You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Blaker NUR 427 Contagion AnalysisDocument5 pagesBlaker NUR 427 Contagion AnalysisJenni CavanaughNo ratings yet
- Blaker NUR 427 Letter To LegislatorDocument3 pagesBlaker NUR 427 Letter To LegislatorJenni CavanaughNo ratings yet
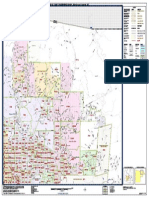
- Arizona Census Tract MapDocument1 pageArizona Census Tract MapJenni CavanaughNo ratings yet
- Hybrid SyllabusDocument22 pagesHybrid SyllabusJenni CavanaughNo ratings yet
- Maternal and Child Health Practice Test 3Document14 pagesMaternal and Child Health Practice Test 3Zeus Jherome ColigadoNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- History and Causology - DR - ShamolDocument265 pagesHistory and Causology - DR - ShamolUmer Farooq100% (1)
- Asthma and Ibuprofen: Effects, Risks, and AlternativesDocument6 pagesAsthma and Ibuprofen: Effects, Risks, and AlternativesYasIsaNo ratings yet
- Adult Invasive Mechanical VentilationDocument73 pagesAdult Invasive Mechanical Ventilationmed2004100% (1)
- Bexitrol F Dpi PDFDocument4 pagesBexitrol F Dpi PDFTahia Rahman JuhiNo ratings yet
- Health7 Q4 M1 v4Document31 pagesHealth7 Q4 M1 v4JEMAX SALANo ratings yet
- Nicl 2Document6 pagesNicl 2M Thoriq Al FathNo ratings yet
- Peds Final Exam Study GuideDocument47 pagesPeds Final Exam Study GuideSammy Levuong100% (1)
- NP IvDocument36 pagesNP IvZharina VillanuevaNo ratings yet
- What Causes COPD?Document4 pagesWhat Causes COPD?Adi PutraNo ratings yet
- AsthmaDocument16 pagesAsthmaRa DiantNo ratings yet
- Medical Devices in Allergy Practice - 2020 - WaojouDocument27 pagesMedical Devices in Allergy Practice - 2020 - WaojouJoão Pedro SantanaNo ratings yet
- Buteyko Breathing Manual - Stop Any Breathing Problems & Improve Health (PDFDrive)Document93 pagesButeyko Breathing Manual - Stop Any Breathing Problems & Improve Health (PDFDrive)Petra Jobova100% (1)
- Oral Medicine H UmarjiDocument299 pagesOral Medicine H UmarjiNekkanti sai shreyaNo ratings yet
- Audio ScriptDocument7 pagesAudio ScriptMohamed AliNo ratings yet
- AsthmaDocument26 pagesAsthmaIzzudin TarmiziNo ratings yet
- Biologic Therapies For Severe Asthma 2022Document15 pagesBiologic Therapies For Severe Asthma 2022Marina DomencoNo ratings yet
- Pe & Health Reviewer (1 Periodical) Module 1 Lesson 1: Physical FitnessDocument7 pagesPe & Health Reviewer (1 Periodical) Module 1 Lesson 1: Physical FitnessFitri CeradoNo ratings yet
- Traditional Zootherapeutic Uses in The Treatment of Asthma by The Ethnic Groups of Assam, IndiaDocument5 pagesTraditional Zootherapeutic Uses in The Treatment of Asthma by The Ethnic Groups of Assam, IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- It Is Now Time To Develop A Matrix To Assist in Case PreparationDocument8 pagesIt Is Now Time To Develop A Matrix To Assist in Case Preparationsabrina_kNo ratings yet
- Brand Plan - SingulairDocument11 pagesBrand Plan - Singulairshashank100% (2)
- Science 9 Q1 Module-3 For PrintingDocument31 pagesScience 9 Q1 Module-3 For PrintingRica Abigail DagosNo ratings yet
- Makalah Bahasa InggrisDocument15 pagesMakalah Bahasa Inggrisfera kartikaNo ratings yet
- COVID-19 - Myths and Facts - AvertDocument6 pagesCOVID-19 - Myths and Facts - AvertLuna BellatrixNo ratings yet
- Chest FinalDocument56 pagesChest FinalLwayNo ratings yet
- CME - Breathlessness RadDocument51 pagesCME - Breathlessness Radjun sianNo ratings yet
- Major Side Effects of Inhaled Glucocorticoids - UpToDateDocument37 pagesMajor Side Effects of Inhaled Glucocorticoids - UpToDateAmr MohamedNo ratings yet
- PED 027 Written ActDocument2 pagesPED 027 Written ActRowella Mae VillenaNo ratings yet
- SSC CGL & CHSL Exam 2015 GK Power CapsuleDocument37 pagesSSC CGL & CHSL Exam 2015 GK Power CapsuleNewstechcafeNo ratings yet
- Asthma and COPDDocument27 pagesAsthma and COPDTzaddi EaileyNo ratings yet
- ACEP Ketamine Guideline 2011Document13 pagesACEP Ketamine Guideline 2011Daniel Crook100% (1)