You might also like
- Blood Transfusion - Hatem AlsrourDocument18 pagesBlood Transfusion - Hatem Alsrourhatem alsrour100% (2)
- Thoracic and Neck TraumaDocument13 pagesThoracic and Neck Traumahatem alsrourNo ratings yet
- Bipolar DisorderDocument19 pagesBipolar Disorderhatem alsrourNo ratings yet
- Abdominal TraumaDocument8 pagesAbdominal Traumahatem alsrour100% (2)
- Triage in Emergency DepartmentDocument25 pagesTriage in Emergency Departmenthatem alsrour91% (11)
- Common Drugs Used in The EmergencyDocument5 pagesCommon Drugs Used in The Emergencyhatem alsrour88% (25)
- Sexually Transmitted DiseasesDocument13 pagesSexually Transmitted Diseaseshatem alsrour100% (2)
- Ventricular Arrhythmia - Hatem AlsrourDocument31 pagesVentricular Arrhythmia - Hatem Alsrourhatem alsrour100% (3)
- Crash Cart - Cardioversion & Defebrilation - Hatem AlsrourDocument17 pagesCrash Cart - Cardioversion & Defebrilation - Hatem Alsrourhatem alsrour100% (2)
- Musculoskeletal TraumaDocument12 pagesMusculoskeletal Traumahatem alsrour100% (1)
- Positive & Negative Symptoms of SchizophreniaDocument1 pagePositive & Negative Symptoms of Schizophreniahatem alsrourNo ratings yet
- Needle Cricothyroidotomy 2 - Hatem AlsrourDocument32 pagesNeedle Cricothyroidotomy 2 - Hatem Alsrourhatem alsrour100% (2)
- Diagnostic Peritoneal Lavage (DPL)Document10 pagesDiagnostic Peritoneal Lavage (DPL)hatem alsrour100% (2)
- Escharotomy Incisions: Hatem AlsrourDocument28 pagesEscharotomy Incisions: Hatem Alsrourhatem alsrour100% (3)
- Common Emergency DrugsDocument58 pagesCommon Emergency Drugshatem alsrour84% (19)
- The Cast and SplintsDocument18 pagesThe Cast and Splintshatem alsrour100% (2)
- Spinal Immobilization - Hatem AlsrourDocument22 pagesSpinal Immobilization - Hatem Alsrourhatem alsrour100% (2)
- Needle CricothyroidotomyDocument9 pagesNeedle Cricothyroidotomyhatem alsrour100% (2)
- Spinal Immobilization: By: Hatem AlsrourDocument16 pagesSpinal Immobilization: By: Hatem Alsrourhatem alsrour100% (2)
- King Saud University College of NursingDocument24 pagesKing Saud University College of Nursinghatem alsrour100% (2)
- Burns & EscharotomyDocument36 pagesBurns & Escharotomyhatem alsrour100% (2)
- King Saud University College of NursingDocument49 pagesKing Saud University College of Nursinghatem alsrour100% (2)
- Bites & StingsDocument13 pagesBites & Stingshatem alsrour100% (2)
- Blood Transfusion - Hatem AlsrourDocument18 pagesBlood Transfusion - Hatem Alsrourhatem alsrour100% (2)
- Arrhythmia: King Saud University College of NursingDocument24 pagesArrhythmia: King Saud University College of Nursinghatem alsrour100% (2)
- King Saud University College of Nursing Gorwth & DevelopmentDocument16 pagesKing Saud University College of Nursing Gorwth & Developmenthatem alsrour100% (6)
- Sexually Transmitted DiseasesDocument13 pagesSexually Transmitted Diseaseshatem alsrour100% (2)
- Crash CartDocument55 pagesCrash Carthatem alsrour100% (4)
- Vitamin Active Form Function Deficiency Disease Precursor Hypervitamin Osis SourcesDocument3 pagesVitamin Active Form Function Deficiency Disease Precursor Hypervitamin Osis Sourceshatem alsrour100% (4)
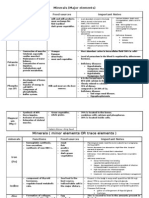
- Minerals (Major Elements) : Minera Ls Functions Food Sources Important NotesDocument3 pagesMinerals (Major Elements) : Minera Ls Functions Food Sources Important Noteshatem alsrour100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- A General Overview of Post Extraction Complicationsprevention Management and Importance of Post Extraction AdvicesDocument13 pagesA General Overview of Post Extraction Complicationsprevention Management and Importance of Post Extraction AdvicesBilqist Savannah PutriNo ratings yet
- 1700 Questions Not in PLABABLEDocument131 pages1700 Questions Not in PLABABLEDaniah Marwan Dawood DAWOODNo ratings yet
