You might also like
- Amniotic PhysioDocument3 pagesAmniotic PhysiobjfieroNo ratings yet
- Sin Título 2Document16 pagesSin Título 2Anilu ApNo ratings yet
- Amniotic Fluid Water Dynamics: M.H. Beall, J.P.H.M. Van Den Wijngaard, M.J.C. Van Gemert, M.G. RossDocument8 pagesAmniotic Fluid Water Dynamics: M.H. Beall, J.P.H.M. Van Den Wijngaard, M.J.C. Van Gemert, M.G. RossCorín AnelNo ratings yet
- Amniotic Fluid As A Vital Sign For Fetal Wellbeing: ReviewDocument9 pagesAmniotic Fluid As A Vital Sign For Fetal Wellbeing: ReviewMeska AmeliaNo ratings yet
- Physiology of Amniotic Fluid Volume RegulationDocument8 pagesPhysiology of Amniotic Fluid Volume RegulationYosep SutandarNo ratings yet
- Chapter 2Document23 pagesChapter 2Shoroq El BeshbeshyNo ratings yet
- Romzan Alfiriza R (2018) Maryo Juan L.T (2018) Sarah Safrilia (201810401011007)Document22 pagesRomzan Alfiriza R (2018) Maryo Juan L.T (2018) Sarah Safrilia (201810401011007)SarahNo ratings yet
- Hydra Mi NosDocument8 pagesHydra Mi NosSudha DeviNo ratings yet
- Pathophysiology of hydrops fetalis and the role of atrial natriuretic peptideDocument25 pagesPathophysiology of hydrops fetalis and the role of atrial natriuretic peptidePandu Nugroho KantaNo ratings yet
- Placental Anatomy and Physiology: Ppds Basic 2019Document31 pagesPlacental Anatomy and Physiology: Ppds Basic 2019Andre Putra100% (1)
- 16 Cardiorespiratory Adjustments at Birth: IntroductionDocument43 pages16 Cardiorespiratory Adjustments at Birth: IntroductionJenny MendozaNo ratings yet
- Please Focus On uWISE Questions As Your Main Study Material and You Can Use This Study Guide As A Reference. Female Reproductive PhysiologyDocument131 pagesPlease Focus On uWISE Questions As Your Main Study Material and You Can Use This Study Guide As A Reference. Female Reproductive PhysiologyhevinpatelNo ratings yet
- Vaginal Fluid SimulantDocument5 pagesVaginal Fluid Simulantluck2livNo ratings yet
- Transient Tachypnea of The Newborn: Pediatrics in Review December 2008Document10 pagesTransient Tachypnea of The Newborn: Pediatrics in Review December 2008Haneen Dabbas2019No ratings yet
- Neonatology: Addisu Aa (Lecturer, MSC in CM)Document35 pagesNeonatology: Addisu Aa (Lecturer, MSC in CM)Abiy AliyeNo ratings yet
- Amniotic FluidDocument55 pagesAmniotic FluidRoselle Joy D. RosalejosNo ratings yet
- Kurjak PerinatologijaDocument2,753 pagesKurjak PerinatologijaSante PlusNo ratings yet
- لقطة شاشة ٢٠٢٣-٠٨-٠٤ في ٠٧.٥٥.٠٤Document51 pagesلقطة شاشة ٢٠٢٣-٠٨-٠٤ في ٠٧.٥٥.٠٤Nour RadhiNo ratings yet
- Amniotic FluidDocument33 pagesAmniotic FluidElsa Aprillia SujadiNo ratings yet
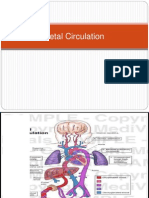
- Fetal CirculationDocument28 pagesFetal CirculationNelai GoNo ratings yet
- Non-Inmune Hrdrops Fetalis. A Short Review of Etiology and PathophysiologyDocument9 pagesNon-Inmune Hrdrops Fetalis. A Short Review of Etiology and PathophysiologyJuan Manuel RosasNo ratings yet
