You might also like
- Dental AmalgamDocument34 pagesDental Amalgamفیضان حنیف0% (2)
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionFrom EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNo ratings yet
- Single Visit ClassDocument42 pagesSingle Visit ClassNandita HegdeNo ratings yet
- Endo Perio LesionsDocument24 pagesEndo Perio LesionsAneen Suresh0% (1)
- Access Cavity PreparationDocument35 pagesAccess Cavity PreparationShaheen Aboobacker Reniya ShaheenNo ratings yet
- Diagnosis of Dental CariesDocument35 pagesDiagnosis of Dental CariesKanika MalikNo ratings yet
- Conservative DentistryDocument13 pagesConservative DentistryFoysal SirazeeNo ratings yet
- Deepthi Smear Layer PresentationDocument69 pagesDeepthi Smear Layer PresentationHari Priya100% (2)
- Cavity Designs For Composite RestorationsDocument20 pagesCavity Designs For Composite RestorationsAditi Chandra0% (5)
- Recent Advances in Pulp Vitality TestingDocument6 pagesRecent Advances in Pulp Vitality Testingatul_singh2001No ratings yet
- Rationale of Endodontic TreatmentDocument45 pagesRationale of Endodontic TreatmentAmy Rita0% (1)
- S - 10 Direct Filling GoldDocument30 pagesS - 10 Direct Filling GoldShaliniNo ratings yet
- Forces Acting On Restorations LD / Orthodontic Courses by Indian Dental AcademyDocument95 pagesForces Acting On Restorations LD / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Post and Core IngleDocument29 pagesPost and Core IngleChintan MakadiaNo ratings yet
- Diseases of PulpDocument81 pagesDiseases of PulpDrMohit Sharma100% (1)
- Biologic Considerations of Enamel Structure and Its Clinical Significance in Practice of Operative DentistryDocument25 pagesBiologic Considerations of Enamel Structure and Its Clinical Significance in Practice of Operative DentistryNofal MundathoduNo ratings yet
- Tests For Biocompatibility of Dental MaterialsDocument151 pagesTests For Biocompatibility of Dental MaterialsDevanshi SharmaNo ratings yet
- Managementofnoncariouslesions 140228135843 Phpapp01Document145 pagesManagementofnoncariouslesions 140228135843 Phpapp01Anoop maniNo ratings yet
- Non Carious Lesions and Their ManagementDocument47 pagesNon Carious Lesions and Their ManagementDrApplu Atrey50% (2)
- Diseases of Periradicular TissuesDocument62 pagesDiseases of Periradicular Tissuesanubhutigupta1404No ratings yet
- Regen EndoDocument88 pagesRegen EndoJitender ReddyNo ratings yet
- Cavosurface Treatment of Various RestorationDocument29 pagesCavosurface Treatment of Various RestorationRimjhim JainNo ratings yet
- Fundamentals of Aesthetic DentistryDocument5 pagesFundamentals of Aesthetic Dentistryladzville1014860No ratings yet
- Non Carious LesionsDocument23 pagesNon Carious LesionsDuaa M. Salah100% (1)
- Cervical LesionsDocument135 pagesCervical Lesionsrasagna reddyNo ratings yet
- Calcium Hydroxide in DentistryDocument17 pagesCalcium Hydroxide in DentistryTarek RabiNo ratings yet
- Dental PulpDocument77 pagesDental PulpJyoti RahejaNo ratings yet
- Role of Saliva in Dental CariesDocument29 pagesRole of Saliva in Dental Carieskhush sidhu100% (1)
- Mod 6 Cavity NomenclatureDocument26 pagesMod 6 Cavity NomenclatureVinceEjorangoCabigaoNo ratings yet
- Management of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearDocument44 pagesManagement of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearANUBHANo ratings yet
- DIAGNOSTIC METHODS (Emphasis On Recent Advances) IN EndodonticsDocument51 pagesDIAGNOSTIC METHODS (Emphasis On Recent Advances) IN EndodonticsKalpesh DeyNo ratings yet
- Regenerative Endodontics Part 2Document118 pagesRegenerative Endodontics Part 2rasagna reddyNo ratings yet
