You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2019 A Smoking Prevention Program Delivered by Medical Students To Secondary Schools in Brazil Called EAT Randomized Controlled TrialDocument12 pages2019 A Smoking Prevention Program Delivered by Medical Students To Secondary Schools in Brazil Called EAT Randomized Controlled TrialpcrpcNo ratings yet
- An Old Risk Factor For COPD: Rest in Peace, 15%: Paulo César Rodrigues Pinto CorrêaDocument2 pagesAn Old Risk Factor For COPD: Rest in Peace, 15%: Paulo César Rodrigues Pinto CorrêapcrpcNo ratings yet
- An Old Risk Factor For COPD: Rest in Peace, 15%: Paulo César Rodrigues Pinto CorrêaDocument2 pagesAn Old Risk Factor For COPD: Rest in Peace, 15%: Paulo César Rodrigues Pinto CorrêapcrpcNo ratings yet
- AMEP 66627 Experience Based Redesign of A Collaborative and Distance Le 040115Document9 pagesAMEP 66627 Experience Based Redesign of A Collaborative and Distance Le 040115pcrpcNo ratings yet
- Reading Fluency - The Road To DevelopingDocument8 pagesReading Fluency - The Road To DevelopingRobison PoreliNo ratings yet
- Ged 105 - Main Topic 1Document33 pagesGed 105 - Main Topic 1Dannica Keyence MagnayeNo ratings yet
- VSTEP Writing: Effects of TourismDocument7 pagesVSTEP Writing: Effects of Tourismtran diemNo ratings yet
- Read The Following Passage and Mark The Letter A, B, C, or D To Indicate The Correct Answer To Each of The QuestionsDocument7 pagesRead The Following Passage and Mark The Letter A, B, C, or D To Indicate The Correct Answer To Each of The QuestionsHồng NhungNo ratings yet
- Emerys IepDocument15 pagesEmerys Iepapi-300745138No ratings yet
- Impact of Brand Experience On Customer Experience A Business To Consumer FocusDocument8 pagesImpact of Brand Experience On Customer Experience A Business To Consumer Focusshiphatun noorNo ratings yet
- IDO Invitation LetterDocument1 pageIDO Invitation LetterthepoliceisafteryouNo ratings yet
- The Art of Training (Your Animal) - Steve MartinDocument6 pagesThe Art of Training (Your Animal) - Steve MartinBlackDawnNo ratings yet
- Papers Framework of Question Tag.Document15 pagesPapers Framework of Question Tag.YoonaNo ratings yet
- Software Engineer Cover LetterDocument3 pagesSoftware Engineer Cover Letternur syahkinaNo ratings yet
- Understanding Human DevelopmentDocument20 pagesUnderstanding Human Developmentwayne amparos100% (4)
- (The Basic Principles of TEFL - TESOL) Task 1Document30 pages(The Basic Principles of TEFL - TESOL) Task 1Asya Sevil YoldasNo ratings yet
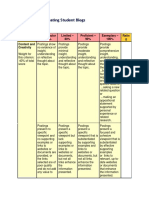
- A Rubric For Evaluating Student BlogsDocument5 pagesA Rubric For Evaluating Student Blogsmichelle garbinNo ratings yet
- Annotated BibliographyDocument5 pagesAnnotated BibliographyBrian MaingiNo ratings yet
- Efforts and Difficulties in Teaching Vocabulary: N. V. F. Liando, J. D. Adam, T. K. LondaDocument5 pagesEfforts and Difficulties in Teaching Vocabulary: N. V. F. Liando, J. D. Adam, T. K. LondaChery BlossomNo ratings yet
- OCC324 Reading ListDocument4 pagesOCC324 Reading ListMUNIRA ALTHUKAIRNo ratings yet
- A Critique Paper On The Discourse of Print Advertising in The PhilippinesDocument6 pagesA Critique Paper On The Discourse of Print Advertising in The PhilippinesEunice ResurrecionNo ratings yet
- LP 2 - Mask MakingDocument2 pagesLP 2 - Mask Makingapi-302077404No ratings yet
- The Brown Bauhaus STUDIO ARCHITECTURE: Fundamental Course - Comprehensive Ale Review + Preparation ProgramDocument10 pagesThe Brown Bauhaus STUDIO ARCHITECTURE: Fundamental Course - Comprehensive Ale Review + Preparation ProgramClaro III TabuzoNo ratings yet
- 1-Didactics vs. Pedagogy - Part 1Document14 pages1-Didactics vs. Pedagogy - Part 1ghadaNo ratings yet
- CS UG MPE 221 Flid Mech DR Mefreh 1Document5 pagesCS UG MPE 221 Flid Mech DR Mefreh 1Mohamed AzeamNo ratings yet
- Human VaulesDocument48 pagesHuman VaulesEstablishment GECBharatpurNo ratings yet
- Student Teacher Performance Everett Pickleball 1Document2 pagesStudent Teacher Performance Everett Pickleball 1api-302193708No ratings yet
- Effects of Procrastination on Student Academic PerformanceDocument16 pagesEffects of Procrastination on Student Academic PerformancealyaNo ratings yet
- Mathematics-guide-for-use-from-September-2020 January-2021Document63 pagesMathematics-guide-for-use-from-September-2020 January-2021krisnaNo ratings yet
- Notre Dame of Masiag, Inc.: Unit Learning PlanDocument3 pagesNotre Dame of Masiag, Inc.: Unit Learning PlanGjc ObuyesNo ratings yet
- CMIP 6103 Ion System Planning-HighlightedDocument231 pagesCMIP 6103 Ion System Planning-HighlightedCastro SamNo ratings yet
- Test Bank For Social Psychology 5th Edition Tom GilovichDocument13 pagesTest Bank For Social Psychology 5th Edition Tom GilovichDevin MckayNo ratings yet
- Barreno, Marou P.: Performance Task 1Document3 pagesBarreno, Marou P.: Performance Task 1mars100% (2)
- Pengembangan Modul Ipa Berbasis Kearifan Lokal Kopi Pada Pokok Bahasan Usaha Dan Energi Di SMPDocument8 pagesPengembangan Modul Ipa Berbasis Kearifan Lokal Kopi Pada Pokok Bahasan Usaha Dan Energi Di SMPAnonymous xXllbGQNo ratings yet