- Ultrasound in Obstet Gyne - 2005 - Jauniaux - The Role of Ultrasound Imaging in Diagnosing and Investigating EarlyDocument12 pagesUltrasound in Obstet Gyne - 2005 - Jauniaux - The Role of Ultrasound Imaging in Diagnosing and Investigating EarlySofiat WahabNo ratings yet
- Ectopic Pregnancy With Special Reference To Tubal Pregnancy and IDocument52 pagesEctopic Pregnancy With Special Reference To Tubal Pregnancy and IAbishaNo ratings yet
- Califmed00263 0071Document4 pagesCalifmed00263 0071Musdalifah MimousNo ratings yet
- 11th Lecture Amnion& Amniotic FluidDocument35 pages11th Lecture Amnion& Amniotic FluidHussein Al Saedi100% (1)
- Amniotic Fluid and Its Abnormality: DefinitionDocument7 pagesAmniotic Fluid and Its Abnormality: DefinitionpebripulunganNo ratings yet
- Amniotic FluidsDocument7 pagesAmniotic FluidsMazlina MaidinNo ratings yet
- Antenatal Physiotherapy Care GuideDocument77 pagesAntenatal Physiotherapy Care Guides_saikalyanNo ratings yet
- Resiratory Disorders in The NewbornDocument36 pagesResiratory Disorders in The NewbornRaquel CarvalhoNo ratings yet
- The Retained Placenta: Andrew D WeeksDocument7 pagesThe Retained Placenta: Andrew D WeeksrifkialbanaNo ratings yet
- Chapter 3 (Final)Document14 pagesChapter 3 (Final)Pureza Maye SalapangNo ratings yet
- Circulatia FetalaDocument6 pagesCirculatia FetalaVasile IsipNo ratings yet
- Transition To Extrauterine LifeDocument2 pagesTransition To Extrauterine LifeGerry SupitNo ratings yet
- Asfixia NeonatalDocument14 pagesAsfixia NeonatalValeria CuellarNo ratings yet
- Scenario Plenary Discussion: Trigger 1Document11 pagesScenario Plenary Discussion: Trigger 1andretegarNo ratings yet
- Balance de Agua en El Feto y El Recién NacidoDocument5 pagesBalance de Agua en El Feto y El Recién NacidoCarlos ReveloNo ratings yet
- Canubas Patent UrachusDocument16 pagesCanubas Patent UrachusLaly Rose CanubasNo ratings yet
- Tenny Parker Change A Reflection of Placental Pathology PDFDocument4 pagesTenny Parker Change A Reflection of Placental Pathology PDFEditors100% (1)
- Disorders in Amniotic FluidDocument5 pagesDisorders in Amniotic FluidLatansa DinaNo ratings yet
- Emedecine Neonatology 2006 PDFDocument540 pagesEmedecine Neonatology 2006 PDFNovi SeptianiNo ratings yet
- Lec 4Document6 pagesLec 4ibrahim.21hm32No ratings yet
- Delivery of PlacentaDocument8 pagesDelivery of PlacentaAbdullahi Suleiman MakaNo ratings yet
- Seminars in Fetal and Neonatal Medicine: Stuart B. Hooper, Calum Roberts, Janneke Dekker, Arjan B. Te PasDocument8 pagesSeminars in Fetal and Neonatal Medicine: Stuart B. Hooper, Calum Roberts, Janneke Dekker, Arjan B. Te PaskiloNo ratings yet
- Physiological Changes in PregnancyDocument35 pagesPhysiological Changes in PregnancyRocio SandersNo ratings yet
- Macleod 1Document8 pagesMacleod 1rakibhossainNo ratings yet
- Maternal Placental Foetal UnitDocument10 pagesMaternal Placental Foetal UnitFestus SinoNo ratings yet
- Bovine Reproduction Booklet UK A5 16pp Text 10Document20 pagesBovine Reproduction Booklet UK A5 16pp Text 10lenn chandNo ratings yet
