You might also like
- Motivation LetterDocument2 pagesMotivation Lettercho carl83% (18)
- More 2 Teacher Book PDFDocument98 pagesMore 2 Teacher Book PDFHuyen Mi100% (2)
- The Day The Crayons Quit-FpdDocument6 pagesThe Day The Crayons Quit-Fpdapi-360143529No ratings yet
- Write Psychology Report SectionsDocument4 pagesWrite Psychology Report SectionsHrithikNo ratings yet
- Early Childhood Philosophy: Amierah Izzati Aisyah Binti Mohd Nazri Lhekkah A/P Sivaraja EDU3013Document8 pagesEarly Childhood Philosophy: Amierah Izzati Aisyah Binti Mohd Nazri Lhekkah A/P Sivaraja EDU3013AmierahIzzatiAisyahNo ratings yet
- Boala Ca SansaDocument561 pagesBoala Ca Sansavaraastadsd94% (34)
- 1994Document200 pages1994Dallas County R-I SchoolsNo ratings yet
- Children Who Are Anxious in Silent - A Review of Selective MutismDocument19 pagesChildren Who Are Anxious in Silent - A Review of Selective MutismNicole WilliamsNo ratings yet
- Mutism SelectivDocument30 pagesMutism SelectivAurelia BartaNo ratings yet
- Three Tiered Interventions For Selective MutismDocument12 pagesThree Tiered Interventions For Selective MutismDiana CarreiraNo ratings yet
- What Is Selective Mutism (SM) ?Document9 pagesWhat Is Selective Mutism (SM) ?Rishabh Kapoor100% (1)
- Selective Mutism Research Paper FinalDocument14 pagesSelective Mutism Research Paper Finalapi-260124422No ratings yet
- Selective Mutism Hadeel Alawna Psychiatry CourseDocument8 pagesSelective Mutism Hadeel Alawna Psychiatry CourseHadeel AlawnaNo ratings yet
- Anxiety Disorders Selective Mutism and Specific PhobiaDocument8 pagesAnxiety Disorders Selective Mutism and Specific PhobiaIQRA YOUSAFNo ratings yet
- My Selective MutismDocument18 pagesMy Selective MutismMichelle DaquelNo ratings yet
- Selective Mutism QuestionnaireDocument2 pagesSelective Mutism QuestionnaireLidia RiveraNo ratings yet
- Edte 500 Inquiry PresentationDocument14 pagesEdte 500 Inquiry Presentationapi-506099136No ratings yet
- Character Traits LessonDocument4 pagesCharacter Traits Lessonapi-355793629No ratings yet
- Character Traits Lesson PlanDocument5 pagesCharacter Traits Lesson Planapi-376373807No ratings yet
- Selective mutism-DSM-5-233-235Document3 pagesSelective mutism-DSM-5-233-235Mella IntaniabellaNo ratings yet
- What Is Your Learning Style?: A Theoretical Study On Various Learning Style Models and Assessment Techniques To Evaluate Students Learning Styles For The Multimedia Supported E-Learning EnvironmentDocument5 pagesWhat Is Your Learning Style?: A Theoretical Study On Various Learning Style Models and Assessment Techniques To Evaluate Students Learning Styles For The Multimedia Supported E-Learning EnvironmentMohamed Iqubal Jawid NazirNo ratings yet
- Selective Mutism in Children: An Extract From Porter, L. (2008) - Young Children's Behaviour, (3 Ed.) Sydney, ElsevierDocument4 pagesSelective Mutism in Children: An Extract From Porter, L. (2008) - Young Children's Behaviour, (3 Ed.) Sydney, ElsevierEvelyn BongalonNo ratings yet
- UDL Guidelines Checklist PDFDocument8 pagesUDL Guidelines Checklist PDFShahida RehmanNo ratings yet
- Career and Multiple IntelligencesDocument7 pagesCareer and Multiple IntelligencesmindoflightNo ratings yet
- Beyond Shyness:: Evidence Based Assessment and Intervention For Selective MutismDocument37 pagesBeyond Shyness:: Evidence Based Assessment and Intervention For Selective MutismIbtisam Marohombsar AlontoNo ratings yet
- Selective Mutism HandoutDocument2 pagesSelective Mutism Handoutapi-302847539100% (1)
- Elective MutismDocument5 pagesElective MutismMAHIMA DASNo ratings yet
- Selective MutismDocument4 pagesSelective MutismMartina SafitryNo ratings yet
- Theory of Mind: An Observational ReportDocument3 pagesTheory of Mind: An Observational ReportMalavika MenonNo ratings yet
- Selective Mutism-For SchoolDocument4 pagesSelective Mutism-For SchoolJeanrose AlavataNo ratings yet
- Selective Mutism, Causes and InterventionsDocument8 pagesSelective Mutism, Causes and InterventionsMartha TriviñoNo ratings yet
- How Is Selective Mutism DiagnosedDocument13 pagesHow Is Selective Mutism DiagnosedFaizal Amiz100% (2)
