You might also like
- Endogenous Modulation of Pain The Role of Exercise, Stress and Cognitions in HumansDocument36 pagesEndogenous Modulation of Pain The Role of Exercise, Stress and Cognitions in HumansLuis cabezas mirandaNo ratings yet
- Efectos Analgesicos EjercicioDocument12 pagesEfectos Analgesicos Ejerciciomilagro meza poloNo ratings yet
- The Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisDocument20 pagesThe Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisBruno FellipeNo ratings yet
- PRM2022 4203138Document8 pagesPRM2022 4203138sarahNo ratings yet
- Sensibilidad Cambio Clinico Instrumentos Generales Especificos Dolor CronicoDocument8 pagesSensibilidad Cambio Clinico Instrumentos Generales Especificos Dolor CronicovitorperonaNo ratings yet
- 1 s2.0 S0965229923000833 MainDocument11 pages1 s2.0 S0965229923000833 MaintheophileflorentinNo ratings yet
- Kine 260Document8 pagesKine 260MarianaNo ratings yet
- Eccentric Exercise and TendinosisDocument13 pagesEccentric Exercise and Tendinosisalinache23No ratings yet
- Arthritis Care Research - 2022 - Lima - How Do Non Surgical Interventions Improve Pain and Physical Function in PeopleDocument36 pagesArthritis Care Research - 2022 - Lima - How Do Non Surgical Interventions Improve Pain and Physical Function in PeoplerdkelsallNo ratings yet
- Aquiles y ExcentricosDocument13 pagesAquiles y ExcentricosCarlos ZavallaNo ratings yet
- Ex. ProtocolDocument17 pagesEx. ProtocoladityaNo ratings yet
- To Compare The Effect of Core Stability Exercises and Muscle Energy Techniques On Low Back Pain PatientsDocument7 pagesTo Compare The Effect of Core Stability Exercises and Muscle Energy Techniques On Low Back Pain PatientsDr Ahmed NabilNo ratings yet
- Author's Accepted Manuscript: Seminars inDocument35 pagesAuthor's Accepted Manuscript: Seminars inAugusto SantosNo ratings yet
- Kinesiofobia y Catastrofismo Del Dolor y PilatesDocument7 pagesKinesiofobia y Catastrofismo Del Dolor y Pilatescecilia martinezNo ratings yet
- Temporal Pattern of The Repeated Bout Effect of Eccentric Exercise On Delayed-Onset Muscle SorenessDocument5 pagesTemporal Pattern of The Repeated Bout Effect of Eccentric Exercise On Delayed-Onset Muscle SorenessRicardo Pereira NevesNo ratings yet
- Assignment Final #2Document6 pagesAssignment Final #2Hafsa ShahzadaNo ratings yet
- Texto Exercício Aeróbico Saúde Mental Uma Revisão Sistemática e Meta-Análise.Document15 pagesTexto Exercício Aeróbico Saúde Mental Uma Revisão Sistemática e Meta-Análise.canaldasprofissoesNo ratings yet
- Psychological Predictors of Anterior Cruciate Ligament Reconstruction Outcomes: A Systematic ReviewDocument11 pagesPsychological Predictors of Anterior Cruciate Ligament Reconstruction Outcomes: A Systematic ReviewjavierNo ratings yet
- A Prediction Rule For Shoulder Pain Related Sick Leave - A Prospective Cohort StudyDocument11 pagesA Prediction Rule For Shoulder Pain Related Sick Leave - A Prospective Cohort StudyGenocir FrankeNo ratings yet
- Exercise and The Prevention of DepressionDocument9 pagesExercise and The Prevention of DepressionEdlene HoffmannNo ratings yet
- Exercise and The Prevention of Depression: Results of The HUNT Cohort StudyDocument9 pagesExercise and The Prevention of Depression: Results of The HUNT Cohort StudyLydia AmaliaNo ratings yet
- Lofgren Et Al., (2018) Long-Term, Health-Enhancing PhysicalDocument9 pagesLofgren Et Al., (2018) Long-Term, Health-Enhancing PhysicalAna Flávia SordiNo ratings yet
- 1737 FullDocument9 pages1737 FullSiti RofatulNo ratings yet
- Acute StretchDocument11 pagesAcute StretchGeorge M. PamborisNo ratings yet
- Kinesio Taping For Sports Injuries: Doi: 10.1136/bjsports-2013-093027Document3 pagesKinesio Taping For Sports Injuries: Doi: 10.1136/bjsports-2013-093027Silvanilla PiliNo ratings yet
- Artigo Numero 3Document13 pagesArtigo Numero 3Bruna AraujoNo ratings yet
