You might also like
- Florida Codes 2020 PDFDocument172 pagesFlorida Codes 2020 PDFDiego Quiroga Cruz100% (1)
- Typical Medical Equip Heat GainDocument1 pageTypical Medical Equip Heat GainMostafa AlaahobaNo ratings yet
- CITY HVAC Design Guide AppendicesDocument41 pagesCITY HVAC Design Guide AppendicesSimon Law100% (1)
- Ahu DesignDocument17 pagesAhu DesignMohamed Aboobucker Mohamed IrfanNo ratings yet
- Ventilation - Electrical Rooms PDFDocument4 pagesVentilation - Electrical Rooms PDFvalentinlupascu33No ratings yet
- Drying: - Removal of Relatively Small Amount of Water or Organic Liquids - Final Processing Step Before PackagingDocument124 pagesDrying: - Removal of Relatively Small Amount of Water or Organic Liquids - Final Processing Step Before PackagingMiscrit Man100% (1)
- Preservation and Conservation For Libraries and ArchivesDocument236 pagesPreservation and Conservation For Libraries and ArchivesflunkedNo ratings yet
- Hvac in Hospitals (Ot)Document11 pagesHvac in Hospitals (Ot)anmol100% (1)
- Guide 1Document3 pagesGuide 1karimNo ratings yet
- Chiller Diversity FactorDocument3 pagesChiller Diversity FactoraadsamudNo ratings yet
- Above 500 Degrees C A PyrometerDocument6 pagesAbove 500 Degrees C A PyrometerCharlie Licup100% (2)
- Refrigeration and Airconditioning Hipolito B Sta MariaDocument106 pagesRefrigeration and Airconditioning Hipolito B Sta MariaMichael De Guzman0% (1)
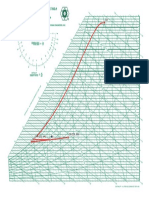
- Ashrae ChartDocument1 pageAshrae Chartalone160162lNo ratings yet
- ASHARE 36 Aee - April - 2021 - Ashrae - Guideline - 36Document42 pagesASHARE 36 Aee - April - 2021 - Ashrae - Guideline - 36Mike KennedyNo ratings yet
- HVAC Building Pressurization Systems: Lessons LearnedDocument45 pagesHVAC Building Pressurization Systems: Lessons Learnedmoh khNo ratings yet
- AHU Fresh AirDocument2 pagesAHU Fresh AirSvetla Nikolova100% (1)
- Saiver AHUDocument12 pagesSaiver AHUNorsyafiqah Rozi100% (1)
- ASHRAE - HVAC-HospitalBook - Room Design PDFDocument4 pagesASHRAE - HVAC-HospitalBook - Room Design PDFalialavi2No ratings yet
- Daikin VRV IV CatalogueDocument56 pagesDaikin VRV IV CatalogueMyo Kyaw KyawNo ratings yet
- Part E - 2 - (HVAC) Engineering DesignDocument69 pagesPart E - 2 - (HVAC) Engineering Designkeya2020No ratings yet
- Dedicated Outdoor Air Systems (Doas) : Indoor Air Quality + Energy Recovery + Humidity ControlDocument39 pagesDedicated Outdoor Air Systems (Doas) : Indoor Air Quality + Energy Recovery + Humidity Controlhtanh100% (1)
- Value Engineering of Car Park Ventilation SystemDocument8 pagesValue Engineering of Car Park Ventilation SystemmitasyahuNo ratings yet
- Ceiling DiffusersDocument21 pagesCeiling DiffusersMonal MuthusamyNo ratings yet
- Fcu PipingDocument20 pagesFcu PipingRamadan RashadNo ratings yet
- Division 23 - Heating, Ventilating and Air ConditioningDocument352 pagesDivision 23 - Heating, Ventilating and Air ConditioningCarl CrowNo ratings yet
- Designing HVAC System With and Without Heat Recovery Wheel Using ECO FRESH Enthalpy WheelDocument4 pagesDesigning HVAC System With and Without Heat Recovery Wheel Using ECO FRESH Enthalpy WheelZain ShariffNo ratings yet
