You might also like
- Motion To DismissDocument3 pagesMotion To DismissPam Ramos100% (1)
- Tutorial How To Run Panel Data Analysis by Using StataDocument21 pagesTutorial How To Run Panel Data Analysis by Using StataDian HendrawanNo ratings yet
- Persoalan N HipotesisDocument10 pagesPersoalan N HipotesisSchahyda ArleyNo ratings yet
- Knights of Rizal V DMCI HomesDocument1 pageKnights of Rizal V DMCI HomesPam RamosNo ratings yet
- Republic V MarcosDocument11 pagesRepublic V MarcosPam RamosNo ratings yet
- Health Systems Strengthening - The University of MelbourneDocument14 pagesHealth Systems Strengthening - The University of MelbourneEstefanía MariñoNo ratings yet
- Leadership Skills for the New Health Economy a 5Q© ApproachFrom EverandLeadership Skills for the New Health Economy a 5Q© ApproachNo ratings yet
- SAMAR II V SeludoDocument2 pagesSAMAR II V SeludoPam Ramos50% (2)
- Stonehill V DioknoDocument3 pagesStonehill V DioknoPam RamosNo ratings yet
- La Razon Social Vs Union InsuranceDocument2 pagesLa Razon Social Vs Union InsurancePam RamosNo ratings yet
- Health Economics 2Document4 pagesHealth Economics 2Rira Fauziah INo ratings yet
- Almeda v. Heirs of Ponciano AlmedaDocument1 pageAlmeda v. Heirs of Ponciano AlmedaPam RamosNo ratings yet
- Health Policy Developments 13: Focus on Health Policy in Times of Crisis, Competition and Regulation, Evaluation in Health CareFrom EverandHealth Policy Developments 13: Focus on Health Policy in Times of Crisis, Competition and Regulation, Evaluation in Health CareNo ratings yet
- Republic of The Philippines v. La OrdenDocument1 pageRepublic of The Philippines v. La OrdenPam Ramos100% (1)
- Legal MemorandumDocument2 pagesLegal MemorandumPam Ramos100% (2)
- Minitab Statguide MultivariateDocument25 pagesMinitab Statguide MultivariateSuraj singhNo ratings yet
- Health Affairs: For Reprints, Links & PermissionsDocument19 pagesHealth Affairs: For Reprints, Links & PermissionsitteNo ratings yet
- Health Care Systems: Getting More Value For Money: Economics Department Policy Note No. 2Document12 pagesHealth Care Systems: Getting More Value For Money: Economics Department Policy Note No. 2Hybird RyantoeNo ratings yet
- Health Budget DeterminantsDocument14 pagesHealth Budget DeterminantsAyo AlabiNo ratings yet
- 1 s2.0 S0140673615605748 MainDocument7 pages1 s2.0 S0140673615605748 Mainashakow8849No ratings yet
- Potential Savings Through Prevention of Avoidable Chronic Illness Among CalPERS State Active MembersDocument10 pagesPotential Savings Through Prevention of Avoidable Chronic Illness Among CalPERS State Active Membersjon_ortizNo ratings yet
- Assignment1 OCTOBER2023Document2 pagesAssignment1 OCTOBER2023nkvkdkmskNo ratings yet
- The Economics of Malnutrition: M. EliaDocument12 pagesThe Economics of Malnutrition: M. EliaolatoyosifolorunsoNo ratings yet
- Out-of-Pocket Expenditures On Health - WagstaffDocument35 pagesOut-of-Pocket Expenditures On Health - WagstaffFelipe MartinezNo ratings yet
- Literature Review - FinalDocument10 pagesLiterature Review - FinaloscarNo ratings yet
- Health Worker Remuneration in WHO Member StatesDocument9 pagesHealth Worker Remuneration in WHO Member StatesKukuh ArdianNo ratings yet
- Catastrophic Household Expenditure For Healthcare in Turkey: Clustering Analysis of Categorical DataDocument10 pagesCatastrophic Household Expenditure For Healthcare in Turkey: Clustering Analysis of Categorical DataErmiyasNo ratings yet