- Lasers Used in Operative Dentistry and EndodonticsDocument28 pagesLasers Used in Operative Dentistry and EndodonticsNingombam Robinson Singh0% (1)
- Final PDLDocument100 pagesFinal PDLDrRahat SaleemNo ratings yet
- Rotary EndodonticsDocument61 pagesRotary EndodonticsVijayendra kamathNo ratings yet
- Access Cavity Preparation FinalDocument63 pagesAccess Cavity Preparation Finalrasagna reddyNo ratings yet
- Recent Advances in Composites PDFDocument7 pagesRecent Advances in Composites PDFShriya Shahu100% (1)
- New Microsoft PowerPoint PresentationDocument158 pagesNew Microsoft PowerPoint PresentationSutapa Roy100% (1)
- Maxillary Nerve: Dr. Sanjana Mall Department of PedodonticsDocument48 pagesMaxillary Nerve: Dr. Sanjana Mall Department of PedodonticsSanjana MallNo ratings yet
- Obturation TechniquesDocument33 pagesObturation TechniquesLAKSHMI ARORANo ratings yet
- Non Carious LesionsDocument38 pagesNon Carious LesionsDrVarun Menon75% (4)
- Kaloji Narayana Rao University of Health Sciences, Warangal, Telangana - 506007Document9 pagesKaloji Narayana Rao University of Health Sciences, Warangal, Telangana - 506007Sriram KasturiNo ratings yet
- Physical Properties of Dental MaterialsDocument87 pagesPhysical Properties of Dental MaterialsManiBernardH100% (1)
- Direct Filling GoldDocument49 pagesDirect Filling Goldjtsnthkrl0% (2)
- 6 Restorationoftheendodonticallytreatedtooth 101219205957 Phpapp02Document100 pages6 Restorationoftheendodonticallytreatedtooth 101219205957 Phpapp02JASPREETKAUR0410100% (1)
- Complications of ExodontiaDocument33 pagesComplications of ExodontiaSunil TiwariNo ratings yet
- Restoration of Endodontically Treated TeethDocument7 pagesRestoration of Endodontically Treated TeethCattleya Tanosselo100% (1)
- 5 EndodonticsDocument38 pages5 EndodonticsHaryanto Haryanto Haryanto100% (1)
- Periodontium (2) - Gingiva: Microscopic Features of GingivaDocument8 pagesPeriodontium (2) - Gingiva: Microscopic Features of Gingivaمحمد محمود القحيفNo ratings yet
- Disinfection of The Root CanalDocument45 pagesDisinfection of The Root CanalSachin B Mangalekar100% (1)
- Cavity Liners and Bases 2Document9 pagesCavity Liners and Bases 2hp1903No ratings yet
- Denture Base ResinsDocument70 pagesDenture Base ResinsSusovan Giri100% (1)
- Biocompatibility of Dental MaterialsDocument21 pagesBiocompatibility of Dental Materialsindian dental academyNo ratings yet
- Tarnish - CorrosionDocument18 pagesTarnish - CorrosionAmniAzmiNo ratings yet
- Introduction Cysts of JawsDocument62 pagesIntroduction Cysts of JawsFatima Siddiqui100% (1)
- Success& Failures in EndoDocument32 pagesSuccess& Failures in Endorasagna reddyNo ratings yet
- Developmental Disturbances of TeethDocument45 pagesDevelopmental Disturbances of TeethAmritha JamesNo ratings yet
- 1 EnamelDocument40 pages1 EnamelHarshvardhanNo ratings yet
- Traumatic Injuries Notes 22nk8pfDocument16 pagesTraumatic Injuries Notes 22nk8pfAmee PatelNo ratings yet
- Dental Caries and Restorative Dentsitry (Autosaved)Document24 pagesDental Caries and Restorative Dentsitry (Autosaved)Subhashini RajshekarNo ratings yet
- Developmentofocclusion 140219113507 Phpapp01 150817175152 Lva1 App6891Document96 pagesDevelopmentofocclusion 140219113507 Phpapp01 150817175152 Lva1 App6891Subhashini RajshekarNo ratings yet
- Growth & DevelopmentDocument74 pagesGrowth & DevelopmentSubhashini RajshekarNo ratings yet
- Development of TeethDocument20 pagesDevelopment of TeethSubhashini RajshekarNo ratings yet
- Indian History PDFDocument188 pagesIndian History PDFNaveed Khan AbbuNo ratings yet
