You might also like
- Treatment Planning Single Maxillary Anterior Implants for DentistsFrom EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNo ratings yet
- Orthodontics andDocument9 pagesOrthodontics andSimona DobreNo ratings yet
- Minimally Invasive Esthetic Therapy A CaseDocument8 pagesMinimally Invasive Esthetic Therapy A CaseMarco VázquezNo ratings yet
- CirugiaDocument27 pagesCirugiaalexmtzgNo ratings yet
- Factores Macroesteticos en El Diseño de SonrisaDocument7 pagesFactores Macroesteticos en El Diseño de SonrisaJassel DurdenNo ratings yet
- JCDA Simon RosenblattDocument8 pagesJCDA Simon RosenblattZiv SimonNo ratings yet
- Lyu 2018Document7 pagesLyu 2018Andres CoboNo ratings yet
- Orthodontic Treatment in A Periodontal Patient With Pathologic Migration of Anterior TeethDocument9 pagesOrthodontic Treatment in A Periodontal Patient With Pathologic Migration of Anterior TeethMárcio LMSNo ratings yet
- Asds 02 0215Document3 pagesAsds 02 02156mf9jf6h99No ratings yet
- Black TriangleDocument9 pagesBlack TriangleYasser MagramiNo ratings yet
- Fixed Partial Dentures: Diagnosis and Treatment Planning For Fixed ProsthodonticsDocument6 pagesFixed Partial Dentures: Diagnosis and Treatment Planning For Fixed ProsthodonticspalliNo ratings yet
- Orthodontically Assisted Restorative Dentistry: Donald F. Reikie, DDS, MSDocument5 pagesOrthodontically Assisted Restorative Dentistry: Donald F. Reikie, DDS, MSAdityaNo ratings yet
- Pucciarelli2018 PDFDocument4 pagesPucciarelli2018 PDFAkanksha MahajanNo ratings yet
- 1 s2.0 S001185321100005X MainDocument17 pages1 s2.0 S001185321100005X MainMohammed OmoshNo ratings yet
- Mi Sympheal DODocument10 pagesMi Sympheal DOChhavi SinghalNo ratings yet
- Multidisciplinary Approach to Esthetic DentistryDocument19 pagesMultidisciplinary Approach to Esthetic DentistryAya Ibrahim Yassin100% (1)
- Integrating Dental Procedures to Improve Occlusal RehabilitationDocument18 pagesIntegrating Dental Procedures to Improve Occlusal RehabilitationgabrielaNo ratings yet
- Design of FPDDocument2 pagesDesign of FPDSorabh JainNo ratings yet
- Transverse Dimension Andlong-Term Stability Robert L Vanarsdall JRDocument10 pagesTransverse Dimension Andlong-Term Stability Robert L Vanarsdall JRMa Lyn GabayeronNo ratings yet
- PERIODONTAL CONSIDERATIONS IN FIXED PROSTHESESDocument5 pagesPERIODONTAL CONSIDERATIONS IN FIXED PROSTHESESWidhi Satrio NugrohoNo ratings yet
- Third Molar Autotransplant Planning With A Tooth Replica. A Year of Follow-Up Case ReportDocument6 pagesThird Molar Autotransplant Planning With A Tooth Replica. A Year of Follow-Up Case ReportAlNo ratings yet
- The Orthodontist's Role in 21st Century Periodontic-Prosthodontic TherapyDocument19 pagesThe Orthodontist's Role in 21st Century Periodontic-Prosthodontic TherapyAna Maria Montoya GomezNo ratings yet
- Primary Teeth ThesisDocument4 pagesPrimary Teeth Thesisgbvc57fd100% (2)
- Periodontal Treatment of Excessive Gingival DisplayDocument12 pagesPeriodontal Treatment of Excessive Gingival DisplayJuan Carlos CárcamoNo ratings yet
- The Single-Tooth Dental Implant: Practical Guidelines For Hard Tissue AugmentationDocument16 pagesThe Single-Tooth Dental Implant: Practical Guidelines For Hard Tissue Augmentation歐亦焜100% (1)
- Dentalcrowding:The Restorativeapproach: Luis Brea,, Anabella Oquendo,, Steven DavidDocument10 pagesDentalcrowding:The Restorativeapproach: Luis Brea,, Anabella Oquendo,, Steven DavidFRISKA E PANJAITANNo ratings yet