- Does Health Aid Reduce Mortality?: Brief 6 Sven WilsonDocument4 pagesDoes Health Aid Reduce Mortality?: Brief 6 Sven WilsonBruno AbarcaNo ratings yet
- Medical Tribune September 2012 PHDocument33 pagesMedical Tribune September 2012 PHAsmphLibrary OrtigasNo ratings yet
- The Suntory and Toyota International Centres For Economics and Related DisciplinesDocument11 pagesThe Suntory and Toyota International Centres For Economics and Related DisciplinesRotariu AlexandruNo ratings yet
- Paper 24Document38 pagesPaper 24ABEL KETEMANo ratings yet
- The Value of Life and The Rise in Health Spending: Robert E. HallDocument42 pagesThe Value of Life and The Rise in Health Spending: Robert E. HallBala SubraNo ratings yet
- Zero B Health Eco Health ReformDocument5 pagesZero B Health Eco Health ReformAnusha VergheseNo ratings yet
- Weil AccountingDocument59 pagesWeil AccountingMafeAcevedoNo ratings yet
- Thesis On Health Care FinancingDocument5 pagesThesis On Health Care Financingchristinawestcharleston100% (2)
- National Health AccountsDocument4 pagesNational Health AccountsMyat MinNo ratings yet
- Equity in Health Care Financing - The Case of MalaysiaDocument14 pagesEquity in Health Care Financing - The Case of MalaysiaAmir IejieNo ratings yet
- Gravelle - 77%Document20 pagesGravelle - 77%Nikos KadinosNo ratings yet
- DR Margaret Chan Director-General of The World Health OrganizationDocument7 pagesDR Margaret Chan Director-General of The World Health OrganizationEric Kwaku KegyaNo ratings yet
- The Grass Is Not Always Greener - Cato Institute Healthcare ReportDocument48 pagesThe Grass Is Not Always Greener - Cato Institute Healthcare ReportChris PostlethwaiteNo ratings yet
- Health Systems 2009 20aug ADocument74 pagesHealth Systems 2009 20aug ANational Child Health Resource Centre (NCHRC)No ratings yet
- C - U A I P T O I: OST Tility Nalyses of Nterventions TO Revent and Reat Besity in SraelDocument50 pagesC - U A I P T O I: OST Tility Nalyses of Nterventions TO Revent and Reat Besity in SraelMinda IANo ratings yet
- Tackling Out-Of-Pocket Health Care Costs A Discussion Paper: Lesley Russell Jennifer DoggettDocument15 pagesTackling Out-Of-Pocket Health Care Costs A Discussion Paper: Lesley Russell Jennifer DoggettLesley Russell100% (1)
- The Importance of Community Health in Economic Development: Pavel ChernyavskiyDocument18 pagesThe Importance of Community Health in Economic Development: Pavel ChernyavskiyFadli NoorNo ratings yet
- National Health Policy, 2017: Revealing Public Health ChicaneryDocument12 pagesNational Health Policy, 2017: Revealing Public Health ChicaneryRohan RegiNo ratings yet
- Healthcare Financing in South-East Asia: Does Fiscal Capacity Matter?Document11 pagesHealthcare Financing in South-East Asia: Does Fiscal Capacity Matter?DoctorRonZ7No ratings yet
- Anderson and Frogner Health Spending HA '08Document10 pagesAnderson and Frogner Health Spending HA '08Michelle WebbNo ratings yet
- Health FinancingDocument34 pagesHealth Financingfarmasi oenNo ratings yet
- Regression AnalysisDocument10 pagesRegression AnalysisHarsh DiwakarNo ratings yet
- Podcast IIDocument49 pagesPodcast IINumeratorNo ratings yet
- Health Economics IntroductionDocument25 pagesHealth Economics Introductionstallioncode5009No ratings yet