- From The Journal of The American Academy of PediatricsDocument10 pagesFrom The Journal of The American Academy of PediatricsMichi MichNo ratings yet
- Physiologic Transition From Intrauterine To Extrauterine LifeDocument12 pagesPhysiologic Transition From Intrauterine To Extrauterine Lifeyhojar PisfilNo ratings yet
- Physiologic Transition From Intrauterine To Extrauterine Life - UpToDateDocument7 pagesPhysiologic Transition From Intrauterine To Extrauterine Life - UpToDateGuilherme Kazuo OgawaNo ratings yet
- Structure and Functions of the PlacentaDocument21 pagesStructure and Functions of the PlacentaAttiqaQureshiNo ratings yet
- 2006 7 E292-E299 William M. Gilbert: Amniotic Fluid DynamicsDocument10 pages2006 7 E292-E299 William M. Gilbert: Amniotic Fluid DynamicsMel MurNo ratings yet
- (Shared) FINAL Placenta Dan Sirkulasi TransisiDocument25 pages(Shared) FINAL Placenta Dan Sirkulasi Transisitwo_riskNo ratings yet
- Aps 201159Document5 pagesAps 201159Alvin JiwonoNo ratings yet
- The Amnion and Amniotic FluidDocument7 pagesThe Amnion and Amniotic FluidMerina FirmansahNo ratings yet
- Amnioticfluid 120212085244 Phpapp01Document43 pagesAmnioticfluid 120212085244 Phpapp01Jhoanie Sanggoy TauliNo ratings yet
- Cord ProlapseDocument4 pagesCord ProlapseCleta Escabarte Dehlin100% (1)
- Resuscitation of The Depressed Newborn: Raleigh, North CarolinaDocument6 pagesResuscitation of The Depressed Newborn: Raleigh, North CarolinaJoulo YabutNo ratings yet
- Diagnosing Heart FailureDocument26 pagesDiagnosing Heart FailureJessica StephanieNo ratings yet
- Prof. Wayan Hypertension - The Cardiovascular ContinuumDocument30 pagesProf. Wayan Hypertension - The Cardiovascular ContinuumJessica StephanieNo ratings yet
- Diagnostic Approach To Palpitations (Dr. Margono)Document27 pagesDiagnostic Approach To Palpitations (Dr. Margono)Jessica StephanieNo ratings yet
- Dabigatran in Primary SPAFDocument9 pagesDabigatran in Primary SPAFJessica StephanieNo ratings yet
- APC&VPC Treatv It or Leave ItDocument42 pagesAPC&VPC Treatv It or Leave ItJessica StephanieNo ratings yet
- Dr. Irsad Andi From Hypertension To Heart FailureDocument48 pagesDr. Irsad Andi From Hypertension To Heart FailureJessica StephanieNo ratings yet
- Clinical Challange of BradycardiaDocument48 pagesClinical Challange of BradycardiaJessica StephanieNo ratings yet
- Dr. Dyana Statin in Chronic Complex PatientsDocument37 pagesDr. Dyana Statin in Chronic Complex PatientsJessica StephanieNo ratings yet
- Cyanotic Congenital Heart DiseaseDocument80 pagesCyanotic Congenital Heart DiseaseJessica StephanieNo ratings yet
- Clinical Use of BloodDocument221 pagesClinical Use of BloodRizma Adlia100% (1)
- What's New in Lipid GuidelinesDocument31 pagesWhat's New in Lipid GuidelinesYunita WidyaningsihNo ratings yet
- Dr. Budhi Setianto Dyslipidemia and AtheroclerosisDocument25 pagesDr. Budhi Setianto Dyslipidemia and AtheroclerosisYunita WidyaningsihNo ratings yet