- Carrierdes1 PDFDocument163 pagesCarrierdes1 PDFDomingo RuizNo ratings yet
- 1.1test MethodologyDocument14 pages1.1test MethodologyjvfcvNo ratings yet
- FireRated Ventilation Duct PresentationDocument25 pagesFireRated Ventilation Duct Presentationkenard291No ratings yet
- Comparison of ASHRAE 52.1 and 52.2 PDFDocument5 pagesComparison of ASHRAE 52.1 and 52.2 PDFChi Kit PhoonNo ratings yet
- Acoustic Calculation of Ventilation SystemsDocument49 pagesAcoustic Calculation of Ventilation SystemsHari Babu DharmavarapuNo ratings yet
- Calculate Exhaust Fan Size (1.1.19)Document6 pagesCalculate Exhaust Fan Size (1.1.19)mohammed imran pashaNo ratings yet
- ASHRAE Standard 62-2007Document26 pagesASHRAE Standard 62-2007schiZ0prEni100% (1)
- Heat Load Calculation ExampleDocument5 pagesHeat Load Calculation ExampleJoshua RanjithNo ratings yet
- IMI HB-1-Balancing of Control LoopsDocument48 pagesIMI HB-1-Balancing of Control LoopsAbey VettoorNo ratings yet
- Optimising Chillers and TowersDocument7 pagesOptimising Chillers and TowersAbhishek SauntokheeNo ratings yet
- HMDA Mechanical Services Data Book Medical Gas Systems 2021 Edition 1 Sources of SupplyDocument10 pagesHMDA Mechanical Services Data Book Medical Gas Systems 2021 Edition 1 Sources of SupplyeimrehNo ratings yet
- Ashrae Acgih Covid 19 White PaperDocument23 pagesAshrae Acgih Covid 19 White PaperBerk KÖTEŞLİNo ratings yet
- Building / Room Air Change RatesDocument11 pagesBuilding / Room Air Change Ratesசண்முக சுந்தரம் குருசாமிNo ratings yet
- Specifications For Fire Rated Gi Duct WorksDocument2 pagesSpecifications For Fire Rated Gi Duct Workspsn_kylmNo ratings yet
- Windows 1256''Plc ApplicationDocument56 pagesWindows 1256''Plc ApplicationAlaa Faiq0% (1)
- Im j1 Personnel Cooling Load Estimation 2014Document40 pagesIm j1 Personnel Cooling Load Estimation 2014Melvin SanchezNo ratings yet
- Commercial Kitchen Exhaust System - Fire Dept 2015Document39 pagesCommercial Kitchen Exhaust System - Fire Dept 2015joabjim8392No ratings yet
- SKM FCU High Static DetailDocument28 pagesSKM FCU High Static DetailInzamamNo ratings yet
- HVAC Design For Healthcare Facilities: Course No: M06-011 Credit: 6 PDHDocument60 pagesHVAC Design For Healthcare Facilities: Course No: M06-011 Credit: 6 PDHNelson VargasNo ratings yet
- Appendix A Ductwork 61294 - 29Document36 pagesAppendix A Ductwork 61294 - 29rastogishivendra100% (9)
- Hospital HVAC Design A Challenge For IAQ, Energy Recovery and System Reliability - Issue Jul-Sep 2002Document11 pagesHospital HVAC Design A Challenge For IAQ, Energy Recovery and System Reliability - Issue Jul-Sep 2002Go Tze FongNo ratings yet
- Ducts and Diffusers Design PDFDocument106 pagesDucts and Diffusers Design PDFsiroliver39No ratings yet
- Kitchen Ventilation Systems PDFDocument69 pagesKitchen Ventilation Systems PDFAzwan AwalludinNo ratings yet
- Hvac OtDocument4 pagesHvac OtshreyaNo ratings yet
- HVAC in Hospital PDFDocument7 pagesHVAC in Hospital PDFMohammed Toema100% (1)
- Flow Tech Louvers PDFDocument10 pagesFlow Tech Louvers PDFMoriyasuNguyenNo ratings yet
