You might also like
- Intentional Replantation Techniques: A Critical ReviewDocument8 pagesIntentional Replantation Techniques: A Critical Reviewitsme543210100% (1)
- The Impact of Sealer Extrusion On Endodontic Outcome: A Systematic Review With Meta-AnalysisDocument7 pagesThe Impact of Sealer Extrusion On Endodontic Outcome: A Systematic Review With Meta-Analysisitsme543210No ratings yet
- Dentalcements1 151002150529 Lva1 App6891Document80 pagesDentalcements1 151002150529 Lva1 App6891itsme543210No ratings yet
- Hemisection As A Conservative Management of Grossly Carious Permanent Mandibular First MolarDocument3 pagesHemisection As A Conservative Management of Grossly Carious Permanent Mandibular First Molaritsme543210No ratings yet
- CastingDocument75 pagesCastingitsme543210No ratings yet
- Failures and ManagementDocument25 pagesFailures and Managementitsme5432100% (1)
- Failures of RestorationsDocument43 pagesFailures of Restorationsitsme543210100% (2)
- NecrosisDocument3 pagesNecrosisitsme543210No ratings yet
- Endodontic InstrumentsDocument63 pagesEndodontic Instrumentsitsme543210100% (1)
- Course DescriptionDocument8 pagesCourse Descriptionitsme543210No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- MlistDocument13 pagesMlistSumanth MopideviNo ratings yet
- Komunikasi Antar SelDocument39 pagesKomunikasi Antar SelMOCHILNo ratings yet
- 9700 - s21 - QP - 43 Worked SolutionDocument24 pages9700 - s21 - QP - 43 Worked SolutionAvocadoNo ratings yet
- Morphology and Physiology of BacteriaDocument9 pagesMorphology and Physiology of Bacteriaprashantshukla8280No ratings yet
- Food Chain and Food Web PDFDocument6 pagesFood Chain and Food Web PDFA. ZNo ratings yet
- Biochemistry CO PoisoningDocument19 pagesBiochemistry CO PoisoningHann SantiagoNo ratings yet
- IJED Lobo Scopin Barbosa HirataDocument14 pagesIJED Lobo Scopin Barbosa HirataCatia Sofia A PNo ratings yet
- PubMed Links 20171119Document2 pagesPubMed Links 20171119Scott BermanNo ratings yet
- 14 - Interferences in Immunoassay PDFDocument16 pages14 - Interferences in Immunoassay PDFLyannYisellNo ratings yet
- Isopod BehaviorDocument4 pagesIsopod BehaviorCody Griffin100% (1)
- Photos Courtesy of David Jubineau: Lip DetailDocument2 pagesPhotos Courtesy of David Jubineau: Lip DetailMedel SantillanNo ratings yet
- Casuarina Equisetifolia: Casuarinaceae LDocument7 pagesCasuarina Equisetifolia: Casuarinaceae LsherenraditaNo ratings yet
- NitroglycerinDocument6 pagesNitroglycerinPapaindoNo ratings yet
- Histology of The Circulatory SystemDocument24 pagesHistology of The Circulatory SystemFatima Zehra YusefNo ratings yet
- M1 Introduction To Anatomy and PhysiologyDocument4 pagesM1 Introduction To Anatomy and PhysiologyMeteor 858No ratings yet
- ddddddddddddddddddddddddddddddddDocument9 pagesddddddddddddddddddddddddddddddddjoao victorNo ratings yet
- Literature Please Refer To Included For Correct: Principles & Practice of Diffusion & OsmosisDocument30 pagesLiterature Please Refer To Included For Correct: Principles & Practice of Diffusion & OsmosisrezamaulanaNo ratings yet
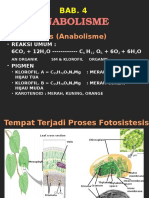
- Bab.4. AnabolismeDocument14 pagesBab.4. AnabolismeSurniSajaNo ratings yet
- Diploma Course in Hearing, Language and Speech (DHLS)Document23 pagesDiploma Course in Hearing, Language and Speech (DHLS)sudhirpratapsinghratNo ratings yet
- Glasgow Theses Service Theses@gla - Ac.ukDocument94 pagesGlasgow Theses Service Theses@gla - Ac.ukKrupali JainNo ratings yet
- Serial Dilution MethodDocument3 pagesSerial Dilution Methoddraneesh75% (4)
- Dengue PPT YaarDocument21 pagesDengue PPT YaarY ShouryaNo ratings yet
- Ultimate Guide To Nootropics - Part 2 - Racetams - The Original Nootropic Family - Nootropics DepotDocument17 pagesUltimate Guide To Nootropics - Part 2 - Racetams - The Original Nootropic Family - Nootropics Depotdgffg456100% (1)
- Cryptid CluebooksDocument20 pagesCryptid CluebooksMaría VélezNo ratings yet
- Biocomputers: Biochemical ComputersDocument3 pagesBiocomputers: Biochemical ComputersAjinkyaJadNo ratings yet
- Charles Darwin Web Quest AnswersDocument3 pagesCharles Darwin Web Quest AnswersKeyshawnNo ratings yet
- Monday 6 May 2019: BiologyDocument16 pagesMonday 6 May 2019: BiologynicaNo ratings yet
- General Biology - Q2 - Week 3Document19 pagesGeneral Biology - Q2 - Week 3Renard JaenNo ratings yet
- Odyssey High School Biology VocabularyDocument24 pagesOdyssey High School Biology VocabularyHanQian WangNo ratings yet
- 19 - 2010 Elevação Do Nível de Consciência em Guandu - Uma Perspectiva GlobalDocument542 pages19 - 2010 Elevação Do Nível de Consciência em Guandu - Uma Perspectiva GlobaldenissatoNo ratings yet