- Oralpatho MCQDocument0 pagesOralpatho MCQkainath0150% (2)
- Case 17Document2 pagesCase 17Ankit GalavNo ratings yet
- Estrogenicity of CompositesDocument8 pagesEstrogenicity of CompositesSubhashini RajshekarNo ratings yet
- General Studies-II Series A KPSCDocument48 pagesGeneral Studies-II Series A KPSCSubhashini RajshekarNo ratings yet
- Hypersensitivity Physio / Orthodontic Courses by Indian Dental AcademyDocument77 pagesHypersensitivity Physio / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Development of Root ApexDocument16 pagesDevelopment of Root ApexSubhashini RajshekarNo ratings yet
- ErgonomicsDocument4 pagesErgonomicsSubhashini RajshekarNo ratings yet
- Longevity of Posterior RestorationsDocument7 pagesLongevity of Posterior RestorationsSubhashini RajshekarNo ratings yet
- Perio-Endo Lesions Clinical Diagnostic Procedure: Submitted by O.R.Ganesh MSD Endo 1 YeraDocument66 pagesPerio-Endo Lesions Clinical Diagnostic Procedure: Submitted by O.R.Ganesh MSD Endo 1 YeraSubhashini RajshekarNo ratings yet
- Microleakage of Amalgam Restorations Associated With Dentin Adhesive, Glass Ionomer Cement and Cavity Varnish by Means of Different Evaluation MethodsDocument5 pagesMicroleakage of Amalgam Restorations Associated With Dentin Adhesive, Glass Ionomer Cement and Cavity Varnish by Means of Different Evaluation MethodsSubhashini RajshekarNo ratings yet
- Effect of Filler Size and Temperature On Packing Stress andDocument9 pagesEffect of Filler Size and Temperature On Packing Stress andSubhashini RajshekarNo ratings yet
- Composite V AmalgamDocument10 pagesComposite V AmalgambryanabauerNo ratings yet
- Dark LesionsDocument9 pagesDark LesionsJamal WadiNo ratings yet
- Lecture Notes - URM UARMDocument54 pagesLecture Notes - URM UARMAragon Palac BacquianoNo ratings yet
- Engine: HMK 102 Energy Workshop ManualDocument20 pagesEngine: HMK 102 Energy Workshop ManualJonathan WENDTNo ratings yet
- Essar Shipping ProjectDocument78 pagesEssar Shipping ProjectvkkothariNo ratings yet
- Ieee C57.135 (2001)Document50 pagesIeee C57.135 (2001)Daniel PaniaguaNo ratings yet
- JBL Sub140p ManualDocument5 pagesJBL Sub140p ManualDiff DonNo ratings yet
- Tps 65160Document28 pagesTps 65160Vukica IvicNo ratings yet
- Physics-Pt With SolutionDocument19 pagesPhysics-Pt With SolutionChris Paul D VarelaNo ratings yet
- 2102 - Vol - 2BDocument7 pages2102 - Vol - 2BSoumen KarNo ratings yet
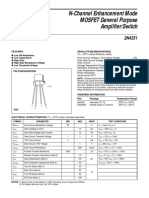
- EMOSFET Nchannel 2N4351Document1 pageEMOSFET Nchannel 2N4351Pradina Kiky WasibagnoNo ratings yet
- Production of Biodiesel From Hybrid Oil Dairy Waste Scum and Karanja and Characterization and Study of Its Performance On Diesel Engine IJERTV3IS070674 PDFDocument5 pagesProduction of Biodiesel From Hybrid Oil Dairy Waste Scum and Karanja and Characterization and Study of Its Performance On Diesel Engine IJERTV3IS070674 PDFManish PatilNo ratings yet
- Lot Inspection Report For LPG New CylindersDocument3 pagesLot Inspection Report For LPG New CylindersJagannath MajhiNo ratings yet
- Type 298 PV100 Medium Voltage IEC Switch Gear and Motor Control Centres 0210Document36 pagesType 298 PV100 Medium Voltage IEC Switch Gear and Motor Control Centres 0210Ryan JayNo ratings yet
- Naya Raipur': A New City Takes RootDocument34 pagesNaya Raipur': A New City Takes Rootrevati chandakNo ratings yet
- LC1044 LRP14 3PH QRG 0823Document2 pagesLC1044 LRP14 3PH QRG 0823FlakooNo ratings yet
- Bangladesh Power Development Board Electricity Bill: LT CONSUMER (Single Register)Document1 pageBangladesh Power Development Board Electricity Bill: LT CONSUMER (Single Register)adfaxfafaea0% (1)
