You might also like
- Meningitis In Children: Signs, Symptoms And TreatmentDocument48 pagesMeningitis In Children: Signs, Symptoms And TreatmentAli FalihNo ratings yet
- Fever With Rash SeminarDocument98 pagesFever With Rash SeminarSYAZRIANA SUHAIMINo ratings yet
- Infections in Pregnancy 2Document26 pagesInfections in Pregnancy 2Karanand Choppingboardd Rahgav MaharajNo ratings yet
- Lymphadenopathy and Lymphadenitis: Causes and ManagementDocument14 pagesLymphadenopathy and Lymphadenitis: Causes and Managementnahiry100% (1)
- Infections in Pregnancy FinalDocument67 pagesInfections in Pregnancy FinalkashafNo ratings yet
- Adenoviruses - Medical Microbiology - NCBI Bookshelf PDFDocument9 pagesAdenoviruses - Medical Microbiology - NCBI Bookshelf PDFNino MwansahNo ratings yet
- @PIDs Curs 200903Document43 pages@PIDs Curs 200903Mohammad_Islam87No ratings yet
- Kumpulan Jurnal DengueDocument122 pagesKumpulan Jurnal DengueMas MantriNo ratings yet
- Neonatal Sepsis 2019.Document6 pagesNeonatal Sepsis 2019.Jean Paúl LópezNo ratings yet
- Treatment and Prognosis of Common Variable ImmunodeficiencyDocument11 pagesTreatment and Prognosis of Common Variable ImmunodeficiencyJoaoNo ratings yet
- Early-Onset Sepsis :clinical and Laboratory ChallengeDocument34 pagesEarly-Onset Sepsis :clinical and Laboratory ChallengelordofthewebNo ratings yet
- Immunodeficiency: Faculty of Applied Science Department of Medical Lab. Ml3A, ML3C, ML3DDocument35 pagesImmunodeficiency: Faculty of Applied Science Department of Medical Lab. Ml3A, ML3C, ML3Dالدنيا ساعة فاجعلها طاعةNo ratings yet
- 2midterm 8 - Diagnostic Virology TRANSDocument2 pages2midterm 8 - Diagnostic Virology TRANSRobee Camille Desabelle-SumatraNo ratings yet
- PAPOVIRUSESDocument35 pagesPAPOVIRUSESFrancis MakanyaNo ratings yet
- I Viral DiseasesDocument41 pagesI Viral DiseasesSagar AcharyaNo ratings yet
- Hiv PPDocument37 pagesHiv PPJitendra YadavNo ratings yet
- Tes Lab Penyakit Infeksi Dan Tropis (April 2011)Document143 pagesTes Lab Penyakit Infeksi Dan Tropis (April 2011)Fajrul AnsarNo ratings yet
- ParasitologyDocument107 pagesParasitologyShimelis Teshome AyalnehNo ratings yet
- Belinda Rodriguez Gerardo Venegas Josue ZometaDocument15 pagesBelinda Rodriguez Gerardo Venegas Josue ZometaBelinda RodriguezNo ratings yet
- Epstein Barr VirusDocument13 pagesEpstein Barr VirusDianaLorenaNo ratings yet
- Immunodeficiency DisordersDocument8 pagesImmunodeficiency DisordersMutya XDNo ratings yet
- Influenza: DR.T .V.R Ao MDDocument81 pagesInfluenza: DR.T .V.R Ao MDtummalapalli venkateswara raoNo ratings yet
- Referat EbvDocument9 pagesReferat EbvgaatgaatNo ratings yet
- Tyhpoid FeverDocument6 pagesTyhpoid FeverMade Oka Heryana100% (1)
- Rubella Ppt. 2017Document10 pagesRubella Ppt. 2017handykavebigNo ratings yet
- Pertusis TreatmentDocument20 pagesPertusis TreatmentJaipratap SinghNo ratings yet
- What is rubella? Causes, symptoms, and prevention of German measlesDocument9 pagesWhat is rubella? Causes, symptoms, and prevention of German measlesMd A RAZZAKNo ratings yet
- Clinical VirologyDocument31 pagesClinical VirologySally ElhadadNo ratings yet
- Cultivation of VirusDocument11 pagesCultivation of VirusSUTHAN50% (2)
- Infectious Diseases - Infective EndocarditisDocument41 pagesInfectious Diseases - Infective Endocarditisfire_n_iceNo ratings yet