- Comparative Efficiency of National Healthcare Systems PDFDocument33 pagesComparative Efficiency of National Healthcare Systems PDFdelap05No ratings yet
- Topic: National Quality Stratergy: Student Name: Unit Code: University Name: DateDocument7 pagesTopic: National Quality Stratergy: Student Name: Unit Code: University Name: DateAmber PreetNo ratings yet
- KemerutDocument2 pagesKemerutFrance Nathaniel CanaleNo ratings yet
- Governance and Corruption in Public Health Care Systems: AbstractDocument23 pagesGovernance and Corruption in Public Health Care Systems: Abstracttenzin tsekyiNo ratings yet
- FICCI EY Report Healthcare ReportDocument72 pagesFICCI EY Report Healthcare Reportsh_niravNo ratings yet
- Health System Productivity in China: A Comparison of Pre-And Post-2009 Healthcare ReformDocument10 pagesHealth System Productivity in China: A Comparison of Pre-And Post-2009 Healthcare ReformMayra GualdronNo ratings yet
- Public and Private Expenditures On Health in A Growth Model JSDDocument17 pagesPublic and Private Expenditures On Health in A Growth Model JSDAnonymous qfU34ZNo ratings yet
- Comment: For Lancet On Universal Universal-Health-CoverageDocument2 pagesComment: For Lancet On Universal Universal-Health-Coverageapi-112905159No ratings yet
- Challenge For UhcDocument3 pagesChallenge For UhcSatyanarayan MeenaNo ratings yet
- Health Policy: BrazilDocument8 pagesHealth Policy: Brazilapi-112905159No ratings yet
- Research Paper in Health EconomicsDocument6 pagesResearch Paper in Health Economicscaqllprhf100% (1)
- Final Jonathan Akpede - Wa 3Document9 pagesFinal Jonathan Akpede - Wa 3api-458086610No ratings yet
- Medicines in Health Systems Working Toward UHC: Presentation ScriptDocument21 pagesMedicines in Health Systems Working Toward UHC: Presentation ScriptHananAhmedNo ratings yet
- Comparing Health System Performance in OECD CountriesDocument14 pagesComparing Health System Performance in OECD CountriesromanpollyNo ratings yet
- Community-Based Health Insurance in Developing CountriesDocument14 pagesCommunity-Based Health Insurance in Developing CountriesRakip MaloskiNo ratings yet
- Contracting Out AccessDocument14 pagesContracting Out AccessMuna Hassan MustafaNo ratings yet
- Determinantes Catastrophic HEALTCHPERUDocument12 pagesDeterminantes Catastrophic HEALTCHPERUJean M Huaman FiallegaNo ratings yet
- Invest in HealthDocument23 pagesInvest in HealthLevi SchneiderNo ratings yet
- What's Behind Out-Of-Control Us Health Care Spending?: The Evolution of U.S. Health Care Spending Post World War IiFrom EverandWhat's Behind Out-Of-Control Us Health Care Spending?: The Evolution of U.S. Health Care Spending Post World War IiNo ratings yet
- Republic V DomingoDocument9 pagesRepublic V DomingoPam RamosNo ratings yet
- Spouses Genato v. ViolaDocument8 pagesSpouses Genato v. ViolaPam RamosNo ratings yet
- Heirs of Sotto v. PalicteDocument9 pagesHeirs of Sotto v. PalictePam RamosNo ratings yet
- Ernesto Oppen Inc. v. CompasDocument6 pagesErnesto Oppen Inc. v. CompasPam RamosNo ratings yet
- Ley Construction v. SedanoDocument8 pagesLey Construction v. SedanoPam RamosNo ratings yet
- Heirs of Sotto v. PalicteDocument7 pagesHeirs of Sotto v. PalictePam RamosNo ratings yet
- AFP V RTCDocument1 pageAFP V RTCPam RamosNo ratings yet
