You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Study Guide Medication AdministrationDocument13 pagesStudy Guide Medication Administrationmdrob89100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nursing Professional ResponsibilitiesDocument9 pagesNursing Professional ResponsibilitieslhenNo ratings yet
- Principles of Drug Therapy in Dentistry PDFDocument163 pagesPrinciples of Drug Therapy in Dentistry PDFJetter LeeNo ratings yet
- 2-E.BMR Liquid InjectionDocument28 pages2-E.BMR Liquid InjectionMohammed Zubair100% (7)
- Test Bank For Pharmacology A Patient Centered Nursing Process Approach 9th EditionDocument7 pagesTest Bank For Pharmacology A Patient Centered Nursing Process Approach 9th Editionjasonwrightjsfaxizewq100% (23)
- MedRad Stellant Operation ManualDocument98 pagesMedRad Stellant Operation ManualStanTofe67% (3)
- LiverDocument27 pagesLiverAndi Arwan AgusnawanNo ratings yet
- Management of Liver Trauma: Joint Hospital Surgical Grand Round 19 June 2004 United Christian HospitalDocument36 pagesManagement of Liver Trauma: Joint Hospital Surgical Grand Round 19 June 2004 United Christian HospitalAndi Arwan AgusnawanNo ratings yet
- HepaticDocument13 pagesHepaticAndi Arwan AgusnawanNo ratings yet
- Paliperidone Xeplion FINAL JUNE 2011 For WebsiteDocument8 pagesPaliperidone Xeplion FINAL JUNE 2011 For WebsiteAndi Arwan AgusnawanNo ratings yet
- Answer: Pulse Difficult To Palpate and East To Obliterate.: - Forwarded MessageDocument39 pagesAnswer: Pulse Difficult To Palpate and East To Obliterate.: - Forwarded MessagemarykristiroseNo ratings yet
- 10 1002@vms3 218Document17 pages10 1002@vms3 218Adriana PalmaNo ratings yet
- Administering Intradermal InjectionDocument17 pagesAdministering Intradermal InjectionPattNo ratings yet
- Doctor Brochure Stylage Bi Soft 2018Document36 pagesDoctor Brochure Stylage Bi Soft 2018薛凯No ratings yet
- MinimizingDocument5 pagesMinimizingAryananda Kondre AndikaNo ratings yet
- Local Anesthetics in Dentistry - Newer Methods of Delivery: Yen Lai Kee Second, Prasanna NeelakantanDocument3 pagesLocal Anesthetics in Dentistry - Newer Methods of Delivery: Yen Lai Kee Second, Prasanna NeelakantanEctopi CanineNo ratings yet
- Infectious DiseaseDocument2 pagesInfectious DiseasealyanadayritNo ratings yet
- Lecturenote - 245348428camel PPT-CH4-7Document146 pagesLecturenote - 245348428camel PPT-CH4-7haloNo ratings yet
- Microplanning: Achyut Shrestha, MDDocument110 pagesMicroplanning: Achyut Shrestha, MDMarchelleNo ratings yet
- FlexPen Generic Injection GuideDocument2 pagesFlexPen Generic Injection GuideIanNo ratings yet
- L2RLE eBOOKDocument80 pagesL2RLE eBOOKpatientsafetyNo ratings yet
- TensesDocument16 pagesTensesPanthers leoNo ratings yet
- A Prolonged Release Parenteral Drug Delivery SystemDocument11 pagesA Prolonged Release Parenteral Drug Delivery SystemronnymcmNo ratings yet
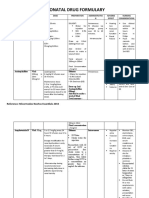
- Neonatal Drug FormularyDocument6 pagesNeonatal Drug FormularyLucian CaelumNo ratings yet
- Clikstar Dispositivo Administrador InsulinaDocument11 pagesClikstar Dispositivo Administrador InsulinaHenry SilvaNo ratings yet
- Vaccine Administration To Poultry FlocksDocument7 pagesVaccine Administration To Poultry FlocksNeeraj KashyapNo ratings yet
- Administering Intramuscular Injections To Children - What Does The Evidence Say?Document8 pagesAdministering Intramuscular Injections To Children - What Does The Evidence Say?ZACHARIAH MANKIRNo ratings yet
- Practice School Report On Indusrial TrainingDocument25 pagesPractice School Report On Indusrial Trainingabhishek .darshaNo ratings yet
- Velcade - HCP - Reconstitution Dosing Administration Booklet - v1 09 15Document8 pagesVelcade - HCP - Reconstitution Dosing Administration Booklet - v1 09 15hafiz iqbalNo ratings yet
- Equivalent To Caffeine 5mg/ml Equivalent To Caffeine 5mg/mlDocument2 pagesEquivalent To Caffeine 5mg/ml Equivalent To Caffeine 5mg/mlatawa1No ratings yet
- Calcium Gluconate1 PDFDocument18 pagesCalcium Gluconate1 PDFNatalia VoicilăNo ratings yet
- Needles Syringes Blood Collection Sharps Disposal Products CatalogDocument72 pagesNeedles Syringes Blood Collection Sharps Disposal Products Catalogmihalcea alinNo ratings yet
- Hepatitis A VaccineDocument5 pagesHepatitis A VaccineHåíthãm KhãtïßNo ratings yet
- Safe Injections - MCQDocument4 pagesSafe Injections - MCQSemo MezoNo ratings yet