You might also like
- Shoulder JointDocument42 pagesShoulder Jointcaystone99No ratings yet
- Joints of The Lower Limb DiagramsDocument39 pagesJoints of The Lower Limb Diagramssanullah123khan.13No ratings yet
- Shoulder: Sternoclavicular JointDocument9 pagesShoulder: Sternoclavicular JointKatherine NunnNo ratings yet
- Upper Limb SkeletonDocument28 pagesUpper Limb SkeletonDanaNo ratings yet
- 2 Shoulder Girdle JointsDocument29 pages2 Shoulder Girdle JointsFarrukh ShahzadNo ratings yet
- Joints of Lower LimbsDocument12 pagesJoints of Lower LimbsMohammed SheikhNo ratings yet
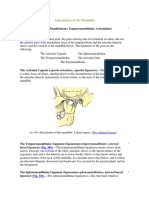
- The Articulation of The MandibleDocument4 pagesThe Articulation of The Mandibleviorel79No ratings yet
- Knee Joint (Anatomy)Document5 pagesKnee Joint (Anatomy)Ojambo FlaviaNo ratings yet
- Upper LimbDocument14 pagesUpper LimbAmbg GhalyNo ratings yet
- Articulation of The Upper ExtremityDocument40 pagesArticulation of The Upper ExtremityDaliaWehNo ratings yet
- Anatomy and Physiology of The Hip BoneDocument2 pagesAnatomy and Physiology of The Hip BoneNkk Aqnd MgdnglNo ratings yet
- Elbow and Antebrachium NotesDocument8 pagesElbow and Antebrachium NoteschadNo ratings yet
- Naik, S. - Biomechanics of Knee ComplexDocument25 pagesNaik, S. - Biomechanics of Knee ComplexKyle Bois100% (4)
- BONEDocument27 pagesBONEVIJAYA KUMAR YNo ratings yet
- Vertebral JointDocument5 pagesVertebral Jointاحمد البزورNo ratings yet
- Examinationoftmjmusclesofmastication2 140115105518 Phpapp02Document79 pagesExaminationoftmjmusclesofmastication2 140115105518 Phpapp02Dr. Anjana MaharjanNo ratings yet
- Assignment Shoulder JointDocument7 pagesAssignment Shoulder JointMary Grace OrozcoNo ratings yet
- Anatomy Units 9-12 ObjectivesDocument18 pagesAnatomy Units 9-12 ObjectivespoNo ratings yet
- Pectoral Girdle and Shoulder JointDocument55 pagesPectoral Girdle and Shoulder JointGaurav ThapaNo ratings yet
- Lec 14 THE KNEE JOINTDocument17 pagesLec 14 THE KNEE JOINTMaheen IrfanNo ratings yet
- Nikkupdfonjoints 180220063659Document84 pagesNikkupdfonjoints 180220063659Adu-danquah StephenNo ratings yet
- Anatomy and Physiology of The Hip BoneDocument8 pagesAnatomy and Physiology of The Hip BoneBeGie MamBaNo ratings yet
- Chapter 24 - MSKDocument3 pagesChapter 24 - MSKannoja selvaNo ratings yet
- Temporomandibular Joint and Muscles of Mastication: ContentsDocument38 pagesTemporomandibular Joint and Muscles of Mastication: ContentsDan 04No ratings yet
- Classification of JointsDocument13 pagesClassification of JointsRajat NangiaNo ratings yet
- Shoulder JointDocument100 pagesShoulder JointKhushboo IkramNo ratings yet
- Comparison of Shoulder and Hip JointDocument3 pagesComparison of Shoulder and Hip JointTONY GO AWAY67% (3)
- Shoulder JointDocument17 pagesShoulder JointShimmering MoonNo ratings yet
- Knee 05102018Document24 pagesKnee 05102018Dk KNo ratings yet
- The Back: Cortez Gomez Lucas VillafuerteDocument53 pagesThe Back: Cortez Gomez Lucas VillafuerteFlorenze Laiza Donor LucasNo ratings yet
- GRDA Intro Bony PelvisDocument5 pagesGRDA Intro Bony PelvisKingNo ratings yet
- Lec: TMJ DR - Nawres BahaaDocument13 pagesLec: TMJ DR - Nawres BahaaMarwa AlfuaadiNo ratings yet
- Anatomy I 24.03.20Document17 pagesAnatomy I 24.03.20Arianna RomanoNo ratings yet