- AIA DHHS Ventilation Requirements For Areas Affecting Patient Care in HospitalsDocument4 pagesAIA DHHS Ventilation Requirements For Areas Affecting Patient Care in HospitalsMahipal Singh RaoNo ratings yet
- ANSI-ASHRAE-ASHE Standard 170-2008 FOR HOSPITALDocument4 pagesANSI-ASHRAE-ASHE Standard 170-2008 FOR HOSPITALPradeep SukumaranNo ratings yet
- Lecture 6 Zoning in HvacDocument32 pagesLecture 6 Zoning in HvacBhaskar BhatiaNo ratings yet
- Table 7.1 Design Parameters: ANSI/ASHRAE/ASHE Standard 170 - 2008Document6 pagesTable 7.1 Design Parameters: ANSI/ASHRAE/ASHE Standard 170 - 2008mkkNo ratings yet
- 78 Return Grille LocationsDocument2 pages78 Return Grille LocationsKyaw San OoNo ratings yet
- Ventilation Lecture 4 PH Alleen LezenDocument25 pagesVentilation Lecture 4 PH Alleen LezenNazimAhmedNo ratings yet
- AHU Catalogue enDocument68 pagesAHU Catalogue enTRISTIANDINDA PERMATANo ratings yet
- 2012 VAV Boxes Energy Efficiency, Air Leakage and ASHRAE 90.1Document29 pages2012 VAV Boxes Energy Efficiency, Air Leakage and ASHRAE 90.1din_thorpe3248No ratings yet
- Upvc Pipes and FittingsDocument40 pagesUpvc Pipes and Fittingshammad21No ratings yet
- Technical Booklet K 2012Document81 pagesTechnical Booklet K 2012Ali GurselNo ratings yet
- Domestic Hot Water Solutions Guide For HospitalsDocument8 pagesDomestic Hot Water Solutions Guide For HospitalsFarhang MotallebiNo ratings yet
- Ventilare Si Desfumare Parcaje - ModelDocument220 pagesVentilare Si Desfumare Parcaje - ModelalanatoraNo ratings yet
- EF303 - Climate Systems - AHU SystemDocument175 pagesEF303 - Climate Systems - AHU SystemAizat Faliq100% (2)
- Dasco Round & Jet DiffusersDocument28 pagesDasco Round & Jet Diffusersمحمد عماد100% (1)
- 8.6 2011 ASHRAE Handbook-HVAC ApplicationsDocument2 pages8.6 2011 ASHRAE Handbook-HVAC ApplicationsNiong DavidNo ratings yet
- CHAPTER 9 Room Ventilation SystemsDocument6 pagesCHAPTER 9 Room Ventilation SystemsJuan IntriagoNo ratings yet
- Design Criteria For Infrastructure Projects, Storm WaterDocument20 pagesDesign Criteria For Infrastructure Projects, Storm WaterAlaa FaiqNo ratings yet
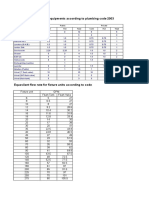
- Fixture Unit For Sanitary Equipments According To Plumbing Code 2003Document2 pagesFixture Unit For Sanitary Equipments According To Plumbing Code 2003Alaa FaiqNo ratings yet
- Chillers CatalogueDocument42 pagesChillers CatalogueAlaa FaiqNo ratings yet
- Lighting Power Densities - ASHREA Load Limit PDFDocument2 pagesLighting Power Densities - ASHREA Load Limit PDFAlaa FaiqNo ratings yet
- Tenant Design StandardsDocument1 pageTenant Design StandardsAlaa FaiqNo ratings yet
- Water SystemDocument1 pageWater SystemAlaa FaiqNo ratings yet
- Canadian Light Source Electrical Design Criteria - Aulakh - 8.1.16.1rev 0Document106 pagesCanadian Light Source Electrical Design Criteria - Aulakh - 8.1.16.1rev 0Alaa FaiqNo ratings yet
- BOQ - Residential Tower - Electrical - 21 JuneDocument194 pagesBOQ - Residential Tower - Electrical - 21 JuneAlaa FaiqNo ratings yet
- Conductor SizesDocument1 pageConductor SizesAlaa FaiqNo ratings yet
- Cable SizingDocument2 pagesCable SizingMohammed ThoufeeqNo ratings yet
- Calculation Formulas To Select Dehumidifiers at HTTPDocument2 pagesCalculation Formulas To Select Dehumidifiers at HTTPalone160162lNo ratings yet