- Infectious Diseases in Pregnancy - 2005 Vol.32 Issues 3Document290 pagesInfectious Diseases in Pregnancy - 2005 Vol.32 Issues 3Rickky Kurniawan,MDNo ratings yet
- Bacteria: Acid Fast Bacilli: Nama Karakteristi K Manifestasi Klinis Struktur Antigen + Enzim + Toxin Diagnosis TerapiDocument2 pagesBacteria: Acid Fast Bacilli: Nama Karakteristi K Manifestasi Klinis Struktur Antigen + Enzim + Toxin Diagnosis TerapiAndreas MoekoeNo ratings yet
- Rickettsia Coxiella: Prof. Khalifa Sifaw GhengheshDocument20 pagesRickettsia Coxiella: Prof. Khalifa Sifaw GhengheshKhalifa Sifaw GhengheshNo ratings yet
- Brucellosis: A Highly Contagious Zoonotic DiseaseDocument55 pagesBrucellosis: A Highly Contagious Zoonotic Diseasesana shakeelNo ratings yet
- 2-Microscopic IdentificationDocument24 pages2-Microscopic IdentificationMunir AhmedNo ratings yet
- Melioidosis.: Burkholderia PseudomalleiDocument34 pagesMelioidosis.: Burkholderia Pseudomalleitummalapalli venkateswara raoNo ratings yet
- Neisseria Meningitidis PDFDocument8 pagesNeisseria Meningitidis PDFmulyadiNo ratings yet
- Ovarian Tumor: Obstetrics & GynecologyDocument37 pagesOvarian Tumor: Obstetrics & GynecologyFathimathNo ratings yet
- Arboviruses: R.Varidianto Yudo T., Dr.,MkesDocument19 pagesArboviruses: R.Varidianto Yudo T., Dr.,MkesalbertmogNo ratings yet
- Communicable Disease Epidemiology-1Document84 pagesCommunicable Disease Epidemiology-1Solomon Nageso LaaftooNo ratings yet
- Candida Auris Prevention and ControlDocument2 pagesCandida Auris Prevention and ControlShoaib MughalNo ratings yet
- Managing Febrile Neutropenia in Pediatric Oncology PatientsDocument38 pagesManaging Febrile Neutropenia in Pediatric Oncology Patientsdr FAHADKHALIQSIALNo ratings yet
- (Human Immunodeficiency Virus) &: Acquired Immune Deficiency SyndromeDocument61 pages(Human Immunodeficiency Virus) &: Acquired Immune Deficiency SyndromeGufron MustofaNo ratings yet
- Microbiology: Case 1 Bacterial Wound InfectionsDocument11 pagesMicrobiology: Case 1 Bacterial Wound InfectionsNIMMAGADDA, KETHANANo ratings yet
- CephalosporinsDocument21 pagesCephalosporinsMoha Bin Ladiif75% (4)
- Opportunistic Infections PDFDocument88 pagesOpportunistic Infections PDFironbuang100% (1)
- Dr.T.V.Rao MD 1Document39 pagesDr.T.V.Rao MD 1tummalapalli venkateswara raoNo ratings yet
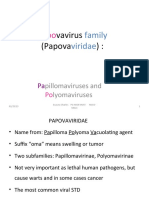
- Papovavirus Family Characteristics and DiseasesDocument25 pagesPapovavirus Family Characteristics and DiseasesIGA ABRAHAMNo ratings yet
- Molecular Carcinogenesis Endometrium PDFDocument7 pagesMolecular Carcinogenesis Endometrium PDFMelati HasnailNo ratings yet
- PyomeningitisDocument54 pagesPyomeningitisRiya BagdiNo ratings yet
- Mycobacterium Tuberculosis and Tuberculosis - TodarDocument18 pagesMycobacterium Tuberculosis and Tuberculosis - TodarTanti Dewi WulantikaNo ratings yet
- Infectious Diseases (1&2) : TuberculosisDocument67 pagesInfectious Diseases (1&2) : TuberculosisYesi SaputriNo ratings yet
- Fungal Virulence FactorsDocument21 pagesFungal Virulence FactorsMutia FatinNo ratings yet
- A Mechanistic Approach to Medicines for Tuberculosis NanotherapyFrom EverandA Mechanistic Approach to Medicines for Tuberculosis NanotherapyMariappan RajanNo ratings yet
- Tuberculosis en PDFDocument307 pagesTuberculosis en PDFAbdullah Khairul AfnanNo ratings yet
- Nri1201 Hiv Poster PDFDocument1 pageNri1201 Hiv Poster PDFalfredoibc100% (1)
- 2018 Final Second Round Senior GroupDocument43 pages2018 Final Second Round Senior GroupKalpavriksha1974No ratings yet