- Developing Prosocial Skills in ChildrenDocument3 pagesDeveloping Prosocial Skills in ChildrenGretz DoriaNo ratings yet
- Improving Theory of Mind FinalDocument15 pagesImproving Theory of Mind FinalAnnick ComblainNo ratings yet
- Early Intervention Preschool Research/Process WorkDocument43 pagesEarly Intervention Preschool Research/Process WorkMurphy C0% (1)
- English Language Learners - Problems and Solutions Found in The Research of General Practitioners of Early ChildhoodDocument7 pagesEnglish Language Learners - Problems and Solutions Found in The Research of General Practitioners of Early ChildhoodThirupathi KNo ratings yet
- Interactive Storybook Reading - Making The Classroom Read-Aloud Program A Meaningful Learning Experience-2Document8 pagesInteractive Storybook Reading - Making The Classroom Read-Aloud Program A Meaningful Learning Experience-2api-253180182No ratings yet
- The Rabbits Lesson 2Document2 pagesThe Rabbits Lesson 2api-383417172100% (1)
- Cultural DiversityDocument7 pagesCultural Diversityapi-378042907No ratings yet
- Alfred Adler: Alfred Adler Proposed The Concept of The Inferiority ComplexDocument5 pagesAlfred Adler: Alfred Adler Proposed The Concept of The Inferiority ComplexJayzel Joy JuanicoNo ratings yet
- VygotskyDocument15 pagesVygotskyparasvarmaNo ratings yet
- Boosting Confidence Through Self-AwarenessDocument55 pagesBoosting Confidence Through Self-AwarenessShaznay AlomiaNo ratings yet
- Play Therapy MenassaDocument15 pagesPlay Therapy MenassaNur Hidayah DaniNo ratings yet
- Career Day Parent LetterDocument2 pagesCareer Day Parent Letterapi-233314088No ratings yet
- Benefits of Children's LiteratureDocument3 pagesBenefits of Children's LiteratureRaji musharafNo ratings yet
- Lit Pro KsmithDocument17 pagesLit Pro Ksmithapi-508873679No ratings yet
- Learning StylesDocument27 pagesLearning StylesAnjanagrace100% (2)
- CBS StudentIdentityDocument4 pagesCBS StudentIdentityWilliam BuquiaNo ratings yet
- Development Matters Statements Ages and StagesDocument6 pagesDevelopment Matters Statements Ages and StagesAye Thanda TheinNo ratings yet
- Helping Your Child With Selective Mutism: Practical Steps To Overcome A Fear of Speaking - Angela E. McHolmDocument4 pagesHelping Your Child With Selective Mutism: Practical Steps To Overcome A Fear of Speaking - Angela E. McHolmbunefoboNo ratings yet
- Reflective Lesson Plan Main IdeaDocument6 pagesReflective Lesson Plan Main Ideanscmanigault100% (1)
- Expressive Language (Using Words and Language) : Print PDFDocument8 pagesExpressive Language (Using Words and Language) : Print PDFNico Corporal CañaveralNo ratings yet
- How Identity Impacts Child Self-EsteemDocument3 pagesHow Identity Impacts Child Self-Esteemiteachfromheart100% (1)
- Molloy College Division of Education Lesson Plan #1 Instructional ObjectiveDocument12 pagesMolloy College Division of Education Lesson Plan #1 Instructional Objectiveapi-348193829100% (1)
- Japanese ValuesDocument13 pagesJapanese ValuesAko Si ChokeyNo ratings yet
- Theories On Language Learning - Vygotsky, Piaget, & Habit FormationDocument30 pagesTheories On Language Learning - Vygotsky, Piaget, & Habit FormationShofia NafisahNo ratings yet
- Notable Books For A Global Society ProjectDocument49 pagesNotable Books For A Global Society Projectapi-488579854No ratings yet
- EriksonDocument17 pagesEriksonAnonymous 3fDD3BNo ratings yet
- Tall Tale Lesson Final GradeDocument12 pagesTall Tale Lesson Final Gradeapi-300370981No ratings yet
- A Culturally-Inclusive Classroom EnvironmentDocument3 pagesA Culturally-Inclusive Classroom EnvironmentAlexana Bi VieNo ratings yet
- Joint Attention and Disorganized Attachment Status in Infants at RiskDocument14 pagesJoint Attention and Disorganized Attachment Status in Infants at RiskCarolina Saavedra MellaNo ratings yet
- Stanescu Romer Pirosca 20fullDocument10 pagesStanescu Romer Pirosca 20fullMary Jelyn Kate GatlabayanNo ratings yet
- Abnoramlities in Efferent Activities MutismDocument9 pagesAbnoramlities in Efferent Activities MutismlaviNo ratings yet
- MutismDocument56 pagesMutismlaviNo ratings yet
- Mutism 1Document23 pagesMutism 1laviNo ratings yet