- TTHHDocument4 pagesTTHHHitesh PanigrahiNo ratings yet
- Brandenburg - Genus Spectra CompactDocument2 pagesBrandenburg - Genus Spectra CompactongNo ratings yet
- Geiger Counter Neon LampDocument3 pagesGeiger Counter Neon LampClaudio Oliveira TavaresNo ratings yet
- Manual de Servicio Motores M6 M7 DenisonDocument24 pagesManual de Servicio Motores M6 M7 DenisonaugustoNo ratings yet
- Capacimetre FemtoDocument30 pagesCapacimetre FemtoJean-Marie ChaputNo ratings yet
- Norm-Info-2020-4 (AWS D1)Document2 pagesNorm-Info-2020-4 (AWS D1)Jan-PaulNo ratings yet
- Copeland cr16k6-pfv-875 Article 1377777669266 en SsDocument1 pageCopeland cr16k6-pfv-875 Article 1377777669266 en SsCharli JuseinNo ratings yet
- Heat Exchanger and Chiller Cleaning in PlaceDocument2 pagesHeat Exchanger and Chiller Cleaning in PlaceChris HaslegoNo ratings yet
- DEPA Air Operated Diaphragm PumpsDocument6 pagesDEPA Air Operated Diaphragm Pumpsboom10No ratings yet
- Grid1 - Untitled - gr1S - CompleteRapportDocument3 pagesGrid1 - Untitled - gr1S - CompleteRapportKhaoula BenNo ratings yet
- Condition Assessment of Power Transformers and Assessment IndicesDocument50 pagesCondition Assessment of Power Transformers and Assessment IndicesSKS_2014No ratings yet
- Catalogue2014 PDFDocument158 pagesCatalogue2014 PDFاشرينكيل مسونكيل100% (1)
- Pump AuditDocument5 pagesPump AuditHeri SulasionoNo ratings yet
- EE 465 Lecture 8Document25 pagesEE 465 Lecture 8hshjxcbzNo ratings yet
- Modeling and Parameter Estimation of Synchronous Machine - GR LekhemaDocument33 pagesModeling and Parameter Estimation of Synchronous Machine - GR LekhemaRatoka LekhemaNo ratings yet
- House Rules: How to Decorate for Every Home, Style, and BudgetFrom EverandHouse Rules: How to Decorate for Every Home, Style, and BudgetNo ratings yet
- Crochet Impkins: Over a million possible combinations! Yes, really!From EverandCrochet Impkins: Over a million possible combinations! Yes, really!Rating: 4.5 out of 5 stars4.5/5 (10)
- The Botanical Hand Lettering Workbook: Draw Whimsical & Decorative Styles & ScriptsFrom EverandThe Botanical Hand Lettering Workbook: Draw Whimsical & Decorative Styles & ScriptsRating: 4.5 out of 5 stars4.5/5 (2)
- Crochet Zodiac Dolls: Stitch the horoscope with astrological amigurumiFrom EverandCrochet Zodiac Dolls: Stitch the horoscope with astrological amigurumiRating: 4 out of 5 stars4/5 (3)
- 100 Micro Amigurumi: Crochet patterns and charts for tiny amigurumiFrom Everand100 Micro Amigurumi: Crochet patterns and charts for tiny amigurumiRating: 5 out of 5 stars5/5 (2)
- Modern Granny Stitch Crochet: Make clothes and accessories using the granny stitchFrom EverandModern Granny Stitch Crochet: Make clothes and accessories using the granny stitchRating: 5 out of 5 stars5/5 (1)
- Crochet Pattern Books: The Ultimate Complete Guide to Learning How to Crochet FastFrom EverandCrochet Pattern Books: The Ultimate Complete Guide to Learning How to Crochet FastRating: 5 out of 5 stars5/5 (1)
- The Martha Manual: How to Do (Almost) EverythingFrom EverandThe Martha Manual: How to Do (Almost) EverythingRating: 4 out of 5 stars4/5 (11)
- Celtic Line Drawing - Simplified InstructionsFrom EverandCeltic Line Drawing - Simplified InstructionsRating: 5 out of 5 stars5/5 (4)
- Dream Sewing Spaces: Design & Organization for Spaces Large & SmallFrom EverandDream Sewing Spaces: Design & Organization for Spaces Large & SmallRating: 4 out of 5 stars4/5 (24)
- Timeless Textured Baby Crochet: 20 heirloom crochet patterns for babies and toddlersFrom EverandTimeless Textured Baby Crochet: 20 heirloom crochet patterns for babies and toddlersNo ratings yet