- Improvement in Anxiety and Pain After Whole Body Whirlpool Hydrotherapy Among Patients With Myofascial Pain SyndromeDocument8 pagesImprovement in Anxiety and Pain After Whole Body Whirlpool Hydrotherapy Among Patients With Myofascial Pain Syndromephysicallen1791No ratings yet
- Aerobic Excercise CompleteDocument25 pagesAerobic Excercise CompleteWACHRISNo ratings yet
- 1 - 2017 - Tuina para Prob Musculo-Esqueléticos - Rev SistDocument22 pages1 - 2017 - Tuina para Prob Musculo-Esqueléticos - Rev SistLuis Miguel MartinsNo ratings yet
- Relationship Between Pain Intensity, Pain Catastrophizing, and Self-Efficacy in Patients With Frozen Shoulder: A Cross-Sectional StudyDocument6 pagesRelationship Between Pain Intensity, Pain Catastrophizing, and Self-Efficacy in Patients With Frozen Shoulder: A Cross-Sectional Studyluisherrera1490No ratings yet
- 2.chronicback PainDocument9 pages2.chronicback PainRiantiara PutrizaNo ratings yet
- Neuromuscular Training For Sports InjuryDocument9 pagesNeuromuscular Training For Sports InjuryPaulo Muñoz BrauchiNo ratings yet
- Journal of Affective Disorders: Research PaperDocument11 pagesJournal of Affective Disorders: Research PaperIvan Andres TorrisiNo ratings yet
- 1 Tai Chi and Rheumatic DiseasesDocument14 pages1 Tai Chi and Rheumatic DiseasescinborbNo ratings yet
- Brain Sciences: Exercise Strengthens Central Nervous System Modulation of Pain in FibromyalgiaDocument13 pagesBrain Sciences: Exercise Strengthens Central Nervous System Modulation of Pain in FibromyalgiaJavier Alejandro Rodriguez MelgozaNo ratings yet
- Assignment Final #3Document6 pagesAssignment Final #3Hafsa ShahzadaNo ratings yet
- 10 1589@jpts 28 96Document6 pages10 1589@jpts 28 96Dian Oktaria SafitriNo ratings yet
- PIIS1526590018304565Document18 pagesPIIS1526590018304565gguida0No ratings yet
- DeeptydhayaniDocument7 pagesDeeptydhayaniburhanNo ratings yet
- Review ArticleDocument14 pagesReview ArticleLuisNo ratings yet
- Jah3 2 E004473 PDFDocument9 pagesJah3 2 E004473 PDFMateo MendozaNo ratings yet
- 21 Lumber StenoisDocument21 pages21 Lumber Stenoisanaab atif ahmedNo ratings yet
- Continued Sports Activity, Using A Pain - Monitoring Model, During Rehabilitation in Patients With Achilles TendinopathyDocument10 pagesContinued Sports Activity, Using A Pain - Monitoring Model, During Rehabilitation in Patients With Achilles TendinopathyMichele MarengoNo ratings yet
- 10 3238@arztebl 2014 0592Document9 pages10 3238@arztebl 2014 0592filipecorsairNo ratings yet
- Exercise Training For Blood Pressure: A Systematic Review and Meta-AnalysisDocument9 pagesExercise Training For Blood Pressure: A Systematic Review and Meta-AnalysisAnonymous 7dsX2F8nNo ratings yet
- Shoulder Symptoms (GP)Document8 pagesShoulder Symptoms (GP)Putri PadmosuwarnoNo ratings yet
- Ceballos-Laita 2020Document15 pagesCeballos-Laita 2020Marco Antonio Morales OsorioNo ratings yet
- Effects of Exercise On Quality of Life in Stroke Survivors: A Meta-AnalysisDocument12 pagesEffects of Exercise On Quality of Life in Stroke Survivors: A Meta-AnalysisNoor KameliaNo ratings yet
- Jurnal B.ing PlorenDocument10 pagesJurnal B.ing Plorensingkong gurihNo ratings yet
- 201705gillespie 1Document9 pages201705gillespie 1Jose PerezNo ratings yet
- Meta Analisis Exercise Therapy For Nonspecific Low Back Pain 2005Document28 pagesMeta Analisis Exercise Therapy For Nonspecific Low Back Pain 2005BenjaminNo ratings yet
- Exercise For Chronic Musculoskeletal Pain: A Biopsychosocial ApproachDocument9 pagesExercise For Chronic Musculoskeletal Pain: A Biopsychosocial ApproachAndressa FerreiraNo ratings yet
- Jurnal 11Document7 pagesJurnal 11nora cyeanirNo ratings yet
- Best Practice & Research Clinical Rheumatology: Kim L. Bennell, Fiona Dobson, Rana S. HinmanDocument25 pagesBest Practice & Research Clinical Rheumatology: Kim L. Bennell, Fiona Dobson, Rana S. HinmanPablo Fuentes LaraNo ratings yet
