You might also like
- Handbook of Vitamin D in Human Health - Prevention, Treatment and ToxicityDocument715 pagesHandbook of Vitamin D in Human Health - Prevention, Treatment and ToxicityElvis Florentino100% (3)
- ExcelDocument1 pageExcelJosh KempNo ratings yet
- Kenwood - FP698 - User ManualDocument8 pagesKenwood - FP698 - User ManualianjprNo ratings yet
- Pif 5 0Document48 pagesPif 5 0patricioacurioNo ratings yet
- MM Module 1 A Prelude To The World of MarketingDocument11 pagesMM Module 1 A Prelude To The World of MarketingAbhishek MukherjeeNo ratings yet
- Vitamin D Fact Sheet FINAL ENDocument8 pagesVitamin D Fact Sheet FINAL ENJu RiNo ratings yet
- Vitamin D and The Skin: An Update For Dermatologists: Key PointsDocument13 pagesVitamin D and The Skin: An Update For Dermatologists: Key PointsBogdan HateganNo ratings yet
- Vitamin D in DermatologyDocument4 pagesVitamin D in DermatologyErnawati HidayatNo ratings yet
- Vit D in DADocument13 pagesVit D in DAVandalita KwNo ratings yet
- Skin Cancer Prevention and UV-protection: How To Avoid Vitamin D-Deficiency?Document7 pagesSkin Cancer Prevention and UV-protection: How To Avoid Vitamin D-Deficiency?uisda astonyNo ratings yet
- D Light Vitamin D and Good HealthDocument6 pagesD Light Vitamin D and Good HealthEde GedeonNo ratings yet
- Vitamin D: Modulator of The Immune SystemDocument15 pagesVitamin D: Modulator of The Immune SystemJosé Antonio Silva NetoNo ratings yet
- 15 Vitamin DDocument17 pages15 Vitamin DAsma SaleemNo ratings yet
- Clinical & Experimental Allergy: Vitamin D and Its Role in Allergic DiseaseDocument10 pagesClinical & Experimental Allergy: Vitamin D and Its Role in Allergic DiseaseMichael HostiadiNo ratings yet
- FOTOPROTECCION Y VITAMINA D Kannan2014Document9 pagesFOTOPROTECCION Y VITAMINA D Kannan2014Anthony GarciaNo ratings yet
- Voulgaris2017 Article VitaminDAndAspectsOfFemaleFertDocument17 pagesVoulgaris2017 Article VitaminDAndAspectsOfFemaleFertLinnette AnaniasNo ratings yet
- 1 Jurnal Vit DDocument11 pages1 Jurnal Vit DDelvia AuroraNo ratings yet
- Vitamin D and Aspects of Female Fertility: ReviewDocument17 pagesVitamin D and Aspects of Female Fertility: ReviewOumaima Ben MerrakchiNo ratings yet
- Optimisation of Vitamin D Status For Enhanced Immuno Protection Against Covid 19 Mccartney and Byrne 2020 Final Imj Submission 200320Document6 pagesOptimisation of Vitamin D Status For Enhanced Immuno Protection Against Covid 19 Mccartney and Byrne 2020 Final Imj Submission 200320dytdenizkarpuzogluNo ratings yet
- Biology of Vitamin DDocument8 pagesBiology of Vitamin DEde GedeonNo ratings yet
- Prevention of Rickets and Vitamin D Deficiency in Infants, Children, and AdolescentsDocument13 pagesPrevention of Rickets and Vitamin D Deficiency in Infants, Children, and AdolescentsChristianHendrikusSoronganNo ratings yet
- Vitamin D - Values For Normal Are Exaggerated March 2011Document4 pagesVitamin D - Values For Normal Are Exaggerated March 2011JamesMyersNo ratings yet
- Use of Vitamin D in Clinical Practice: Review ArticleDocument15 pagesUse of Vitamin D in Clinical Practice: Review ArticleBimantoro SaputroNo ratings yet
- Prevention of Rickets and Vitamin D Deficiency in Infants, Children, and AdolescentsDocument11 pagesPrevention of Rickets and Vitamin D Deficiency in Infants, Children, and AdolescentsWill TohallinoNo ratings yet
