You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Antianxiety DrugsDocument41 pagesAntianxiety Drugsirina22_alessNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Death by SupermarketDocument355 pagesDeath by SupermarketWajihNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Evidence-Informed Primary Care Management of Low Back Pain - Clinical Practice Guideline - CanadaDocument49 pagesEvidence-Informed Primary Care Management of Low Back Pain - Clinical Practice Guideline - CanadaCambriaChicoNo ratings yet
- Practical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryDocument29 pagesPractical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryShahinaz ShamsNo ratings yet
- Anxiety DisordersDocument37 pagesAnxiety DisordersDr Dushyant Kamal Dhari75% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Exam Drug Sem 2 - 2021Document6 pagesExam Drug Sem 2 - 2021Achi Beridze100% (1)
- Lesson Plan DepressionDocument19 pagesLesson Plan DepressionRahul Kumar Diwakar100% (1)
- Kellogg Casebook 2001 For Case Interview Practice - MasterTheCaseDocument74 pagesKellogg Casebook 2001 For Case Interview Practice - MasterTheCaseMasterTheCase.comNo ratings yet
- PharmacologyAnesthesiology RevalidaDocument166 pagesPharmacologyAnesthesiology RevalidaKENT DANIEL SEGUBIENSE100% (1)
- IDSA Releases Guidance On Antibiotic Selection For Gram-Negative Antimicrobial-Resistant Bacterial Infections - ACP Internist Weekly - ACP InternistDocument3 pagesIDSA Releases Guidance On Antibiotic Selection For Gram-Negative Antimicrobial-Resistant Bacterial Infections - ACP Internist Weekly - ACP InternistStacey WoodsNo ratings yet
- Switching Ace-Inhibitors: Change To Change From Enalapril Quinapril RamiprilDocument2 pagesSwitching Ace-Inhibitors: Change To Change From Enalapril Quinapril RamiprilGlory Claudia KarundengNo ratings yet
- Management of Bacterial and Fungal Infections in Cirrhosis JOH 2021Document17 pagesManagement of Bacterial and Fungal Infections in Cirrhosis JOH 2021Francisco Javier Gonzalez NomeNo ratings yet
- Id 397 TeicoplaninDocument2 pagesId 397 TeicoplaninStacey WoodsNo ratings yet
- J Jacadv 2023 100389Document12 pagesJ Jacadv 2023 100389Edward ElBuenoNo ratings yet
- Therapeutic Drug Monitoring in Adults at NUH2011 FinalDocument2 pagesTherapeutic Drug Monitoring in Adults at NUH2011 FinalStacey WoodsNo ratings yet
- Antithrombotic Therapy For VTE DiseaseDocument13 pagesAntithrombotic Therapy For VTE DiseaseStacey WoodsNo ratings yet
- 2023 ESPEN Practical and Partially Revised Guideline - Clinical Nutrition in The Intensive Care UnitDocument19 pages2023 ESPEN Practical and Partially Revised Guideline - Clinical Nutrition in The Intensive Care UnitStacey WoodsNo ratings yet
- Splenectomy Guideline Final 2012Document6 pagesSplenectomy Guideline Final 2012Stacey WoodsNo ratings yet
- Palliative2 Nausea MedtableDocument2 pagesPalliative2 Nausea MedtableStacey WoodsNo ratings yet
- Appropriate Use of Laxatives in The Older PersonDocument7 pagesAppropriate Use of Laxatives in The Older PersonStacey WoodsNo ratings yet
- Critical CareDocument8 pagesCritical CareDzikrul Haq KarimullahNo ratings yet
- Antibiotik WhoDocument49 pagesAntibiotik WhodjebrutNo ratings yet
- Antibiotic Selection - The Clinical AdvisorDocument6 pagesAntibiotic Selection - The Clinical AdvisorStacey WoodsNo ratings yet
- Tamiflu PrescribingDocument26 pagesTamiflu PrescribingStacey WoodsNo ratings yet
- Multimorbidity Clinical Assessment and Management 1837516654789Document22 pagesMultimorbidity Clinical Assessment and Management 1837516654789Stacey WoodsNo ratings yet
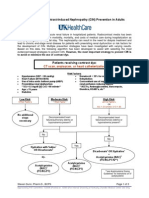
- Contrast NephRopathy GuidelinesDocument3 pagesContrast NephRopathy GuidelinesStacey WoodsNo ratings yet