- Word List UrinalysisDocument2 pagesWord List Urinalysischerry100% (1)
- Đề Số 22 Có Giải Chi TiếtDocument17 pagesĐề Số 22 Có Giải Chi TiếtHuong Giang PhungNo ratings yet
- Visitors Personal Declaration Form - COVID 19Document1 pageVisitors Personal Declaration Form - COVID 19Leoni FrancNo ratings yet
- Mitochondrial Disorders A Review of Anesthetic ConsiderationsDocument10 pagesMitochondrial Disorders A Review of Anesthetic ConsiderationsSanaNo ratings yet
- 3D Echocardiography-CRC Press (2020)Document289 pages3D Echocardiography-CRC Press (2020)sainal edi kamalNo ratings yet
- ACMG Classification of Sequence VariantsDocument4 pagesACMG Classification of Sequence VariantsDienatha Sekar BuanaNo ratings yet
- Written Assignment 1 HSNS171 Fundamentals of Nursing Practice 1 Word Count: 973Document7 pagesWritten Assignment 1 HSNS171 Fundamentals of Nursing Practice 1 Word Count: 973Sophie Anderson0% (1)
- 7381-Article Text-34752-1-10-20230316Document10 pages7381-Article Text-34752-1-10-20230316jihan OktafianiNo ratings yet
- Perfor M Ance-Enhancing DrugsDocument112 pagesPerfor M Ance-Enhancing Drugszakaria zakariyaNo ratings yet
- Grade 11 FOODFISH TVL Q3WK7-8Document24 pagesGrade 11 FOODFISH TVL Q3WK7-8janeNo ratings yet
- Cardiothoracic SurgeryDocument24 pagesCardiothoracic SurgeryMARTINNo ratings yet
- Tirads PDFDocument8 pagesTirads PDFElio Emil Córdova VillarNo ratings yet
- Censoring Issues in Survival Analysis: Kwan-Moon Leung, Robert M. Elashoff, and Abdelmonem A. AfifiDocument22 pagesCensoring Issues in Survival Analysis: Kwan-Moon Leung, Robert M. Elashoff, and Abdelmonem A. AfifiLili MolinaNo ratings yet
- Evaluation of Antimicrobial Activity of ZITRITIDEDocument16 pagesEvaluation of Antimicrobial Activity of ZITRITIDEednisoNo ratings yet
- Nursing Care of Clients Nursing Care of Clients With Altered Ventilatory With Altered Ventilatory Function FunctionDocument179 pagesNursing Care of Clients Nursing Care of Clients With Altered Ventilatory With Altered Ventilatory Function FunctionPia Rose RoqueNo ratings yet
- Case Study On Chronic Kidney DiseaseDocument101 pagesCase Study On Chronic Kidney DiseaseZNEROL100% (6)
- Dafpus YasinDocument2 pagesDafpus YasinYusuf Arif SalamNo ratings yet
- Environmental Streptococci and Enterococcus Spp. - A Practical Summary For Controlling Mastitis - VirginiaAg DASC-7P (2012)Document2 pagesEnvironmental Streptococci and Enterococcus Spp. - A Practical Summary For Controlling Mastitis - VirginiaAg DASC-7P (2012)userNo ratings yet
- Stress and Its Coping Strategies Among The CaregiverDocument28 pagesStress and Its Coping Strategies Among The CaregiverSandesh BaralNo ratings yet
- Herbal Medicine For EveryoneDocument63 pagesHerbal Medicine For EveryoneMaratus Solehah100% (2)
- Lumbar PunctureDocument3 pagesLumbar PunctureKarsten RohlfsNo ratings yet
- Contents - 2016 - Veterinary Clinics of North America Food Animal Practice PDFDocument4 pagesContents - 2016 - Veterinary Clinics of North America Food Animal Practice PDFfelipeNo ratings yet
- Enhanced Recovery After Surgery: It's Time To Change Practice!Document12 pagesEnhanced Recovery After Surgery: It's Time To Change Practice!Anditha Namira RSNo ratings yet
- Mupirocin Drug StudyDocument1 pageMupirocin Drug StudyArthur Christopher Corpuz0% (1)
- The Human Immune SystemDocument24 pagesThe Human Immune Systemmilka berhaneNo ratings yet
- Developmental Disorders of The Gallbladder, Extrahepatic Biliary Tract, and PancreasDocument1 pageDevelopmental Disorders of The Gallbladder, Extrahepatic Biliary Tract, and PancreasbloodsphereNo ratings yet
- Immunohistochemical MarkersDocument12 pagesImmunohistochemical MarkersAsmara SyedNo ratings yet
- MSC Dissertation Cover PageDocument5 pagesMSC Dissertation Cover PageSomeoneToWriteMyPaperSingapore100% (1)