- Q (FG'RR - DB Bli Ot' Tlroh': /ta TrsDocument1 pageQ (FG'RR - DB Bli Ot' Tlroh': /ta TrsJessica StephanieNo ratings yet
- Dr. M. Ridwan The Role of Exercise Training in Cardiometabolic Disorder - Dr. Ridwan SPJP - Inaprevent3 - FINALDocument29 pagesDr. M. Ridwan The Role of Exercise Training in Cardiometabolic Disorder - Dr. Ridwan SPJP - Inaprevent3 - FINALJessica StephanieNo ratings yet
- Textbook of Pleural Diseases 2008 PDFDocument673 pagesTextbook of Pleural Diseases 2008 PDFJessica StephanieNo ratings yet
- Ho GG/: BT/ T"ap 4 Lut4uli$ L."KDocument1 pageHo GG/: BT/ T"ap 4 Lut4uli$ L."KJessica StephanieNo ratings yet
- Dr. Cholid Is Hypertension Preventable DiseaseDocument31 pagesDr. Cholid Is Hypertension Preventable DiseaseJessica StephanieNo ratings yet
- CER60 Glaucoma-Treatment 20120524Document443 pagesCER60 Glaucoma-Treatment 20120524Jessica StephanieNo ratings yet
- Clinical Use of BloodDocument221 pagesClinical Use of BloodRizma Adlia100% (1)
- Clinical Use of BloodDocument221 pagesClinical Use of BloodRizma Adlia100% (1)
- T/etcll (Ec: at 9eo, Tec. Fioba$ Tmu Tto !C"W)Document1 pageT/etcll (Ec: at 9eo, Tec. Fioba$ Tmu Tto !C"W)Jessica StephanieNo ratings yet
- Iln-.9O1 / R T, Ir.E (H Llarr: Naiifn"./ - MG - I ..Document1 pageIln-.9O1 / R T, Ir.E (H Llarr: Naiifn"./ - MG - I ..Jessica StephanieNo ratings yet
- RadiksDocument1 pageRadiksJessica StephanieNo ratings yet
- Ancient Chinese Philosopher Laozi BiographyDocument1 pageAncient Chinese Philosopher Laozi BiographyJessica StephanieNo ratings yet
- Yuli 1Document1 pageYuli 1Jessica StephanieNo ratings yet
- Neuropati 3 + PleksusDocument1 pageNeuropati 3 + PleksusJessica StephanieNo ratings yet
- Traumatic Bone Fracture and Nerve Injury Diagnosis and TreatmentDocument1 pageTraumatic Bone Fracture and Nerve Injury Diagnosis and TreatmentJessica StephanieNo ratings yet
- T3q R. Uilil F' Ffi: Dl$obqlDocument1 pageT3q R. Uilil F' Ffi: Dl$obqlJessica StephanieNo ratings yet
- Neuropati 1Document1 pageNeuropati 1Jessica StephanieNo ratings yet
- Madhya Pradesh Pharmaceutical Companies ListDocument21 pagesMadhya Pradesh Pharmaceutical Companies ListvivekNo ratings yet
- Sepsis NeonatorumDocument3 pagesSepsis NeonatorumKim TranateNo ratings yet
- Medical Surgical Nursing Test VIIDocument7 pagesMedical Surgical Nursing Test VIIclobregasNo ratings yet
- Lumineer Doctors GuideDocument24 pagesLumineer Doctors Guideahm4dentNo ratings yet
- Innovation at 3M CorporationDocument28 pagesInnovation at 3M CorporationTina NugraheniNo ratings yet
- Material Safety Data Sheet: 1. Product and Company IdentificationDocument4 pagesMaterial Safety Data Sheet: 1. Product and Company IdentificationDisco17No ratings yet
- Material Safety Data Sheet (MSDS)Document22 pagesMaterial Safety Data Sheet (MSDS)OladimejiNo ratings yet
- FCPS ComplaintDocument56 pagesFCPS Complaintwamu885100% (1)