- Drug Information Center/KAUH: Selecting Gluten-Free Antibiotics in Celiac DiseaseDocument6 pagesDrug Information Center/KAUH: Selecting Gluten-Free Antibiotics in Celiac DiseaseStacey WoodsNo ratings yet
- C.a.U.S.E. - Cardiac Arrest Ultra-Sound Exam - A Better Approach To Managing Patients in Primary Non-Arrhythmogenic Cardiac ArrestDocument2 pagesC.a.U.S.E. - Cardiac Arrest Ultra-Sound Exam - A Better Approach To Managing Patients in Primary Non-Arrhythmogenic Cardiac ArrestStacey WoodsNo ratings yet
- Procoagulant GuidelineDocument30 pagesProcoagulant GuidelineStacey WoodsNo ratings yet
- Antimicrobials at The End of LifeDocument2 pagesAntimicrobials at The End of LifeStacey WoodsNo ratings yet
- Fluid Choices Impact Outcome in Septic ShockDocument7 pagesFluid Choices Impact Outcome in Septic ShockStacey WoodsNo ratings yet
- Elderly Patients Making Wise ChoicesDocument6 pagesElderly Patients Making Wise ChoicesStacey WoodsNo ratings yet
- Potasio. 2014.Document19 pagesPotasio. 2014.Nestor Enrique Aguilar SotoNo ratings yet
- Biomarkers of SepsisDocument8 pagesBiomarkers of SepsisStacey WoodsNo ratings yet
- StrokeDocument2 pagesStrokeStacey WoodsNo ratings yet
- Preoperative Insulin 2013Document3 pagesPreoperative Insulin 2013Stacey WoodsNo ratings yet
- Airway Clearance in The Intensive Care UnitDocument5 pagesAirway Clearance in The Intensive Care UnitStacey WoodsNo ratings yet
- The ABC of Weaning Failure - A Structured ApproachDocument9 pagesThe ABC of Weaning Failure - A Structured ApproachArul ShanmugamNo ratings yet
- Anna Gray's Psychiatric Assessment and TreatmentDocument10 pagesAnna Gray's Psychiatric Assessment and TreatmentsalfaciNo ratings yet
- Literature ReviewDocument5 pagesLiterature Reviewapi-559333867No ratings yet
- Interview QuestionsDocument5 pagesInterview QuestionsraprapNo ratings yet
- Mindfulness-Based Cognitive Therapy For DepressionDocument10 pagesMindfulness-Based Cognitive Therapy For DepressionCMValmaNo ratings yet
- Social Anxiety Disorder Treatment GuideDocument6 pagesSocial Anxiety Disorder Treatment GuidebrokentoeNo ratings yet
- Hair-Pulling Disorder (Trichotillomania)Document7 pagesHair-Pulling Disorder (Trichotillomania)Artlab CreativedesignNo ratings yet
- 117 NotesDocument17 pages117 NotesMARYISABEL �ERNINo ratings yet
- KNH 413 Sga Case StudyDocument11 pagesKNH 413 Sga Case Studyapi-301897220No ratings yet
- Abnormal Sexuality and Sexual DysfunctionsDocument8 pagesAbnormal Sexuality and Sexual DysfunctionsIsabel CastilloNo ratings yet
- Nikolas Rose - Neurochemical Selves - Society, Nov/Dec 2003Document14 pagesNikolas Rose - Neurochemical Selves - Society, Nov/Dec 2003kod65redNo ratings yet
- PsychologyDocument7 pagesPsychologyHarish KumarNo ratings yet
- Topics List - First AID 2019Document28 pagesTopics List - First AID 2019saraNo ratings yet
- What Is Serotonin SyndromeDocument4 pagesWhat Is Serotonin SyndromeBianca CaterinalisendraNo ratings yet
- MHN DRUGDocument2 pagesMHN DRUGWillington ShinyNo ratings yet
- Anxirty Disorders PDFDocument28 pagesAnxirty Disorders PDFZohaib TariqNo ratings yet
- Ford Ajg 2014 GuidelineDocument26 pagesFord Ajg 2014 GuidelineVinsensius Rubin Ferreri ArismarjiantoNo ratings yet
- Is Cardiovascular or Resistance Exercise Better To Treat Patients With Depression A Narrative ReviewDocument9 pagesIs Cardiovascular or Resistance Exercise Better To Treat Patients With Depression A Narrative ReviewjasonNo ratings yet
- The Efficacy of Psychodynamic Psychotherapy Jonathan Shedler PDFDocument12 pagesThe Efficacy of Psychodynamic Psychotherapy Jonathan Shedler PDFManuel PernetasNo ratings yet
- Psych 3.4 SsriDocument3 pagesPsych 3.4 SsriAlyanna Marie MirandaNo ratings yet
- Review of Literature on Social PhobiaDocument18 pagesReview of Literature on Social PhobiaMark San AndresNo ratings yet
- Lichen Simplex Chronicus - TreatmentDocument5 pagesLichen Simplex Chronicus - TreatmentclarissapamudjiNo ratings yet