- 2018 Final Second Round JuniorDocument64 pages2018 Final Second Round JuniorKalpavriksha1974No ratings yet
- Ultrasound Report The Black Box of Fetal StatusDocument43 pagesUltrasound Report The Black Box of Fetal StatusKalpavriksha19740% (1)
- Fetal Growth RestrictionDocument74 pagesFetal Growth RestrictionKalpavriksha1974No ratings yet
- 2018 Final Best Second Round JuniorDocument64 pages2018 Final Best Second Round JuniorKalpavriksha1974No ratings yet
- 2018 Kalpavriksha Round 2 Senior Group 3 Question PaperDocument13 pages2018 Kalpavriksha Round 2 Senior Group 3 Question PaperKalpavriksha1974No ratings yet
- 2nd Kalpavriksha Interschool Quiz Competition 2013Document83 pages2nd Kalpavriksha Interschool Quiz Competition 2013Kalpavriksha1974No ratings yet
- 2018 Final Junior RoundDocument43 pages2018 Final Junior RoundKalpavriksha1974No ratings yet
- 2018 Final Best Second Round SeniorDocument71 pages2018 Final Best Second Round SeniorKalpavriksha1974No ratings yet
- Recent Advances in Gynaec UsgDocument46 pagesRecent Advances in Gynaec UsgKalpavriksha1974No ratings yet
- First Trimester (NT-NB Scan) - Inverting The Antenatal PyramidDocument21 pagesFirst Trimester (NT-NB Scan) - Inverting The Antenatal PyramidKalpavriksha1974No ratings yet
- Infertile Couple - Role of Ultrasound FinalDocument31 pagesInfertile Couple - Role of Ultrasound FinalKalpavriksha1974No ratings yet
- Re Examining Sonographic Cut Off Values For Diagnosing Early Pregnancy Loss 2161 0932.1000141Document4 pagesRe Examining Sonographic Cut Off Values For Diagnosing Early Pregnancy Loss 2161 0932.1000141Kalpavriksha1974No ratings yet
- 2018 Kalpavriksha Round 2 Junior Group 2 Question PaperDocument12 pages2018 Kalpavriksha Round 2 Junior Group 2 Question PaperKalpavriksha1974No ratings yet
- Second Trimester Scanning With Pictorial RepresentationDocument16 pagesSecond Trimester Scanning With Pictorial RepresentationKalpavriksha1974No ratings yet
- Genetic Screening For Markers in Second TrimesterDocument8 pagesGenetic Screening For Markers in Second TrimesterKalpavriksha1974No ratings yet
- Investigating and Managing Non-immune Fetal HydropsDocument14 pagesInvestigating and Managing Non-immune Fetal HydropsMariana González DíazNo ratings yet
- Fetal Ocular Distance in Normal PregnanciesDocument5 pagesFetal Ocular Distance in Normal PregnanciesKalpavriksha1974No ratings yet
- CMV VirusDocument8 pagesCMV VirusKalpavriksha1974No ratings yet
- Detailed Fetal ExaminationsDocument7 pagesDetailed Fetal ExaminationsKalpavriksha1974No ratings yet
- Ductus Venosus in First TrimesterDocument7 pagesDuctus Venosus in First TrimesterKalpavriksha1974No ratings yet
- Fetal Cardiac ArrythmiasDocument61 pagesFetal Cardiac ArrythmiasKalpavriksha1974No ratings yet
- Hospital LetterDocument1 pageHospital LetterKalpavriksha1974No ratings yet
- 11 - 14 Weeks ScanDocument10 pages11 - 14 Weeks ScanKalpavriksha1974No ratings yet
- Fetal Kidney HydronephrosisDocument6 pagesFetal Kidney HydronephrosisKalpavriksha1974No ratings yet
- Injso11 QPDocument22 pagesInjso11 QPKalpavriksha1974No ratings yet
- Detailed Fetal ExaminationsDocument7 pagesDetailed Fetal ExaminationsKalpavriksha1974No ratings yet
- Inbo13 QuestionDocument40 pagesInbo13 QuestionKalpavriksha1974No ratings yet
- QUIZ Guidelines QDocument3 pagesQUIZ Guidelines QKalpavriksha1974No ratings yet