- Jced 13 E75Document6 pagesJced 13 E75Ezza RezzaNo ratings yet
- The Aesthetic Smile: Diagnosis Treatment: Garber SalamaDocument11 pagesThe Aesthetic Smile: Diagnosis Treatment: Garber SalamaAdriana RibeiroNo ratings yet
- Original Articles: Rationale and Methods For Crown LengtheningDocument4 pagesOriginal Articles: Rationale and Methods For Crown LengtheningAna CernaianuNo ratings yet
- Guia Anterior - Gonzalez Hernandez-61-2Document12 pagesGuia Anterior - Gonzalez Hernandez-61-2Fred TorresNo ratings yet
- 7.principles of Dentofacial Orthopedics PDFDocument10 pages7.principles of Dentofacial Orthopedics PDFMafer VazquezNo ratings yet
- 3 Badr2016Document22 pages3 Badr2016Daniel Espinoza EspinozaNo ratings yet
- Alternativas A TotalesDocument12 pagesAlternativas A TotalesJuan Jose Stuven RodriguezNo ratings yet
- Root Resorption A 6-Year Follow-Up Case ReportDocument3 pagesRoot Resorption A 6-Year Follow-Up Case Reportpaola lopezNo ratings yet
- Combined Orthodontic - .Vdphjohjwbm5Sfbunfoupgb Q 1ptupsuipepoujd (Johjwbm3FdfttjpoDocument16 pagesCombined Orthodontic - .Vdphjohjwbm5Sfbunfoupgb Q 1ptupsuipepoujd (Johjwbm3FdfttjpobetziiNo ratings yet
- Diagnosis and Treatment Planning in Fixed Partial Dentures / Orthodontic Courses by Indian Dental AcademyDocument34 pagesDiagnosis and Treatment Planning in Fixed Partial Dentures / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Orthognathic Surgery For Patients With Maxillofacial DeformitiesDocument25 pagesOrthognathic Surgery For Patients With Maxillofacial DeformitiesahmedatefNo ratings yet
- Gingival Recession Related To Removable Partial Dentures in Older PatientsDocument6 pagesGingival Recession Related To Removable Partial Dentures in Older Patientssara luciaNo ratings yet
- Missing Lateral Incisors Treatment ApproachesDocument17 pagesMissing Lateral Incisors Treatment ApproachesAvneet MalikNo ratings yet
- Zachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationDocument5 pagesZachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationplsssssNo ratings yet
- Predict Root Coverage OutcomesDocument8 pagesPredict Root Coverage OutcomesEvan BlackwellNo ratings yet
- Wal Drop 2008Document12 pagesWal Drop 2008César RodríguezNo ratings yet
- Soft Tissue Enhancement Around Dental ImplantDocument20 pagesSoft Tissue Enhancement Around Dental ImplantWang KaiminNo ratings yet
- Crown Lengthening Techniques and IndicationsDocument5 pagesCrown Lengthening Techniques and IndicationsAnil NepalNo ratings yet
- Section 051 Restorative ContoursDocument20 pagesSection 051 Restorative ContoursirfanahmedshaikhNo ratings yet
- Ke Principles of Implant Dentistr in The Esthetic Zone: Michael Sonick, DMD Debb Hwang, DMDDocument6 pagesKe Principles of Implant Dentistr in The Esthetic Zone: Michael Sonick, DMD Debb Hwang, DMDVikas Aggarwal100% (1)
- The Single-Tooth RestorationDocument5 pagesThe Single-Tooth Restorationumerjaved86No ratings yet
- 2006 - Zuchelli - Predetermine The Line of Root Coverage PDFDocument8 pages2006 - Zuchelli - Predetermine The Line of Root Coverage PDFAntonio González RuizNo ratings yet
- Anterior Esthetic Crown-Lengthening Surgery: A Case ReportDocument4 pagesAnterior Esthetic Crown-Lengthening Surgery: A Case ReportSNo ratings yet
- Lyons Et Al-2017-Periodontology 2000Document4 pagesLyons Et Al-2017-Periodontology 2000Julio César PlataNo ratings yet