- Power of Words Influence of Preexercise Information On Hypoalgesia After Exercise Randomized Controlled TrialDocument32 pagesPower of Words Influence of Preexercise Information On Hypoalgesia After Exercise Randomized Controlled TrialDuvan CarvajalNo ratings yet
- Therapeutic Exercise and Orthopedic Manual Therapy For Impingement Syndrome: A Systematic ReviewDocument7 pagesTherapeutic Exercise and Orthopedic Manual Therapy For Impingement Syndrome: A Systematic ReviewkhushmitNo ratings yet
- Kraaimaat 2003Document21 pagesKraaimaat 2003tanviNo ratings yet
- 1711 16 2457 1 10 20201014 PDFDocument7 pages1711 16 2457 1 10 20201014 PDFRodrigo SaireNo ratings yet
- Exercicio e DorDocument3 pagesExercicio e DorOctavio HoraNo ratings yet
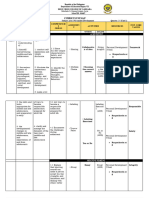
- Understanding by DesignDocument2 pagesUnderstanding by DesignWen Yee TangNo ratings yet
- Ethics ppt3Document22 pagesEthics ppt3Maryam SharifNo ratings yet
- CH 1 8th EditionDocument26 pagesCH 1 8th EditionKim DepapeNo ratings yet
- Resourcefile 355 PDFDocument1 pageResourcefile 355 PDFYahya AnirNo ratings yet
- Reading ReflectionDocument7 pagesReading ReflectionZulkifli MydeenNo ratings yet
- BCS-A Thomas 2019Document20 pagesBCS-A Thomas 2019Raluca GeorgescuNo ratings yet
- FC2 M2022apccp044 Q3Document3 pagesFC2 M2022apccp044 Q319BPS147 Shravanthi PadmanabanNo ratings yet
- Learning and Teaching PDFDocument75 pagesLearning and Teaching PDFSayali Bhojane0% (1)
- Pe Action Plan - Template Action Plan For Quality Physical Education and Schools SportDocument1 pagePe Action Plan - Template Action Plan For Quality Physical Education and Schools SportElisha TanNo ratings yet
- CMY3705 Assignment 1Document9 pagesCMY3705 Assignment 1Thameshree MoodleyNo ratings yet
- Advertising Research ProjectDocument52 pagesAdvertising Research ProjectronaktejaniNo ratings yet
- Performance Appraisal and 360 DegreeDocument2 pagesPerformance Appraisal and 360 DegreeHosahalli Narayana Murthy PrasannaNo ratings yet
- Lilith in The Houses - Tom JacobsDocument6 pagesLilith in The Houses - Tom Jacobsrigaut74No ratings yet
- Debra L. Nelson, Ronald J. Burke - Gender, Work Stress, and Health (2002)Document260 pagesDebra L. Nelson, Ronald J. Burke - Gender, Work Stress, and Health (2002)Reboot FastbootNo ratings yet
- Environment AnalysisDocument15 pagesEnvironment AnalysisMuhammad Rafiq TanjungNo ratings yet
- Listening Lesson PlanDocument3 pagesListening Lesson PlankalagaziNo ratings yet
- The Twelfth InsightDocument10 pagesThe Twelfth InsightsimonaloredanaNo ratings yet
- What Is PsychodramaDocument2 pagesWhat Is PsychodramaKuthubudeen T MNo ratings yet
- Reyes, Laurence JDocument22 pagesReyes, Laurence JLAURENCE REYESNo ratings yet
- Descriptive Methods - SurveyDocument23 pagesDescriptive Methods - SurveyPriya GunaNo ratings yet
- Digital ShockDocument41 pagesDigital ShockAmanda AhopeltoNo ratings yet
- The Direct Demonstration Method in TeachingDocument6 pagesThe Direct Demonstration Method in TeachingTrixie Mae Candido100% (1)
- Inner Experiences - Theory Measurement Frequency Content and FunctionsDocument165 pagesInner Experiences - Theory Measurement Frequency Content and FunctionsRadael JuniorNo ratings yet
- Grade 11 Per Dev Curriculum Map Unit 1Document4 pagesGrade 11 Per Dev Curriculum Map Unit 1Christel Joy De San PedroNo ratings yet
- Balbin Activity 8 AhiccDocument2 pagesBalbin Activity 8 AhiccJulius Ryan Lim BalbinNo ratings yet
- Your Past LivesDocument165 pagesYour Past LivesSanjay Jain100% (18)
- Cultural AdaptationDocument4 pagesCultural AdaptationcessyJDNo ratings yet
- Mumbai University Exam Circular No 2 22052020Document17 pagesMumbai University Exam Circular No 2 22052020Yash BoradeNo ratings yet
- Structural FunctionalismDocument2 pagesStructural FunctionalismYunis0% (1)
- Practical Exercise Theme: Modern DeontologyDocument8 pagesPractical Exercise Theme: Modern DeontologyАкбота АлдиярNo ratings yet