- The Roles of Adolescents ' Emotional Problems and Social Media Addiction On Their Self-EsteemDocument10 pagesThe Roles of Adolescents ' Emotional Problems and Social Media Addiction On Their Self-EsteemVince Raeden AmaranteNo ratings yet
- 8 Eng Model Paper Feb 2022Document4 pages8 Eng Model Paper Feb 2022tocasNo ratings yet
- Kahren S. Reantaso RN ResumeDocument4 pagesKahren S. Reantaso RN ResumeKahren ReantasoNo ratings yet
- Impact of Covid-19 on Ethiopia's Tourism and Hotel IndustryDocument6 pagesImpact of Covid-19 on Ethiopia's Tourism and Hotel IndustryFuadNo ratings yet
- Store Employee Safety Handbook: Dear Dollar General EmployeeDocument6 pagesStore Employee Safety Handbook: Dear Dollar General EmployeeLaura HugginsNo ratings yet
- Rapidplan™ Knowledge-Based Planning: BrainDocument5 pagesRapidplan™ Knowledge-Based Planning: BrainolgaNo ratings yet
- VerbalReasoningTest10 Solutions PDFDocument13 pagesVerbalReasoningTest10 Solutions PDFAdewale QuadriNo ratings yet
- Standardi EvropskiDocument25 pagesStandardi EvropskiAna Safranec VasicNo ratings yet
- Aisyah GDM ArticleDocument18 pagesAisyah GDM ArticleBesari Md DaudNo ratings yet
- Grade 7 Cosme - Nail DiseasesDocument22 pagesGrade 7 Cosme - Nail DiseasesLigaya PastorNo ratings yet
- Leptospirosis: An Overview of Epidemiology, Clinical Features and Diagnosis in MalaysiaDocument57 pagesLeptospirosis: An Overview of Epidemiology, Clinical Features and Diagnosis in Malaysiawoihon50% (2)
- POULTRY FARM OPERATION AND LAB TECHNIQUES REPORTDocument30 pagesPOULTRY FARM OPERATION AND LAB TECHNIQUES REPORTBakhtawarNo ratings yet
- Revalida 1Document3 pagesRevalida 1herrabiel solisNo ratings yet
- DELHI PPN LIST HOSPITALS WITH 44 HOSPITAL DETAILSDocument20 pagesDELHI PPN LIST HOSPITALS WITH 44 HOSPITAL DETAILSLOGICAL YTNo ratings yet
- ICS Course Introduces Incident Management SystemDocument22 pagesICS Course Introduces Incident Management SystemMessias PortoNo ratings yet
- Shreya Rajesh - Case Study AnalysisDocument1 pageShreya Rajesh - Case Study AnalysisshreyaNo ratings yet
- "The Life and Times of Mr. Nicholls" Michael George Nicholls-Pierce Liberal Studies LIBS 390-01 Intellectual AutobiographyDocument5 pages"The Life and Times of Mr. Nicholls" Michael George Nicholls-Pierce Liberal Studies LIBS 390-01 Intellectual Autobiographyapi-573024890No ratings yet
- Relationships Remedies HomoeopathyDocument3 pagesRelationships Remedies HomoeopathyVijay KumarNo ratings yet
- Pae-Central Nervous SystemDocument17 pagesPae-Central Nervous SystemMegha ProjectsNo ratings yet
- Unit IG2: Risk AssessmentDocument22 pagesUnit IG2: Risk AssessmentMohammad Awees SanadiNo ratings yet
- Rogue Trader - Converted Dark Heresy Psychic PowersDocument13 pagesRogue Trader - Converted Dark Heresy Psychic PowersDontNeed100% (2)
- Low-Dose Quetiapine in Schizophrenia: Meta-Analysis High-: The Psychiatrist OnlineDocument5 pagesLow-Dose Quetiapine in Schizophrenia: Meta-Analysis High-: The Psychiatrist OnlineMichael CoxNo ratings yet