- Bilateral Fusion of Mandibular Second Molars With Supernumerary Teeth: Case ReportDocument5 pagesBilateral Fusion of Mandibular Second Molars With Supernumerary Teeth: Case ReportUcc Ang BangarenNo ratings yet
- Redictable and Precise Tooth Preparation Techniques For Porcelain Laminate Veneers in Complex CasesDocument7 pagesRedictable and Precise Tooth Preparation Techniques For Porcelain Laminate Veneers in Complex CasesnobelcyrilNo ratings yet
- Non Familiar Characterization Using A Loop Connection in A Fixed Partial DentureDocument3 pagesNon Familiar Characterization Using A Loop Connection in A Fixed Partial DentureAzzam SaqrNo ratings yet
- Management of Perio Prostho Situations in DentistryDocument18 pagesManagement of Perio Prostho Situations in DentistryHarsha ReddyNo ratings yet
- chin implantDocument6 pageschin implantAnkita GuravNo ratings yet
- The Fate of The Distal Papilla Around Tooth-Bound Implant-Supported Restorations in Maxillary Central Incisor SitesDocument7 pagesThe Fate of The Distal Papilla Around Tooth-Bound Implant-Supported Restorations in Maxillary Central Incisor SitesValentinaNo ratings yet
- Step-By-Step Instructions On The: Straumann TibrushDocument4 pagesStep-By-Step Instructions On The: Straumann Tibrushadambear213No ratings yet
- JadaDocument14 pagesJadaadambear213No ratings yet
- CDC - Half of American Adults Have Periodontal Disease - PerioDocument3 pagesCDC - Half of American Adults Have Periodontal Disease - Perioadambear213No ratings yet
- Greenstein Et Tarnow 2006ddDocument11 pagesGreenstein Et Tarnow 2006ddAnup Lal RajbahakNo ratings yet
- Keratinized Mucosa Around Dental ImplantsDocument2 pagesKeratinized Mucosa Around Dental Implantsadambear213No ratings yet
- Dental Office Marketing PlanDocument20 pagesDental Office Marketing PlanPalo Alto Software100% (10)
- Jop 1974 45 3 151Document4 pagesJop 1974 45 3 151adambear213No ratings yet
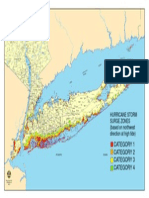
- Nys Storm Surge ZonesDocument1 pageNys Storm Surge Zonesadambear213No ratings yet
- Malpractice and Perio DiseaseDocument4 pagesMalpractice and Perio Diseaseadambear213No ratings yet
- Sterile Healing Solutions FOFDocument2 pagesSterile Healing Solutions FOFadambear213No ratings yet
- 3-Evaluation of Human Recession Defects Treated With Coronally Advanced Flaps and Either Enamel Matrix Derivatives or Connective Tissue - Comparison of Clinical Parameters at 10Document10 pages3-Evaluation of Human Recession Defects Treated With Coronally Advanced Flaps and Either Enamel Matrix Derivatives or Connective Tissue - Comparison of Clinical Parameters at 10adambear213No ratings yet
- 27Document7 pages27adambear213No ratings yet
- TISPDocument14 pagesTISPadambear213100% (1)
- Ideas Academy Reports: and InnovationsDocument9 pagesIdeas Academy Reports: and Innovationsadambear213No ratings yet
- J 1600-0757 1997 tb00094 XDocument21 pagesJ 1600-0757 1997 tb00094 Xadambear213No ratings yet
- Average Tooth MeasurmentsDocument1 pageAverage Tooth Measurmentsadambear213No ratings yet
- ArticleDocument7 pagesArticleadambear213No ratings yet
- REVISED ASSIGNMENTS Biology and Pathology of The PeriodontiumDocument2 pagesREVISED ASSIGNMENTS Biology and Pathology of The Periodontiumadambear213No ratings yet
- 16Document9 pages16adambear213No ratings yet
- WhatsNew E OldDocument25 pagesWhatsNew E Oldadambear213No ratings yet
- WhatsNew EDocument37 pagesWhatsNew Eadambear213No ratings yet
- Suture Surg Gut Chrom Bge FS2 4Document1 pageSuture Surg Gut Chrom Bge FS2 4adambear213No ratings yet
- Map ArenaDocument1 pageMap Arenaadambear213No ratings yet