- Sama Notes Upper LimbDocument15 pagesSama Notes Upper LimbMaiUyen Kieu50% (2)
- Joints and Ligaments of VertebraeDocument7 pagesJoints and Ligaments of Vertebraerahma sajjadNo ratings yet
- Articulations of The PelvisDocument4 pagesArticulations of The PelvisSiva ShanmugamNo ratings yet
- Learning Objectives: The Shoulder JointDocument7 pagesLearning Objectives: The Shoulder JointLaura TapiaNo ratings yet
- AnatomyDocument29 pagesAnatomyazeemNo ratings yet
- Temporomandibular JointDocument86 pagesTemporomandibular Jointdrpankajaapaliya100% (2)
- Anatomy 1Document17 pagesAnatomy 1Uljana NasonovaNo ratings yet
- Hip Joint - Anatomy and Physiology: LigamentsDocument3 pagesHip Joint - Anatomy and Physiology: LigamentsNeil AlviarNo ratings yet
- TMJ WordDocument21 pagesTMJ WordBharathi GudapatiNo ratings yet
- CHAPTER 2 Thoracic LimbDocument32 pagesCHAPTER 2 Thoracic LimbChristine Joyce NavarroNo ratings yet
- Joints: Dr. Vidhya Department of AnatomyDocument27 pagesJoints: Dr. Vidhya Department of Anatomyelan suriyanNo ratings yet
- JointsDocument27 pagesJointsVarsha Mol MohananNo ratings yet
- Overview of Anatomy of The Upper LimbsDocument5 pagesOverview of Anatomy of The Upper LimbsRosanaNo ratings yet
- Definition of Shoulder DislocationDocument66 pagesDefinition of Shoulder DislocationDeepika verma100% (1)
- AD 5 Vertebral AnatomyDocument37 pagesAD 5 Vertebral AnatomyLintang ZerlinaNo ratings yet
- Hap AssignmentDocument3 pagesHap AssignmentMaliha khanNo ratings yet
- TMJ Disorders 1Document7 pagesTMJ Disorders 1Negin HekmatjooNo ratings yet
- AnteriorDocument13 pagesAnteriorFranz FradesNo ratings yet
- O.L.Zharikova, PH.D., Associate Professor Department of Normal Anatomy BSMU, MinskDocument37 pagesO.L.Zharikova, PH.D., Associate Professor Department of Normal Anatomy BSMU, MinsknishaninishaNo ratings yet
- Anatomy of Hip JointDocument5 pagesAnatomy of Hip JointSneha ParveenNo ratings yet
- Tempromanndibular JointDocument10 pagesTempromanndibular Jointehab radmanNo ratings yet
- The Hip JointDocument4 pagesThe Hip Jointshash82No ratings yet
- ANATOMY I 23.03.20 I The Pectoral Girdle and Upper LimbDocument25 pagesANATOMY I 23.03.20 I The Pectoral Girdle and Upper LimbArianna RomanoNo ratings yet
- Arthrology: DR N. ChikumbaDocument50 pagesArthrology: DR N. ChikumbaNatty ChikumbaNo ratings yet
- Shoulder Joint Complex and Arm RegionDocument59 pagesShoulder Joint Complex and Arm RegionGish KioiNo ratings yet
- HIP JOINT PresentationDocument16 pagesHIP JOINT PresentationAreeha KhanNo ratings yet
- The Joint Capsule May Be RegardedDocument4 pagesThe Joint Capsule May Be RegardedAlina MoiseNo ratings yet
- Interchondral LigamentsDocument8 pagesInterchondral LigamentsAlina MoiseNo ratings yet
- Arthrology FinalDocument28 pagesArthrology FinalAlina MoiseNo ratings yet
- ARTHROLOGYDocument10 pagesARTHROLOGYAlina MoiseNo ratings yet
- The Joint Capsule May Be RegardedDocument4 pagesThe Joint Capsule May Be RegardedAlina MoiseNo ratings yet
- The Joint Capsule May Be RegardedDocument4 pagesThe Joint Capsule May Be RegardedAlina MoiseNo ratings yet
- The Joint Capsule May Be RegardedDocument4 pagesThe Joint Capsule May Be RegardedAlina MoiseNo ratings yet
- Open Note TestDocument9 pagesOpen Note TestDean JezerNo ratings yet
