You might also like
- Emergencymedicine Evaluationandmanagement Ofanemia: Brit Long,, Alex KoyfmanDocument22 pagesEmergencymedicine Evaluationandmanagement Ofanemia: Brit Long,, Alex KoyfmanVictor ChisNo ratings yet
- Normocytic Anemia Guide for Family PhysiciansDocument16 pagesNormocytic Anemia Guide for Family PhysiciansPaula ArayaNo ratings yet
- Emergencymedicine Evaluationandmanagement Ofanemia: Brit Long,, Alex KoyfmanDocument22 pagesEmergencymedicine Evaluationandmanagement Ofanemia: Brit Long,, Alex KoyfmanCarlos Alberto Torres LópezNo ratings yet
- New Treatment Paradigm for Iron Deficiency Anemia in the ElderlyDocument11 pagesNew Treatment Paradigm for Iron Deficiency Anemia in the ElderlyCarlos OlivoNo ratings yet
- Anemia For The Primary Care PhysicianDocument16 pagesAnemia For The Primary Care PhysicianAbdón Guerra FariasNo ratings yet
- Tinjauan Pustaka 2Document12 pagesTinjauan Pustaka 226 ThufailNo ratings yet
- Journal 1Document13 pagesJournal 1Nur Ajiyanti 'anthi' SabirinaNo ratings yet
- Anemia: Marcel E Conrad, MD, (Retired) Distinguished Professor of Medicine, UniversityDocument56 pagesAnemia: Marcel E Conrad, MD, (Retired) Distinguished Professor of Medicine, UniversityChamara AtukoralaNo ratings yet
- Hemolytic Anemia ReviewDocument7 pagesHemolytic Anemia ReviewMihu DragostinNo ratings yet
- AnemiaDocument26 pagesAnemiaGustavo GracoNo ratings yet
- Table 93-1 1: Prevalence of AnemiaDocument4 pagesTable 93-1 1: Prevalence of AnemiaorangeNo ratings yet
- Blood Disorders in GeriatricDocument29 pagesBlood Disorders in GeriatricdheaNo ratings yet
- Author 'S Accepted ManuscriptDocument24 pagesAuthor 'S Accepted ManuscriptAgal BimaNo ratings yet
- Anemia in PregnancyDocument11 pagesAnemia in PregnancyDustin Raul Lazo BedoyaNo ratings yet
- Iron Deficiency Anemia in Pregnancy: Clinical Expert SeriesDocument12 pagesIron Deficiency Anemia in Pregnancy: Clinical Expert Seriesognesia putri wageNo ratings yet
- Types, Causes, Symptoms and Treatment of AnemiaDocument54 pagesTypes, Causes, Symptoms and Treatment of Anemiaammar amerNo ratings yet
- Update On (Approach To) Anemia1 (Changes)Document39 pagesUpdate On (Approach To) Anemia1 (Changes)Balchand KukrejaNo ratings yet
- Anemia in ChildrenDocument9 pagesAnemia in ChildrenVillegas Sepúlveda AbrahamNo ratings yet
- Evaluation of MacrocytosisDocument6 pagesEvaluation of MacrocytosisSi vis pacem...No ratings yet
- Anemia of Chronic Disease in The ElderlyDocument7 pagesAnemia of Chronic Disease in The ElderlyAkbarNo ratings yet
- Review Jurnal Anfisman Grup G English VersionDocument11 pagesReview Jurnal Anfisman Grup G English VersionKayla NikenNo ratings yet
- 1 s2.0 S0006497120325088 MainDocument10 pages1 s2.0 S0006497120325088 MainDewi NurpitasariNo ratings yet
- Anemia at Older AgeDocument10 pagesAnemia at Older AgeAbdullah ZuhairNo ratings yet
- 505 FullDocument11 pages505 FullRolando Jose CastilloNo ratings yet
- ABP3 IntoxmetalespesadosDocument18 pagesABP3 IntoxmetalespesadosFernandoLuyoNo ratings yet
- Anemia in PregnancyDocument7 pagesAnemia in PregnancyNatalia ElizabethNo ratings yet
- Anemia y Tracto GiDocument5 pagesAnemia y Tracto GiCarlos MichasNo ratings yet
- Anemia Research PaperDocument7 pagesAnemia Research Papergw0q12dx100% (1)
- лекции англDocument17 pagesлекции англBrett StevensonNo ratings yet
- Study of Anemia and Its Correlation With Hematological Parameters in Patient of Various Age GroupDocument7 pagesStudy of Anemia and Its Correlation With Hematological Parameters in Patient of Various Age GroupIOSRjournal0% (1)