- Ofilada v. Spouses AndalDocument12 pagesOfilada v. Spouses AndalPam RamosNo ratings yet
- People v. MupasDocument2 pagesPeople v. MupasPam RamosNo ratings yet
- People v. MupasDocument2 pagesPeople v. MupasPam RamosNo ratings yet
- Rep V Pimentel and in Re PNB v. US District Court For The District of HawaiiDocument11 pagesRep V Pimentel and in Re PNB v. US District Court For The District of HawaiiPam RamosNo ratings yet
- Statistical Functions of EZRDocument3 pagesStatistical Functions of EZRbudiutom8307No ratings yet
- Unit-5 RelDocument5 pagesUnit-5 Rel20AD022 KAMALI PRIYA SNo ratings yet
- Using R To Teach EconometricsDocument15 pagesUsing R To Teach Econometricsjojo liNo ratings yet
- Regression EquationDocument56 pagesRegression EquationMuhammad TariqNo ratings yet
- Hotelling's T2 PDFDocument12 pagesHotelling's T2 PDFscjofyWFawlroa2r06YFVabfbajNo ratings yet
- Machine Learning FOR Signal Processing: Sriramg@iisc - Ac.inDocument16 pagesMachine Learning FOR Signal Processing: Sriramg@iisc - Ac.inlubhawan pariharNo ratings yet
- Uts DeskriantiDocument10 pagesUts DeskriantiDeskrianti TanaemNo ratings yet
- The One Way AnovaDocument55 pagesThe One Way AnovaAmirmktNo ratings yet
- Two-Way ANOVA: C1 Versus C2, C3Document8 pagesTwo-Way ANOVA: C1 Versus C2, C3Nur Ain Ahmad FikriNo ratings yet
- CORRELATIONDocument4 pagesCORRELATIONAira SantosNo ratings yet
- Repeated Measures ANOVADocument41 pagesRepeated Measures ANOVANilaamChowNo ratings yet
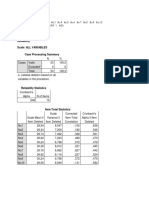
- Reliability Scale: All Variables Case Processing SummaryDocument5 pagesReliability Scale: All Variables Case Processing SummaryAmsal NasutionNo ratings yet
- Discriminant AnalysisDocument7 pagesDiscriminant AnalysisHisham ElhadidiNo ratings yet
- Naïve Method, Average of Historic Cost and Moving Average MethodDocument2 pagesNaïve Method, Average of Historic Cost and Moving Average Methodakshat gilraNo ratings yet
- Bnad 277 Final ProjectDocument11 pagesBnad 277 Final Projectapi-638728331No ratings yet
- Bahir Dar University: Ethiopian Institute of Textile and Fashion TechnologyDocument14 pagesBahir Dar University: Ethiopian Institute of Textile and Fashion TechnologyAnonymous PM3K4DNo ratings yet
- Linear Regression in R - R TutorialDocument33 pagesLinear Regression in R - R TutorialSai SanthoshNo ratings yet
- Domenella Lezma ReplicationDocument26 pagesDomenella Lezma ReplicationGonzalo Lezma FloridaNo ratings yet
- Pengaruh Modal Kerja Terhadap Laba Bersih Pada Pt. Perkebunan Nusantara Iv MedanDocument11 pagesPengaruh Modal Kerja Terhadap Laba Bersih Pada Pt. Perkebunan Nusantara Iv MedanDavid Clint MalessyNo ratings yet
- Multiple Linear Regression: BIOST 515 January 15, 2004Document32 pagesMultiple Linear Regression: BIOST 515 January 15, 2004HazemIbrahimNo ratings yet
- MclogitDocument19 pagesMclogitkyotopinheiroNo ratings yet
- SMChap 012Document15 pagesSMChap 012Anonymous uRz4Sb8m9eNo ratings yet
- A Zaenal Mufaqih - Tugas6Document6 pagesA Zaenal Mufaqih - Tugas6hexsbayNo ratings yet
- Practice FinalDocument16 pagesPractice FinalJessica ZhaiNo ratings yet
- Weather Trends Sales PredictorDocument6 pagesWeather Trends Sales PredictorWananda Muhammad RifkiNo ratings yet
- CvmsDocument37 pagesCvmsrealtorrobbinsmithNo ratings yet
- Statistical Properties of OLSDocument59 pagesStatistical Properties of OLSEvgenIy BokhonNo ratings yet