- Week 6 PCP Workbook QsDocument6 pagesWeek 6 PCP Workbook Qsapi-479849199No ratings yet
- Sports OITE - 2012 2013 2014Document167 pagesSports OITE - 2012 2013 2014ICH KhuyNo ratings yet
- Examination of CNS PDFDocument38 pagesExamination of CNS PDFZargis Talukder100% (3)
- Mbbs Question BankDocument38 pagesMbbs Question BankHappy MukherjeeNo ratings yet
- World Armwrestling Federation (WAF) Rules of Armwrestling Sitdown and StandingDocument13 pagesWorld Armwrestling Federation (WAF) Rules of Armwrestling Sitdown and StandingZil FadliNo ratings yet
- The Magic of Correct Pin Placement in Ilizarov SurgeryDocument34 pagesThe Magic of Correct Pin Placement in Ilizarov SurgeryLakshmanan PrakashNo ratings yet
- I Sing of Arms and of A Man Medial Epicondylosis and The Sexual Division of Labour in Prehistoric EuropeDocument8 pagesI Sing of Arms and of A Man Medial Epicondylosis and The Sexual Division of Labour in Prehistoric EuropeFelipe ÁngelNo ratings yet
- Simplified New Energy WaysDocument36 pagesSimplified New Energy WaysOBNo ratings yet
- 2.08 KinanthrEometric AssesDocument30 pages2.08 KinanthrEometric AssesAndreas ZourdosNo ratings yet
- 3 Trends Worth Tapping IntoDocument8 pages3 Trends Worth Tapping IntoJefferson Medinaceli MalayaoNo ratings yet
- David Butler Neural Tissue Mobilisation-1Document11 pagesDavid Butler Neural Tissue Mobilisation-1Himani BhondgeNo ratings yet
- Complication of FractureDocument79 pagesComplication of FractureAhmad SyahmiNo ratings yet
- All About MalteseDocument82 pagesAll About MalteselubokojyxarovNo ratings yet
- Price List Euro 2022Document6 pagesPrice List Euro 2022mnegrilam2002No ratings yet
- Elbow: Posterior ApproachDocument5 pagesElbow: Posterior Approachhaitham alkhamaisehNo ratings yet
- Workout BookDocument13 pagesWorkout Bookfordy1usNo ratings yet
- Apk 1997Document9 pagesApk 1997Pau CMedinaNo ratings yet
- Amputation LevelsDocument9 pagesAmputation Levelskrissh20No ratings yet
- TNT Get Back in Shape Workouts PDFDocument10 pagesTNT Get Back in Shape Workouts PDFaboubakereldjazairi100% (1)
- Chicken Wing DissectionDocument13 pagesChicken Wing DissectionJaga_Sahsiny_1No ratings yet
- Ab'Asanas (Expanded & Updated)Document56 pagesAb'Asanas (Expanded & Updated)Nicola AvonNo ratings yet
- Kinesiology Elbow Joint PDFDocument8 pagesKinesiology Elbow Joint PDFRozyNo ratings yet
- Movement Mobility 101Document21 pagesMovement Mobility 101testNo ratings yet
- 2023 JOT Low Transcondylar Fractures of The Distal Humerus - A Multicenter Cohort StudyDocument6 pages2023 JOT Low Transcondylar Fractures of The Distal Humerus - A Multicenter Cohort StudyjcmarecauxlNo ratings yet
- Supracondylar Fractures of The Humerus in Children.3Document8 pagesSupracondylar Fractures of The Humerus in Children.3Azmi FarhadiNo ratings yet
- Dermatomes and Myotomes and Its Clinical Special Test in Upper Limb and Lower LimbDocument42 pagesDermatomes and Myotomes and Its Clinical Special Test in Upper Limb and Lower LimbkkaammiillaahhNo ratings yet
- Gym BasicsDocument112 pagesGym BasicsMario Maldonado100% (1)
- OMM Review SheetDocument9 pagesOMM Review SheetSolomon Seth Sallfors100% (2)
- Tendon ReflexDocument13 pagesTendon ReflexNurul Huda M ShahrinNo ratings yet