You might also like
- Bipolar 1 Case PresentationDocument111 pagesBipolar 1 Case PresentationJhensczy Hazel Maye AlbaNo ratings yet
- A Nursing Case Study On: Alzheimer's DiseaseDocument22 pagesA Nursing Case Study On: Alzheimer's DiseaseJesslee Llanes100% (4)
- Bipolar CaseDocument41 pagesBipolar CaseEmariel Dulana25% (4)
- Case Study of DementiaDocument9 pagesCase Study of DementiaNsengimana Eric Maxigy0% (1)
- Alzheimer's Case Study: 74-Year-Old Woman With Memory LossDocument8 pagesAlzheimer's Case Study: 74-Year-Old Woman With Memory LossMaria Fatima CaminsNo ratings yet
- Case Study Paranoid SchizoDocument46 pagesCase Study Paranoid SchizoDiksha Sharma100% (1)
- Alzheimers Disease Case PresentationDocument41 pagesAlzheimers Disease Case Presentationkhate fonte100% (1)
- Case Study BipolarDocument22 pagesCase Study BipolarRobert de Guzman Jr.93% (29)
- Depression Care PlanDocument21 pagesDepression Care PlanDeepesh Divakaran100% (5)
- Mood Disorder Case PresentationDocument65 pagesMood Disorder Case PresentationRhomizal Mazali83% (6)
- Cholelithiasis Case StudyDocument51 pagesCholelithiasis Case StudyANCHAL SHARMANo ratings yet
- Nursing Case Study DementiaDocument21 pagesNursing Case Study DementiaBella WilliamsNo ratings yet
- Bipolar Case StudyDocument46 pagesBipolar Case StudyNissie Degulacion100% (1)
- Psy Case StudyDocument81 pagesPsy Case StudyIOM BNSNo ratings yet
- Case Study On SchizophreniaDocument21 pagesCase Study On SchizophreniaAdrian Mallar100% (1)
- Case StudyDocument8 pagesCase StudyAmberlynn Stolarski100% (2)
- Nursing Care for Schizophrenic PatientsDocument1 pageNursing Care for Schizophrenic PatientsMabhel Fatima Abayan EspinosaNo ratings yet
- Psychiatric Case Presentation: Praveenrajkumar Csu Junior InternDocument33 pagesPsychiatric Case Presentation: Praveenrajkumar Csu Junior InternRishi Du AgbugayNo ratings yet
- Bipolar Mood Disorder Case RevisionDocument11 pagesBipolar Mood Disorder Case RevisionEden Marie Francisco100% (1)
- Alzheimer Disease Case StudyDocument6 pagesAlzheimer Disease Case StudyWarren67% (3)
- 2.e.case Ctudy On BPADDocument9 pages2.e.case Ctudy On BPADManisa Parida100% (1)
- Schizophrenia Case StudyDocument8 pagesSchizophrenia Case Studyaira2350% (2)
- Case History ReportDocument27 pagesCase History Reportdivya100% (2)
- Case Study: On AlcoholismDocument50 pagesCase Study: On AlcoholismMonika100% (1)
- Case Study of Bipolar DisorderDocument1 pageCase Study of Bipolar DisorderIrene Mae Villanueva Ariola0% (1)
- 2.A Ndera CaseDocument14 pages2.A Ndera CaseNsengimana Eric MaxigyNo ratings yet
- MDD Case PresentationDocument84 pagesMDD Case PresentationReymund Timog TalarocNo ratings yet
- Case StudyDocument11 pagesCase Studyapi-507420243100% (1)
- Case Study of BronchoPneumoniaDocument64 pagesCase Study of BronchoPneumoniaJomari Zapanta100% (2)
- Case Study SchizopreniaDocument21 pagesCase Study SchizopreniaRay-ann Sorilla100% (1)
- Case Study BipolarDocument22 pagesCase Study BipolarMaria Visitacion100% (1)
- Anxiety NeurosisDocument34 pagesAnxiety Neurosisilakkiya ilakkiyaNo ratings yet
- Case Study on Severe Depression with PsychosisDocument33 pagesCase Study on Severe Depression with PsychosisPallavi KharadeNo ratings yet
- Cases Study On BipolarDocument37 pagesCases Study On BipolarjaoNo ratings yet
- Bipolar Affective Disorder, Manic Episode With PsychoticDocument30 pagesBipolar Affective Disorder, Manic Episode With PsychoticCharan Pal SinghNo ratings yet
- Paranoid Schizophrenia Case StudyDocument29 pagesParanoid Schizophrenia Case StudySimran Josan100% (3)
- Case Presentation of DepressionDocument39 pagesCase Presentation of DepressionMithun Dey71% (28)
- Case Presentation of Bipolar Affective Disorder, Current Episode, Manic With Psychotic DisorderDocument37 pagesCase Presentation of Bipolar Affective Disorder, Current Episode, Manic With Psychotic DisorderEarl John Natividad89% (9)