- Starcool CI5Document223 pagesStarcool CI5Jonas Matheus Sardena PeresNo ratings yet
- Service Manual - Manual HVAC (HEATING, VENTILATION, AND AIR CONDITIONING)Document53 pagesService Manual - Manual HVAC (HEATING, VENTILATION, AND AIR CONDITIONING)Jairo MoralesNo ratings yet
- Sabiana Sabiana: Ceiling Air ConditioningDocument20 pagesSabiana Sabiana: Ceiling Air ConditioningkiradavidNo ratings yet
- Vaisala Industrial-Product-Catalog-low PDFDocument224 pagesVaisala Industrial-Product-Catalog-low PDFJose GarciaNo ratings yet
- NR 12 Solar ShadingDocument52 pagesNR 12 Solar ShadingStrumfetaPipetaNo ratings yet
- FPLRN 268Document14 pagesFPLRN 268tonyNo ratings yet
- The Applications of Heat Exchangers Refrigeration SystemsDocument38 pagesThe Applications of Heat Exchangers Refrigeration SystemsBasem RajabNo ratings yet
- Lab Report: Refrigeration SystemDocument5 pagesLab Report: Refrigeration SystemFarhan AizatNo ratings yet
- MODULE 1 Conduction Through Plane Wall & Composite Plane WallsDocument5 pagesMODULE 1 Conduction Through Plane Wall & Composite Plane WallsFamela GadNo ratings yet
- Lutron Me-9000 PDFDocument2 pagesLutron Me-9000 PDFPravin & Co. Pravin shahNo ratings yet
- Humidification / Dehumidification SystemDocument4 pagesHumidification / Dehumidification SystemMatias RolonNo ratings yet
- WWW Belart Com Bel Art h42070 1400 Secador Digital HygrometeDocument2 pagesWWW Belart Com Bel Art h42070 1400 Secador Digital HygrometecarbouNo ratings yet
- Tugas Termodinamika 1 - Siti Choirunisa Furi K - 5213416033Document3 pagesTugas Termodinamika 1 - Siti Choirunisa Furi K - 5213416033siti choirunisa furi kurnitaNo ratings yet
- Module 2 NotesDocument17 pagesModule 2 NotesKajalNo ratings yet
- Calibrating A Thermometer: To Calibrate A Thermometer, The Ice Point of Water Is Usually Taken To BeDocument4 pagesCalibrating A Thermometer: To Calibrate A Thermometer, The Ice Point of Water Is Usually Taken To BeMuhammad UbaidNo ratings yet
- 2016-09-25 Refrigeration Engineering Syllabus PDFDocument5 pages2016-09-25 Refrigeration Engineering Syllabus PDFTy PhanNo ratings yet
- HVAC Design Cooling Capacity Calculations & Psychrometrics 29 Feb To 1 March 2016 PDFDocument3 pagesHVAC Design Cooling Capacity Calculations & Psychrometrics 29 Feb To 1 March 2016 PDFKoo Cheng KongNo ratings yet
- PP2 - Advance HVAC Course OEA - 1Document49 pagesPP2 - Advance HVAC Course OEA - 1Bassel El Sayed AliNo ratings yet
- Product Data: 38AUQ07 - 12 Heat Pump Outdoor Unit Split System With Puronr Refrigerant 60 HZDocument24 pagesProduct Data: 38AUQ07 - 12 Heat Pump Outdoor Unit Split System With Puronr Refrigerant 60 HZMarco Antonio Camacho Tezanos-PintoNo ratings yet
- AirCon Final Project 6BDocument85 pagesAirCon Final Project 6BArielle Jean BarcenasNo ratings yet
- Iiiii: by Lewis G. Harriman III, Member ASHRAE, and James Judge, P.E., Member ASHRAEDocument6 pagesIiiii: by Lewis G. Harriman III, Member ASHRAE, and James Judge, P.E., Member ASHRAERafael Echano AcederaNo ratings yet
- STULZ CompactPlus DX Brochure 1211 enDocument4 pagesSTULZ CompactPlus DX Brochure 1211 enCristian EncinaNo ratings yet