You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Effect of Exercise On Blood Pressure Control in HypertensiveDocument6 pagesEffect of Exercise On Blood Pressure Control in HypertensiveAliyah Adek RahmahNo ratings yet
- Exercise and Weight Loss Reduce Blood Pressure in Men and Women With Mild HypertensionDocument12 pagesExercise and Weight Loss Reduce Blood Pressure in Men and Women With Mild HypertensionAliyah Adek RahmahNo ratings yet
- Bates-Jensen Wound Assessment Tool (BWAT)Document4 pagesBates-Jensen Wound Assessment Tool (BWAT)Jamie OngNo ratings yet
- CFMHN Standards 1Document19 pagesCFMHN Standards 1Aliyah Adek RahmahNo ratings yet
- Dash AdekDocument8 pagesDash AdekAliyah Adek RahmahNo ratings yet
- Bars - DLDocument12 pagesBars - DLSimone BandrawalaNo ratings yet
- Bars - DLDocument12 pagesBars - DLSimone BandrawalaNo ratings yet
- Komunikasi 3BDocument31 pagesKomunikasi 3BAliyah Adek RahmahNo ratings yet
- Circulation 2002 Corti 2935 40Document7 pagesCirculation 2002 Corti 2935 40Aliyah Adek RahmahNo ratings yet
- Circulation 1994 Washington 2166 79Document15 pagesCirculation 1994 Washington 2166 79Aliyah Adek RahmahNo ratings yet
- Qigong For Hypertension A Systematic Review.19Document14 pagesQigong For Hypertension A Systematic Review.19Aliyah Adek RahmahNo ratings yet
- Chronic IllnessDocument3 pagesChronic IllnessAliyah Adek RahmahNo ratings yet
- Circulation 2010 Pladevall 1183 91Document23 pagesCirculation 2010 Pladevall 1183 91Aliyah Adek RahmahNo ratings yet
- Circulation 1994 Washington 2166 79Document15 pagesCirculation 1994 Washington 2166 79Aliyah Adek RahmahNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pendlay 5x5 Strength Program for BeginnersDocument2 pagesPendlay 5x5 Strength Program for BeginnersGuiye MarisiNo ratings yet
- Male Hypogonadism: Approval Number: G.MKT - GM.MH.04.2018.0513Document19 pagesMale Hypogonadism: Approval Number: G.MKT - GM.MH.04.2018.0513Billi Siddiqui100% (1)
- The Barbell Prescription PDFDocument376 pagesThe Barbell Prescription PDFRINNA100% (2)
- Nutrition for the Community Exam QuestionsDocument6 pagesNutrition for the Community Exam QuestionsRamBabuMeenaNo ratings yet
- Deurenberg Formula Imc para %grasaDocument10 pagesDeurenberg Formula Imc para %grasaAna Cecilia VegaNo ratings yet
- Zhuang, 2019 Differential Anti-Adipogenic Effects of EPA and DHA in ObesityDocument11 pagesZhuang, 2019 Differential Anti-Adipogenic Effects of EPA and DHA in ObesityDaniela Patricia Alvarez AravenaNo ratings yet
- Full-Sentence Speech FinalDocument2 pagesFull-Sentence Speech Finalapi-363883917No ratings yet
- Intervention Module - For NutritionDocument13 pagesIntervention Module - For NutritionRadhaKrishna BallaNo ratings yet
- Eating Disorders (All)Document11 pagesEating Disorders (All)Quỳnh LùnNo ratings yet
- Diene-O-Lean: Positioning Statement Who Should Use This Product?Document2 pagesDiene-O-Lean: Positioning Statement Who Should Use This Product?Nannda SuccindaaNo ratings yet
- Factors Affecting Wound HealingDocument11 pagesFactors Affecting Wound HealingFredy Rodeardo MaringgaNo ratings yet
- Respiratory MedicationsDocument18 pagesRespiratory Medicationsapi-338095748No ratings yet
- Food, Cooking Skills, and Health: A Literature Review: ArticleDocument7 pagesFood, Cooking Skills, and Health: A Literature Review: ArticleBarnali DuttaNo ratings yet
- Health, Fitness, and Wellness Goals for 2010Document20 pagesHealth, Fitness, and Wellness Goals for 2010Dusan Profesor JovanovicNo ratings yet
- Insanity - Dig Deeper!: Week 1 2-Jan 1-Jan 31-DecDocument5 pagesInsanity - Dig Deeper!: Week 1 2-Jan 1-Jan 31-DecErick Venegas HerreraNo ratings yet
- Body Image and Mental Health: GlossaryDocument6 pagesBody Image and Mental Health: GlossarySalsa Dwi PutriNo ratings yet
- Low-Fat Diet SheetDocument4 pagesLow-Fat Diet SheetPortableCreator100% (1)
- Sneaky Hacks That Boost MetabolismDocument11 pagesSneaky Hacks That Boost MetabolismLois JNo ratings yet
- Belly Fat Burning PDFDocument3 pagesBelly Fat Burning PDFSunny BiswalNo ratings yet
- Nbme 13Document11 pagesNbme 13ChadCowgill100% (1)
- PE Lesson on Fitness AssessmentsDocument25 pagesPE Lesson on Fitness AssessmentsRiz Monterola100% (5)
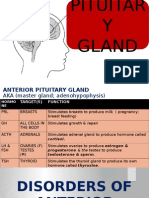
- Disorders of Pituitary GlandDocument34 pagesDisorders of Pituitary GlandninaaltheaNo ratings yet
- Descriptive Statistics Tasks SolvedDocument38 pagesDescriptive Statistics Tasks Solved0p00No ratings yet
- Diabetes ElektifDocument7 pagesDiabetes ElektifSiti SofiaNo ratings yet
- Notre Dame of Tacurong College Nursing Lesson Guide on Dietary ComputationsDocument11 pagesNotre Dame of Tacurong College Nursing Lesson Guide on Dietary ComputationsSehun OohNo ratings yet
- The Control of Partitioning Between Protein and FaDocument19 pagesThe Control of Partitioning Between Protein and FaChoi Joon-HyunNo ratings yet
- Fracora Placenta 5000 InstructionsDocument9 pagesFracora Placenta 5000 InstructionsKishin Dōji ZenkiNo ratings yet
- 10pounds MusclePlanDocument41 pages10pounds MusclePlanMahadiMohdDin100% (1)
- Screening Nutrition Care ProcessDocument70 pagesScreening Nutrition Care ProcessSiwonniekyubum DijaNo ratings yet
- Assessment and Management of Patients With Vascular Disorders and Problems of Peripheral CirculationDocument45 pagesAssessment and Management of Patients With Vascular Disorders and Problems of Peripheral CirculationCarlos RiosNo ratings yet