- The Role of Vitamin D in The Immunopathogenesis of Allergic Skin DiseasesDocument6 pagesThe Role of Vitamin D in The Immunopathogenesis of Allergic Skin DiseasesAndre FerdianNo ratings yet
- Vitamin D Guide MinDocument16 pagesVitamin D Guide Minps piasNo ratings yet
- Vitamin D and Human Health: Molecular SciencesDocument6 pagesVitamin D and Human Health: Molecular SciencesRuth WibowoNo ratings yet
- Vitamin D: What You Need To KnowDocument8 pagesVitamin D: What You Need To KnowSatendra ThakurNo ratings yet
- Use of Vitamin D in Clinical Practice: Review ArticleDocument15 pagesUse of Vitamin D in Clinical Practice: Review ArticleWill TohallinoNo ratings yet
- A Pilot Study Assessing The Effect of Prolonged Administration of High Daily Doses of Vitamin D On The Clinical Course of Vitiligo and PsoriasisDocument14 pagesA Pilot Study Assessing The Effect of Prolonged Administration of High Daily Doses of Vitamin D On The Clinical Course of Vitiligo and PsoriasisMario CoelhoNo ratings yet
- Vitamin D Deficiency in Childhood Old Lessons and Current Challenges 2018Document14 pagesVitamin D Deficiency in Childhood Old Lessons and Current Challenges 2018Arturo RNo ratings yet
- The Role of Vitamin D in Enhancing Immunity and Its RecommendationsDocument4 pagesThe Role of Vitamin D in Enhancing Immunity and Its RecommendationsWarstek TVNo ratings yet
- Vitamina DDocument4 pagesVitamina DAnonymous BWVVQpxNo ratings yet
- Lesson 8 - Vitamin D and Health - The Missing Vitamin in Humans - pp.1-3Document3 pagesLesson 8 - Vitamin D and Health - The Missing Vitamin in Humans - pp.1-3Cláudia FranzãoNo ratings yet
- Vitamin D in Health and Disease A Literature Review. Basit SDocument4 pagesVitamin D in Health and Disease A Literature Review. Basit SaflspyogfNo ratings yet
- Wolpowitz Vitamin D PDFDocument17 pagesWolpowitz Vitamin D PDFdr.herusetiawanNo ratings yet
- Biochem ProjectDocument10 pagesBiochem ProjectDana AhmadNo ratings yet
- Vitamin D and Multiple Sclerosis A ComprehensiveDocument27 pagesVitamin D and Multiple Sclerosis A ComprehensiveEugenia KoumakiNo ratings yet
- Relation of Vitamin D and Immunity With Reference To Unani System of Medicine - A ReviewDocument5 pagesRelation of Vitamin D and Immunity With Reference To Unani System of Medicine - A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Vitamin D and Ocular InflammationDocument5 pagesVitamin D and Ocular InflammationRIYA PARVEENNo ratings yet
- Vitamin D in Health and Disease A Literature Review PDFDocument8 pagesVitamin D in Health and Disease A Literature Review PDFafdtxmwjsNo ratings yet
- Vitamin D Literature ReviewDocument8 pagesVitamin D Literature Reviewea7gpeqm100% (1)
- Vitamin DDocument9 pagesVitamin DREINONo ratings yet
- 4612 4621 Vitamin D Supplementation For Osteoporosis in Older AdultsDocument10 pages4612 4621 Vitamin D Supplementation For Osteoporosis in Older AdultsMohammedNo ratings yet
- Cancer, Sunlight and Vitamin DDocument8 pagesCancer, Sunlight and Vitamin DDavid Rafael RamírezNo ratings yet
- Nutrients: Vitamin D and Age-Related Macular DegenerationDocument15 pagesNutrients: Vitamin D and Age-Related Macular DegenerationPatih GajahmadaNo ratings yet
- Vitamin D in Health and Disease A Literature ReviewDocument7 pagesVitamin D in Health and Disease A Literature Reviewfihum1hadej2100% (1)
- Vitamin D and Dementia PDFDocument9 pagesVitamin D and Dementia PDFRocco LamponeNo ratings yet
- Funadmental Questions and Inquiries To Sun ExposesDocument10 pagesFunadmental Questions and Inquiries To Sun ExposesRafi BouhamoudaNo ratings yet