- IBR Application CDocument12 pagesIBR Application CChris HudginsNo ratings yet
- Sterile Healing Solutions FOFDocument2 pagesSterile Healing Solutions FOFadambear213No ratings yet
- Family MedicineDocument156 pagesFamily MedicinedtriggNo ratings yet
- FinalsDocument8 pagesFinalsDumpNo ratings yet
- Block 1 Board Review - Lecture NotesDocument127 pagesBlock 1 Board Review - Lecture NotesCece RereNo ratings yet
- Theories of Motivation and Child Moral DevelopmentDocument5 pagesTheories of Motivation and Child Moral DevelopmentPamela mirandaNo ratings yet
- Right To HealthDocument9 pagesRight To HealthPriya SharmaNo ratings yet
- Puskesmas Dua Puluh Tiga Ilir Publishes Vaccination Ticket ListDocument98 pagesPuskesmas Dua Puluh Tiga Ilir Publishes Vaccination Ticket ListLaboratorium PKM 23 IlirNo ratings yet
- Synthesis, Experimental and Theoretical Characterizations of A NewDocument7 pagesSynthesis, Experimental and Theoretical Characterizations of A NewWail MadridNo ratings yet
- Wastewater Treatment Plant Design PDFDocument68 pagesWastewater Treatment Plant Design PDFmostafa1alaahobaNo ratings yet
- Material Safety Data Sheet: WWW - Smartlab.co - IdDocument8 pagesMaterial Safety Data Sheet: WWW - Smartlab.co - Idlalan suparlanNo ratings yet
- VIDEO 2 - Thì hiện tại tiếp diễn và hiện tại hoàn thànhDocument3 pagesVIDEO 2 - Thì hiện tại tiếp diễn và hiện tại hoàn thànhÝ Nguyễn NhưNo ratings yet
- Alok ResumeDocument3 pagesAlok Resumealok choudharyNo ratings yet
- 01 - 01 - SK10 - JXNipponDocument1 page01 - 01 - SK10 - JXNipponredevils86No ratings yet
- SCE Research Paper PDFDocument12 pagesSCE Research Paper PDFmuoi2002No ratings yet
- Gate Installation ReportDocument3 pagesGate Installation ReportKumar AbhishekNo ratings yet
- 1 Colmac DX Ammonia Piping Handbook 4th EdDocument64 pages1 Colmac DX Ammonia Piping Handbook 4th EdAlbertoNo ratings yet
- Aplikasi Berbagai Jenis Media Dan ZPT Terhadap Aklimatisasi Anggrek VandaDocument15 pagesAplikasi Berbagai Jenis Media Dan ZPT Terhadap Aklimatisasi Anggrek VandaSihonoNo ratings yet
- Biology (Paper I)Document6 pagesBiology (Paper I)AH 78No ratings yet
- ABSCESSDocument35 pagesABSCESSlax prajapatiNo ratings yet
- 9 To 5 Props PresetsDocument4 pages9 To 5 Props Presetsapi-300450266100% (1)
- Q4 Module 8Document14 pagesQ4 Module 8DerickNo ratings yet
- 3 Types of Chemical BondsDocument12 pages3 Types of Chemical BondsSaediRisquéBriskeyNo ratings yet
- Micdak BackgroundDocument3 pagesMicdak Backgroundappiah ernestNo ratings yet
- Steam System Design RequirementsDocument29 pagesSteam System Design RequirementsAthirahNo ratings yet
- RHS NCRPO COVID FormDocument1 pageRHS NCRPO COVID Formspd pgsNo ratings yet
- Parasitology Lecture Hosts, Symbiosis & TransmissionDocument10 pagesParasitology Lecture Hosts, Symbiosis & TransmissionPatricia Ann JoseNo ratings yet
- Benefits and Limitations of Vojta ApproachDocument50 pagesBenefits and Limitations of Vojta ApproachAlice Teodorescu100% (3)
- Hypertension Protocol Mukta VatiDocument18 pagesHypertension Protocol Mukta VatiDr. Avnish UpadhyayNo ratings yet
- Insurance Principles, Types and Industry in IndiaDocument10 pagesInsurance Principles, Types and Industry in IndiaAroop PalNo ratings yet
- Assessment Formal AssessmentDocument7 pagesAssessment Formal Assessmentashish33% (3)
- Position paper-MUNUCCLE 2022: Refugees) Des États !Document2 pagesPosition paper-MUNUCCLE 2022: Refugees) Des États !matNo ratings yet