- Crochet Southwest Spirit: Over 20 Bohemian Crochet Patterns Inspired by the American SouthwestFrom EverandCrochet Southwest Spirit: Over 20 Bohemian Crochet Patterns Inspired by the American SouthwestRating: 5 out of 5 stars5/5 (2)
- Crochet with London Kaye: Projects and Ideas to Yarn Bomb Your LifeFrom EverandCrochet with London Kaye: Projects and Ideas to Yarn Bomb Your LifeRating: 5 out of 5 stars5/5 (1)
- Tunisian Crochet for Beginners: Step-by-step Instructions, plus 5 Patterns!From EverandTunisian Crochet for Beginners: Step-by-step Instructions, plus 5 Patterns!Rating: 5 out of 5 stars5/5 (3)
- Friends: The One with the Crochet: The Official Crochet Pattern BookFrom EverandFriends: The One with the Crochet: The Official Crochet Pattern BookRating: 5 out of 5 stars5/5 (1)
- Amigurumi Cats: Crochet Sweet Kitties the Japanese Way (24 Projects of Cats to Crochet)From EverandAmigurumi Cats: Crochet Sweet Kitties the Japanese Way (24 Projects of Cats to Crochet)No ratings yet
- Crochet Creatures of Myth and Legend: 19 Designs Easy Cute Critters to Legendary BeastsFrom EverandCrochet Creatures of Myth and Legend: 19 Designs Easy Cute Critters to Legendary BeastsRating: 4.5 out of 5 stars4.5/5 (10)
- Crochet Collage Garden: 100 patterns for crochet flowers, plants and petalsFrom EverandCrochet Collage Garden: 100 patterns for crochet flowers, plants and petalsRating: 5 out of 5 stars5/5 (1)
- Kawaii Crochet Garden: 40 super cute amigurumi patterns for plants and moreFrom EverandKawaii Crochet Garden: 40 super cute amigurumi patterns for plants and moreRating: 5 out of 5 stars5/5 (5)
- Too Cute Amigurumi: 30 Crochet Patterns for Adorable Animals, Playful Plants, Sweet Treats and MoreFrom EverandToo Cute Amigurumi: 30 Crochet Patterns for Adorable Animals, Playful Plants, Sweet Treats and MoreRating: 5 out of 5 stars5/5 (2)
- Knit Soxx for Everyone: 25 Colorful Sock Patterns for the Whole FamilyFrom EverandKnit Soxx for Everyone: 25 Colorful Sock Patterns for the Whole FamilyRating: 4.5 out of 5 stars4.5/5 (2)
- Crochet Donut Buddies: 50 easy amigurumi patterns for collectible crochet toysFrom EverandCrochet Donut Buddies: 50 easy amigurumi patterns for collectible crochet toysRating: 4.5 out of 5 stars4.5/5 (7)
- Colorful Crochet Knitwear: Crochet sweaters and more with mosaic, intarsia and tapestry crochet patternsFrom EverandColorful Crochet Knitwear: Crochet sweaters and more with mosaic, intarsia and tapestry crochet patternsNo ratings yet
- Radical Sewing: Pattern-Free, Sustainable Fashions for All BodiesFrom EverandRadical Sewing: Pattern-Free, Sustainable Fashions for All BodiesNo ratings yet
- Jane Austen Embroidery: Authentic embroidery projects for modern stitchersFrom EverandJane Austen Embroidery: Authentic embroidery projects for modern stitchersRating: 4 out of 5 stars4/5 (3)
- Two Simple Shapes = 26 Crocheted Cardigans, Tops & Sweaters: If you can crochet a square and rectangle, you can make these easy-to-wear designs!From EverandTwo Simple Shapes = 26 Crocheted Cardigans, Tops & Sweaters: If you can crochet a square and rectangle, you can make these easy-to-wear designs!Rating: 3 out of 5 stars3/5 (2)
- Crochet Lace: Techniques, Patterns, and ProjectsFrom EverandCrochet Lace: Techniques, Patterns, and ProjectsRating: 3.5 out of 5 stars3.5/5 (3)
- The Knotting & Braiding Bible: The Complete Guide to Creative Knotting including Kumihimo, Macramé, and PlaitingFrom EverandThe Knotting & Braiding Bible: The Complete Guide to Creative Knotting including Kumihimo, Macramé, and PlaitingRating: 4.5 out of 5 stars4.5/5 (5)