- Pediatric Acute Anemia PDFDocument6 pagesPediatric Acute Anemia PDFpurwanto nugrohoNo ratings yet
- Anemia LectureDocument12 pagesAnemia LectureprogramgrabberNo ratings yet
- 857 1857 1 PBDocument4 pages857 1857 1 PBJesselle LasernaNo ratings yet
- IDA by DR AbdifatahDocument52 pagesIDA by DR AbdifatahAbdifatah AhmedNo ratings yet
- Haematology AnemiaDocument7 pagesHaematology AnemiaGayanNo ratings yet
- Evaluation of Anemia in ChildrenDocument9 pagesEvaluation of Anemia in ChildrenHasnaniaNo ratings yet
- AnemiaDocument21 pagesAnemiaMarie WagasNo ratings yet
- Presentation On Blood DisordersDocument122 pagesPresentation On Blood Disordersvarshasharma05No ratings yet
- GGFHGFJKL KJKHGFDGHJKLDocument14 pagesGGFHGFJKL KJKHGFDGHJKLVania Millenia MelindaNo ratings yet
- 209-Hematology Review - Case StudiesDocument129 pages209-Hematology Review - Case StudiesKhalid Khalidi100% (2)
- Chapter 49Document6 pagesChapter 49Melissa Aina Mohd YusofNo ratings yet
- Progress ReportDocument28 pagesProgress ReportHope SerquiñaNo ratings yet
- Practice Question Week 1Document9 pagesPractice Question Week 1Gps PandetteNo ratings yet
- Jurnal AnastesiDocument12 pagesJurnal AnastesilissamariasianiparNo ratings yet
- Anemia (: /Ə Ni Miə/ Also Spelled Greek Red Blood Cells HemoglobinDocument13 pagesAnemia (: /Ə Ni Miə/ Also Spelled Greek Red Blood Cells HemoglobinAryana BudiawanNo ratings yet
- Anemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewDocument15 pagesAnemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewZoreyca RiveraNo ratings yet
- Pharmaceutical Sciences: A Case-Control Study of Prevalence of Anaemia Among Patients With Type 2 DiabetesDocument5 pagesPharmaceutical Sciences: A Case-Control Study of Prevalence of Anaemia Among Patients With Type 2 DiabetesiajpsNo ratings yet
- Erythrocyte Life Cycle: PathophysiologyDocument15 pagesErythrocyte Life Cycle: PathophysiologyYeniNo ratings yet
- Running Head: BLOOD DISORDERS 1Document6 pagesRunning Head: BLOOD DISORDERS 1serenity779No ratings yet
- Anemia (Pronounced: o o o o o o oDocument12 pagesAnemia (Pronounced: o o o o o o opamela100181No ratings yet
- Approach Considerations: Magnetic Resonance Imaging in Research SettingsDocument5 pagesApproach Considerations: Magnetic Resonance Imaging in Research SettingsLamyaa Ali HasanNo ratings yet
- PallorDocument16 pagesPallorManal AlQuaimi100% (1)
- J of Gen and Family Med - 2017 - Nagao - Diagnosis and Treatment of Macrocytic Anemias in AdultsDocument5 pagesJ of Gen and Family Med - 2017 - Nagao - Diagnosis and Treatment of Macrocytic Anemias in Adultsmarcolius11No ratings yet
- Thesis AnemiaDocument7 pagesThesis AnemiaBuyPapersForCollegeSingapore100% (1)
- Salinan Terjemahan 307211717 Laporan Pendahuluan AnemiaDocument16 pagesSalinan Terjemahan 307211717 Laporan Pendahuluan AnemiaRidho HidayatullahNo ratings yet
- Evaluation of Pallor in ChildrenDocument23 pagesEvaluation of Pallor in ChildrenFlorie Lei BulosNo ratings yet
- The Complete Guide on Anemia: Learn Anemia Symptoms, Anemia Causes, and Anemia Treatments. Anemia types covered in full details: Iron-deficiency, Microcytic, Autoimmune Hemolytic, Sideroblastic, and Normocytic AnemiaFrom EverandThe Complete Guide on Anemia: Learn Anemia Symptoms, Anemia Causes, and Anemia Treatments. Anemia types covered in full details: Iron-deficiency, Microcytic, Autoimmune Hemolytic, Sideroblastic, and Normocytic AnemiaRating: 3.5 out of 5 stars3.5/5 (9)
- Blood DisordersDocument8 pagesBlood DisordersDeevashwer Rathee100% (1)
- JR TA AnemiaDocument26 pagesJR TA AnemiaMohamad Ananto CNo ratings yet