- Case Study On OCD: Sri Lakshmi College of NursingDocument49 pagesCase Study On OCD: Sri Lakshmi College of NursingveereshNo ratings yet
- Mental Case StudyDocument38 pagesMental Case StudyNishaThakuri75% (4)
- Schizophrenia Case StudyDocument24 pagesSchizophrenia Case StudyRichard Sy100% (3)
- Process Recording 2Document7 pagesProcess Recording 2Hardeep KaurNo ratings yet
- Undifferentiated SchizophreniaDocument190 pagesUndifferentiated Schizophreniaallexiscampaner100% (16)
- Case Study of Paranoid SchizophreniaDocument22 pagesCase Study of Paranoid SchizophreniaFloidas Fernando100% (8)
- Schizophrenia CaseDocument14 pagesSchizophrenia CaseFrancez Anne Guanzon100% (1)
- Bipolar Disorder Case StudyDocument14 pagesBipolar Disorder Case StudyValiant Baybay67% (3)
- Schizophrenia ParanoidDocument129 pagesSchizophrenia ParanoidhjhjhjkjkNo ratings yet
- Case Presentation On GadDocument38 pagesCase Presentation On GadBarjeesNo ratings yet
- Case Study For DementiaDocument51 pagesCase Study For DementiapogichannyNo ratings yet
- Pyomyositis (Ca1)Document66 pagesPyomyositis (Ca1)Emman Ramos60% (5)
- Mi Case StudyDocument27 pagesMi Case StudyMary Hope BacutaNo ratings yet
- Micu Case Study d1Document28 pagesMicu Case Study d1jmarc_2180% (5)
- AFPMC V. Luna General Hospital: Case StudyDocument27 pagesAFPMC V. Luna General Hospital: Case StudyLemuel GuevarraNo ratings yet
- Molar Pregnancy: Capitol Medical Center CollegesDocument38 pagesMolar Pregnancy: Capitol Medical Center CollegesDarlene Laude GoyaNo ratings yet
- 2 21 23 Capstone PaperDocument6 pages2 21 23 Capstone Paperapi-655053476No ratings yet
- Stress Insomnia OutputDocument18 pagesStress Insomnia OutputReyes PaulNo ratings yet
- Gamazon Jurwell - (Act 2 Bioethics)Document3 pagesGamazon Jurwell - (Act 2 Bioethics)Gino Carlo BrionesNo ratings yet
- Diabetes Mellitus Type 2Document20 pagesDiabetes Mellitus Type 2Kylie GolindangNo ratings yet
- ..Table of ContentsDocument40 pages..Table of ContentsJobelle AcenaNo ratings yet
- Vascular Dementia (Case Study)Document22 pagesVascular Dementia (Case Study)Coleen Mae CamaristaNo ratings yet
- Behavior Modification Therapy: An Evidence-Based Approach to Changing Unwanted Behaviors Through Reinforcement and ExtinctionDocument19 pagesBehavior Modification Therapy: An Evidence-Based Approach to Changing Unwanted Behaviors Through Reinforcement and ExtinctionJm OpolintoNo ratings yet
- WORD BM Case 1Document7 pagesWORD BM Case 1Jm OpolintoNo ratings yet
- Evaluation Tool From ADUDocument6 pagesEvaluation Tool From ADUJm OpolintoNo ratings yet
- Hiv LectureDocument1 pageHiv LectureJm OpolintoNo ratings yet
- Date Activity Accomplishment Hindering Factor/problem Encountered Solution RecommendationsDocument1 pageDate Activity Accomplishment Hindering Factor/problem Encountered Solution RecommendationsJm OpolintoNo ratings yet
- Process Recording ExampleDocument7 pagesProcess Recording ExampleCheska ت HortelanoNo ratings yet
- Documentation MethodsDocument1 pageDocumentation MethodsJm OpolintoNo ratings yet
- Care of Clients with Hidradenitis Suppurativa (Acne InversaDocument15 pagesCare of Clients with Hidradenitis Suppurativa (Acne InversaJm OpolintoNo ratings yet
- Community Organization DocumentationDocument71 pagesCommunity Organization DocumentationJm Opolinto100% (1)
- Gerontologic Nur - GIT ChangesDocument106 pagesGerontologic Nur - GIT ChangesJm OpolintoNo ratings yet
- Duties and ResponsibilitiesDocument1 pageDuties and ResponsibilitiesJm OpolintoNo ratings yet
- Psqi Sleep QuestionnaireDocument1 pagePsqi Sleep QuestionnaireOverSkyLordNo ratings yet
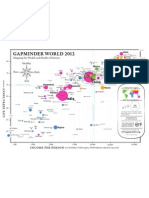
- Gapminder World 2012Document1 pageGapminder World 2012Diego DiegoteNo ratings yet
- IMIA EthicsDocument12 pagesIMIA EthicsJm OpolintoNo ratings yet
- FEU Kardex SampleDocument1 pageFEU Kardex SampleJm OpolintoNo ratings yet
