You might also like
- Unvf Application Form InstructionsDocument4 pagesUnvf Application Form InstructionsfieqaNo ratings yet
- TOC Template2014Document1 pageTOC Template2014ujononoNo ratings yet
- Room As Signac Adem FeaturesDocument1 pageRoom As Signac Adem FeaturesujononoNo ratings yet
- Sample CV 5Document1 pageSample CV 5SynchronizeNo ratings yet
- Loan Proposal TmeplateDocument4 pagesLoan Proposal TmeplateujononoNo ratings yet
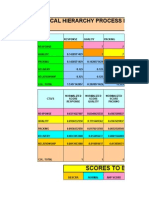
- Ahp Matrix TemplateDocument55 pagesAhp Matrix TemplateavhanNo ratings yet
- CorelDRAW Graphics Suite X7Document1 pageCorelDRAW Graphics Suite X7ujononoNo ratings yet
- Titlepage Project 001 Winter2015Document1 pageTitlepage Project 001 Winter2015ujononoNo ratings yet
- Mawapres AhpDocument14 pagesMawapres AhpHanny Indri HapsariNo ratings yet
- Serial Windows LindoDocument7 pagesSerial Windows LindoujononoNo ratings yet
- Lebarl Kol - FixDocument9 pagesLebarl Kol - FixujononoNo ratings yet
- WD Spectools Word Sample 04Document9 pagesWD Spectools Word Sample 04api-318461273No ratings yet
- Tebal - FixDocument9 pagesTebal - FixujononoNo ratings yet
- Tebal - FixDocument9 pagesTebal - FixujononoNo ratings yet
- 1 XHFSDHDDocument1 page1 XHFSDHDujononoNo ratings yet
- Book 1 BLJGJDocument1 pageBook 1 BLJGJujononoNo ratings yet
- Abstr AksDocument1 pageAbstr AksujononoNo ratings yet
- Photoshop CS5 Read MeDocument11 pagesPhotoshop CS5 Read Meali_mohammed_18No ratings yet
- Lamp IranDocument1 pageLamp IranujononoNo ratings yet
- Pee 03 b2c e CommerceDocument33 pagesPee 03 b2c e CommerceujononoNo ratings yet
- IEEE Outline FormatDocument3 pagesIEEE Outline FormatAlex HerrmannNo ratings yet
- E Jadwal Kuliah Genap 20132014 Ind 11 FebDocument117 pagesE Jadwal Kuliah Genap 20132014 Ind 11 FebujononoNo ratings yet
- IEEE Outline FormatDocument3 pagesIEEE Outline FormatAlex HerrmannNo ratings yet
- 11 Chapter 7 Genetic Disorders PDFDocument8 pages11 Chapter 7 Genetic Disorders PDFwienslaw5804No ratings yet
- Jurnal Risk Assesment3Document7 pagesJurnal Risk Assesment3ujononoNo ratings yet
- Table of Genetic DisordersDocument3 pagesTable of Genetic DisordersujononoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ka Shen Level 2Document26 pagesKa Shen Level 2Volkan VVolkan100% (3)
- Sessions 4 - 2023Document13 pagesSessions 4 - 2023Chen ZhonghaoNo ratings yet
- Download Pathophysiology The Biologic Basis For Disease In Adults And Children Kathryn L Mccance Sue E Huether 2019 8Th Ed 8Th Edition Pathophysiology The Biologic Basis For Disease In Adults And Children full chapter pdf scribdDocument68 pagesDownload Pathophysiology The Biologic Basis For Disease In Adults And Children Kathryn L Mccance Sue E Huether 2019 8Th Ed 8Th Edition Pathophysiology The Biologic Basis For Disease In Adults And Children full chapter pdf scribdjames.bishop563100% (3)
- Wislowska-Stanek - Neurobiological Basis of Increased Risk For Suicidal Behaviour - 2021Document16 pagesWislowska-Stanek - Neurobiological Basis of Increased Risk For Suicidal Behaviour - 2021dojabrNo ratings yet
- Transcript of Chris Wark's ''Square One'' Cancer-Coaching ProgramDocument229 pagesTranscript of Chris Wark's ''Square One'' Cancer-Coaching ProgramArtan100% (11)