- Selective Mutism Treatment Case SamplesDocument18 pagesSelective Mutism Treatment Case SampleslaviNo ratings yet
- Abnoramlities in Efferent Activities MutismDocument9 pagesAbnoramlities in Efferent Activities MutismlaviNo ratings yet
- Selective Mutism - VianaDocument11 pagesSelective Mutism - VianalaviNo ratings yet
- MutismDocument10 pagesMutismlaviNo ratings yet
- p91 PDFDocument10 pagesp91 PDFRisfikawati RiskalNo ratings yet
- Abnoramlities in Efferent Activities MutismDocument9 pagesAbnoramlities in Efferent Activities MutismlaviNo ratings yet
- MutismDocument56 pagesMutismlaviNo ratings yet
- Mutism 1Document23 pagesMutism 1laviNo ratings yet
- Mutism 1Document23 pagesMutism 1laviNo ratings yet
- 6 Hrs Agreement FormDocument3 pages6 Hrs Agreement FormLougiebelle DimaanoNo ratings yet
- Straight To The Point Evaluation of IEC Materials PDFDocument2 pagesStraight To The Point Evaluation of IEC Materials PDFHasan NadafNo ratings yet
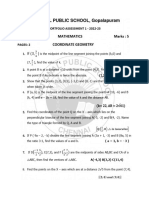
- G10 - Portfolio Assessment 1 - 2022-2023Document2 pagesG10 - Portfolio Assessment 1 - 2022-2023ayush rajeshNo ratings yet
- Jncip EntDocument4 pagesJncip Entreal_mc0% (2)
- Examining Conflicts and Sharing Ideas in Panel DiscussionsDocument4 pagesExamining Conflicts and Sharing Ideas in Panel DiscussionsOfficial Lara Delos SantosNo ratings yet
- WQuest Itools 2 Tests 5Document1 pageWQuest Itools 2 Tests 5Magdalena QuirogaNo ratings yet
- Managing The Primary Classroom: - How Physical Class Environment Contribute To Effective LessonDocument16 pagesManaging The Primary Classroom: - How Physical Class Environment Contribute To Effective LessonJannah AziziNo ratings yet
- Cyber Security RoadmapDocument7 pagesCyber Security RoadmapNavin Kumar PottavathiniNo ratings yet
- Newsletter 201003Document23 pagesNewsletter 201003Tim LinNo ratings yet
- Shabnam Mehrtash, Settar Koçak, Irmak Hürmeriç Altunsöz: Hurmeric@metu - Edu.trDocument11 pagesShabnam Mehrtash, Settar Koçak, Irmak Hürmeriç Altunsöz: Hurmeric@metu - Edu.trsujiNo ratings yet
- Davao Medical School Foundation, Inc. BS in Nursing Curriculum (Prospectus)Document1 pageDavao Medical School Foundation, Inc. BS in Nursing Curriculum (Prospectus)吉永 いりかNo ratings yet
- Lamm, J. Schleiermacher's PlatoDocument278 pagesLamm, J. Schleiermacher's PlatonicodeloNo ratings yet
- Basketball Prison Ball Lesson PlansDocument4 pagesBasketball Prison Ball Lesson Plansapi-273012822No ratings yet
- 22 Louise Hay - The List - Affirmations FilteredDocument15 pages22 Louise Hay - The List - Affirmations Filteredch srinivas100% (2)
- Dijelovi Kuće-Radni ListićDocument10 pagesDijelovi Kuće-Radni ListićGise Cerutti Pavić100% (1)
- Lesson PlanDocument10 pagesLesson PlanBUCOY, SHELLEY KAYE R.No ratings yet
- Brief Syllabus in School Administration and SupervisionDocument2 pagesBrief Syllabus in School Administration and SupervisionEingilbert BenoliraoNo ratings yet
- Iitm - MDocument1 pageIitm - Msachin pathakNo ratings yet
- San Jose Community College: College of Arts and SciencesDocument5 pagesSan Jose Community College: College of Arts and SciencesSH ENNo ratings yet
- Simulations A Tool For Testing Virtual Reality in The Language ClassroomDocument10 pagesSimulations A Tool For Testing Virtual Reality in The Language ClassroomSyed Qaiser HussainNo ratings yet
- Deductive ReasoningDocument2 pagesDeductive ReasoningLorenzo B. FollosoNo ratings yet
- Dapat na Pagtuturo sa Buhangin Central Elementary SchoolDocument14 pagesDapat na Pagtuturo sa Buhangin Central Elementary SchoolKATHLEEN CRYSTYL LONGAKITNo ratings yet
- Weekly Report, Literature Meeting 2Document2 pagesWeekly Report, Literature Meeting 2Suzy NadiaNo ratings yet
- Table of Specification (TOS)Document2 pagesTable of Specification (TOS)Charlene FiguracionNo ratings yet
- (ACV-S06) Week 06 - Pre-Task - Quiz - Weekly Quiz (PA) - INGLES IV (36824)Document5 pages(ACV-S06) Week 06 - Pre-Task - Quiz - Weekly Quiz (PA) - INGLES IV (36824)Gianfranco Riega galarzaNo ratings yet
- Grade 7 - 10 Class Program Sy 2022 2023Document4 pagesGrade 7 - 10 Class Program Sy 2022 2023Niel Marc TomasNo ratings yet
- Phobia Release in Five DaysDocument32 pagesPhobia Release in Five DaysMoi100% (8)