- Artificial Lung Design & Gas ExchangeDocument25 pagesArtificial Lung Design & Gas Exchangealoove66No ratings yet
- C5 - Metabolism and Enzyme Part 1Document20 pagesC5 - Metabolism and Enzyme Part 1Daniel LohNo ratings yet
- Brain Basics: John Jefferys and Alison CooperDocument20 pagesBrain Basics: John Jefferys and Alison CooperswarnNo ratings yet
- 3 9 1 bMSDS-Reagen-LaboratoriumDocument4 pages3 9 1 bMSDS-Reagen-Laboratoriumswahyulisah100% (1)
- Chapter 3 Science Form 4Document30 pagesChapter 3 Science Form 4Shafie BuyaminNo ratings yet
- Super 108 DR LalDocument8 pagesSuper 108 DR Lalarkaprava paulNo ratings yet
- ANAESTHESIOLOGYDocument38 pagesANAESTHESIOLOGYcollinsmagNo ratings yet
- SGD Physiology Endocrine and MetabolismDocument7 pagesSGD Physiology Endocrine and MetabolismTinesh RajahNo ratings yet
- HerniaDocument36 pagesHerniashankarrao3No ratings yet
- 2016 - 13 - Fleming - Lagged Syndesmotic Fixation - Our Clinical ExperienceDocument8 pages2016 - 13 - Fleming - Lagged Syndesmotic Fixation - Our Clinical ExperienceJacob DoughertyNo ratings yet
- The Management of Intra Abdominal Infections From A Global Perspective 2017 WSES Guidelines For Management of Intra Abdominal InfectionsDocument34 pagesThe Management of Intra Abdominal Infections From A Global Perspective 2017 WSES Guidelines For Management of Intra Abdominal InfectionsJuan CastroNo ratings yet
- M 371Document14 pagesM 371Anonymous h0DxuJTNo ratings yet
- 2018 Life Sciences Tsset (Answers With Explanation)Document24 pages2018 Life Sciences Tsset (Answers With Explanation)Swetha SrigirirajuNo ratings yet
- Personal IdentificationDocument13 pagesPersonal IdentificationJose Li ToNo ratings yet
- Spesifikasi Patient Monitor: Draeger - Vista 120S: Type Parameter Merk FeaturesDocument3 pagesSpesifikasi Patient Monitor: Draeger - Vista 120S: Type Parameter Merk Featuresflorensia shielyNo ratings yet
- Anatomy of A ClamDocument6 pagesAnatomy of A ClamRU VickNo ratings yet
- Modul Strategik Bab 1 Ting 5Document6 pagesModul Strategik Bab 1 Ting 5SK Pos TenauNo ratings yet
- 3.03 Understand Structures, Functions and Disorders of The Nervous SystemDocument38 pages3.03 Understand Structures, Functions and Disorders of The Nervous SystemLoriwinchesterNo ratings yet
- Phylum Arthropoda - Why such abundance and diversityDocument4 pagesPhylum Arthropoda - Why such abundance and diversitySHILNo ratings yet
- Bulacan State University College of Nursing Final Exam ReviewDocument7 pagesBulacan State University College of Nursing Final Exam ReviewDemiar Madlansacay QuintoNo ratings yet
- Mobilization NotesDocument239 pagesMobilization NotesSuganya Balachandran100% (6)
- HeparinDocument2 pagesHeparinNinoska Garcia-Ortiz100% (4)
- Cell Cycle Lesson PlanDocument4 pagesCell Cycle Lesson PlanJustine Pama94% (17)
- What Are The Types of EndosDocument3 pagesWhat Are The Types of EndosSailu KatragaddaNo ratings yet
- MSC 060913 PDFDocument44 pagesMSC 060913 PDFViroopaksha V JaddipalNo ratings yet
- IlizarovDocument62 pagesIlizarovAsh Moaveni100% (2)
- Overview of Complications Occurring in The Post-Anesthesia Care UnitDocument14 pagesOverview of Complications Occurring in The Post-Anesthesia Care UnitShahabuddin ShaikhNo ratings yet
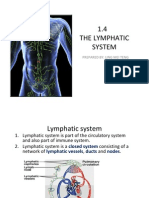
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDocument15 pages1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingNo ratings yet
- Unit 1, InvertebratesDocument4 pagesUnit 1, InvertebratesnatalescorNo ratings yet
- Long-Term Memory Encoding and RetrievalDocument24 pagesLong-Term Memory Encoding and RetrievalThavasi mari selvam NNo ratings yet