- Why Your DNA Isn T Your DestinyDocument75 pagesWhy Your DNA Isn T Your Destinywasabi999No ratings yet
- Occupational Skin Cancer and Precancerous LesionsDocument9 pagesOccupational Skin Cancer and Precancerous LesionsAnonymous 7g5UghNo ratings yet
- Valproic Acid and Epilepsy: From Molecular Mechanisms To Clinical EvidencesDocument21 pagesValproic Acid and Epilepsy: From Molecular Mechanisms To Clinical EvidencesRiki AntoNo ratings yet
- Biochem 442 Ruohola-Baker Midterm 2Document18 pagesBiochem 442 Ruohola-Baker Midterm 2bpwalshNo ratings yet
- Eukaryotic ChromosomeDocument94 pagesEukaryotic ChromosomeRtNo ratings yet
- SasdsadsaDocument11 pagesSasdsadsaJorge MariaNo ratings yet
- Mindfulness Based Stress Reduction: An Integrated View of Physiological and Molecular Aspects of Mindfulness Intervention On Stress ManagementDocument14 pagesMindfulness Based Stress Reduction: An Integrated View of Physiological and Molecular Aspects of Mindfulness Intervention On Stress ManagementajmrdNo ratings yet
- Sexual Assault and Intimate Partner Violence: July 2018Document11 pagesSexual Assault and Intimate Partner Violence: July 2018Duygu ÜzülmezNo ratings yet
- DEVPSY Reviewer - Chapters 1-6 PDFDocument19 pagesDEVPSY Reviewer - Chapters 1-6 PDFKathleen Anica SahagunNo ratings yet
- ABELHADocument5 pagesABELHAPatrick MarquesNo ratings yet
- Neurobiological Basis SuicideDocument476 pagesNeurobiological Basis SuicideEva100% (2)
- Bevan, T. (2015) - The Psychobiology of Transsexualism and Transgenderism. A New View Based On Scientific Evidence PDFDocument280 pagesBevan, T. (2015) - The Psychobiology of Transsexualism and Transgenderism. A New View Based On Scientific Evidence PDFDavid Ostoa100% (3)
- UNIT 2 (Unfinished)Document22 pagesUNIT 2 (Unfinished)青木ケイNo ratings yet
- Hertz-Picciotto Et Al. 2018Document33 pagesHertz-Picciotto Et Al. 2018Celeste ReyNo ratings yet
- Working Memory, Long-Term Memory, and Instructional DesignDocument8 pagesWorking Memory, Long-Term Memory, and Instructional DesignPablo RuisotoNo ratings yet
- Hasler 2015Document32 pagesHasler 2015Seplou7iNo ratings yet
- Plant - Pathogen Interaction & Disease Development - ppt-2003Document91 pagesPlant - Pathogen Interaction & Disease Development - ppt-2003lordniklaus100% (6)
- Perceptions of EpigeneticsDocument3 pagesPerceptions of Epigeneticsapi-20009652No ratings yet
- Genetics Analysis and Principles 7Th Edition Brooker Full ChapterDocument51 pagesGenetics Analysis and Principles 7Th Edition Brooker Full Chapterwilliam.shaw138100% (17)
- BioSysBio 2008 Conference Full ScheduleDocument19 pagesBioSysBio 2008 Conference Full ScheduleA Roy100% (2)
- Book-Nutrigenomics 1stpreviewDocument24 pagesBook-Nutrigenomics 1stpreviewCarlos Alberto dos Santos -VHA-Vilhena-Eeef Cecilia MeirelesNo ratings yet
- 2018 Year 11 Human Biology ATAR Course OutlineDocument21 pages2018 Year 11 Human Biology ATAR Course OutlineNessrynNo ratings yet
- Plastic Surgery Persuasive EssayDocument4 pagesPlastic Surgery Persuasive Essayezm8kqbt100% (2)
- Brochure RoyalEpigen P5Document12 pagesBrochure RoyalEpigen P5Julia BottiniNo ratings yet
- Wolstenholme Et Al. (2011)Document10 pagesWolstenholme Et Al. (2011)DaBid Lopez RodriguezNo ratings yet