- Prolapse of The Umbilical CordDocument13 pagesProlapse of The Umbilical CordJm OpolintoNo ratings yet
- AnesthesiaDocument2 pagesAnesthesiaJm OpolintoNo ratings yet
- Social Media ApplicationsDocument15 pagesSocial Media ApplicationsJm OpolintoNo ratings yet
- Last Holographic WillDocument2 pagesLast Holographic WillJenny Reyes50% (4)
- Revised Withholding Tax TablesDocument1 pageRevised Withholding Tax TablesJonasAblangNo ratings yet
- Ethics HIDocument10 pagesEthics HIbjnpedronptrpNo ratings yet
- Dying Person's Rights GuideDocument2 pagesDying Person's Rights GuideJm OpolintoNo ratings yet
- Nutrition WellnessDocument3 pagesNutrition WellnessJm OpolintoNo ratings yet
- Postpartum Behaviour As Predictor of Weight Change From Before Pregnancy To One Year PostpartumDocument8 pagesPostpartum Behaviour As Predictor of Weight Change From Before Pregnancy To One Year PostpartumJm OpolintoNo ratings yet
- Prolapse of The Umbilical CordDocument13 pagesProlapse of The Umbilical CordJm OpolintoNo ratings yet
- BandLslides JPGDocument100 pagesBandLslides JPGDanny RamosNo ratings yet
- Errors of RefractionDocument27 pagesErrors of RefractionAminaNo ratings yet
- Nama Cantik Gugus PhytagorasDocument2 pagesNama Cantik Gugus PhytagorasSaniihasannNo ratings yet
- Maternal & Child Care Nursing ReviewDocument37 pagesMaternal & Child Care Nursing Reviewɹǝʍdןnos98% (130)
- VIVA Training in ENTDocument8 pagesVIVA Training in ENTOpi PippoNo ratings yet
- About Medical ResearchDocument21 pagesAbout Medical ResearchMohebNo ratings yet
- Crps AbstractDocument32 pagesCrps AbstractroooNo ratings yet
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmkatNo ratings yet
- Tugas Terjemahan-Manajemen NyeriDocument50 pagesTugas Terjemahan-Manajemen NyeriNur MuawanaNo ratings yet
- Clinic Think FinalDocument6 pagesClinic Think FinalTop MusicNo ratings yet
- WOC CaseDocument4 pagesWOC Casedwi adindaNo ratings yet
- Pressure UlcersDocument43 pagesPressure UlcersZubda Butt100% (2)
- DIAGNOSISDocument44 pagesDIAGNOSISEgieAprianNo ratings yet
- Pilonodular Synovitis 2Document19 pagesPilonodular Synovitis 2Madhan Mohan Reddy KatikareddyNo ratings yet
- Instruction For The Students To The Station 6 ECG DiagnosticsDocument3 pagesInstruction For The Students To The Station 6 ECG DiagnosticsCynthia GNo ratings yet
- LECTURE 2 Biological Basis of BehaviorDocument74 pagesLECTURE 2 Biological Basis of BehaviorColossal HeartNo ratings yet
- Case Presentation 1Document4 pagesCase Presentation 1api-448765847No ratings yet
- ArpitDocument73 pagesArpitDurgesh PushkarNo ratings yet
- Gasem MH HANTA Salatiga 2019Document43 pagesGasem MH HANTA Salatiga 2019ChristianNo ratings yet
- Causes and Mechanisms of Acute Renal Injury and Chronic Kidney DiseaseDocument12 pagesCauses and Mechanisms of Acute Renal Injury and Chronic Kidney DiseaseCres Padua QuinzonNo ratings yet
- Acute Abdominal Pain History and Exam HPCDocument5 pagesAcute Abdominal Pain History and Exam HPCnaafNo ratings yet
- Im Board QuestionsDocument59 pagesIm Board QuestionsJulius Matthew LuzanaNo ratings yet
- Hemophilia, meningitis, and shunt care nursing questionsDocument5 pagesHemophilia, meningitis, and shunt care nursing questionsSherilNo ratings yet
- Long Case PresentationDocument3 pagesLong Case PresentationAkshat WaranNo ratings yet
- Clinical ECG RoundsDocument2 pagesClinical ECG RoundsKai Siang ChanNo ratings yet
- Anemia NotesDocument10 pagesAnemia NotesCYRUS CHEPKWONYNo ratings yet
- Addison's Disease: Symptoms, Causes, TreatmentDocument7 pagesAddison's Disease: Symptoms, Causes, TreatmentDexter DawsonNo ratings yet
- 2do Consenso Mexicano de AQEvDocument11 pages2do Consenso Mexicano de AQEvMlckey BarriosNo ratings yet
- Case 2 HydrocephalusDocument1 pageCase 2 HydrocephalusJasminKate SutacioNo ratings yet
- Neuro Passmedicin 2020Document1,102 pagesNeuro Passmedicin 2020Vikrant100% (1)