaNo ratings yet
- TOC Prof Chintamanis Comprehensive Book On SurgeryDocument4 pagesTOC Prof Chintamanis Comprehensive Book On SurgeryKoustav ChakrabortyNo ratings yet
- Analgesics - Uses, Treatment, RisksDocument5 pagesAnalgesics - Uses, Treatment, RisksHonour JamesNo ratings yet