- Vitamina D e TuberculoseDocument5 pagesVitamina D e TuberculoseIngrid MillanNo ratings yet
- Vitamin D Deficiency Research PaperDocument6 pagesVitamin D Deficiency Research Papergw0935a9100% (1)
- Vitamin D Is Not As Toxic As Was Once Thought: A Historical and An Up-to-Date PerspectiveDocument4 pagesVitamin D Is Not As Toxic As Was Once Thought: A Historical and An Up-to-Date Perspectivehosam alosNo ratings yet
- Vitamin D Resistance As A Possible Cause of Autoimmune Diseases: A Hypothesis Con Firmed by A Therapeutic High-Dose Vitamin D ProtocolDocument11 pagesVitamin D Resistance As A Possible Cause of Autoimmune Diseases: A Hypothesis Con Firmed by A Therapeutic High-Dose Vitamin D Protocoldr belaidi nadirNo ratings yet
- Vitamin D's Effect On Immune Function: ReviewDocument21 pagesVitamin D's Effect On Immune Function: ReviewColo VoltaNo ratings yet
- Baking Update Special Edition March 2011 Vitamin D The RevolutionDocument2 pagesBaking Update Special Edition March 2011 Vitamin D The RevolutionJavier GuerreroNo ratings yet
- Analysis of Association of Vitamin D3, Hemoglobin and Ferritin With Special Respect To Libyan PatientsDocument5 pagesAnalysis of Association of Vitamin D3, Hemoglobin and Ferritin With Special Respect To Libyan PatientsMediterr J Pharm Pharm SciNo ratings yet
- Mercola Vitamin D in The Prevention of Covid-19 FullDocument46 pagesMercola Vitamin D in The Prevention of Covid-19 Fullcalell01No ratings yet
- Low Serum Vitamin D Levels in Type 2 Diabetes Patients Are Associated With Decreased Mycobacterial ActivityDocument9 pagesLow Serum Vitamin D Levels in Type 2 Diabetes Patients Are Associated With Decreased Mycobacterial ActivityLina SilvaNo ratings yet
- Autism, Vitamin D and Early Brain DevelopmentDocument3 pagesAutism, Vitamin D and Early Brain Developmentnizma safarinaNo ratings yet
- TMP 8673Document50 pagesTMP 8673FrontiersNo ratings yet
- Regulationofimmune Functionbyvitamindand ItsuseindiseasesofimmunityDocument34 pagesRegulationofimmune Functionbyvitamindand ItsuseindiseasesofimmunitypilarerasoNo ratings yet
- Sunshine and Vitamin D: A Comprehensive Guide to the Benefits of the "Sunshine Vitamin"From EverandSunshine and Vitamin D: A Comprehensive Guide to the Benefits of the "Sunshine Vitamin"No ratings yet
- 057 English Trial PMR 2010 Paper1Document16 pages057 English Trial PMR 2010 Paper1Gurichha KaurNo ratings yet
- Simple Present Tense and Simple Past TenseDocument7 pagesSimple Present Tense and Simple Past TenseResta MahesaNo ratings yet
- MicroPro Grill Recipes 2020Document85 pagesMicroPro Grill Recipes 2020Jayme-Lea VanderschootNo ratings yet
- Meghalaya State InformationDocument5 pagesMeghalaya State InformationCHAITANYA SIVA100% (1)
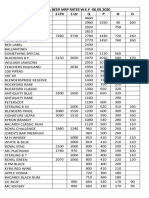
- Liquor & Beer MRP Rates Wef 17.12.2019 (1) - 1Document2 pagesLiquor & Beer MRP Rates Wef 17.12.2019 (1) - 1Kondu Krishna Vamsi ChowdaryNo ratings yet
- FST 362Document26 pagesFST 362गणेश सुधाकर राउत0% (1)
- Croatia 5 KvarnerDocument37 pagesCroatia 5 KvarnermumikaNo ratings yet
- Our Food 1. Fill in The BlanksDocument5 pagesOur Food 1. Fill in The BlanksSatish BhadaniNo ratings yet
- Journal of Applied Horticulture VOL 8Document87 pagesJournal of Applied Horticulture VOL 8123fvcNo ratings yet
- Present Simple and Present ContinuousDocument23 pagesPresent Simple and Present ContinuousLidia Gil González0% (1)
- BFN MastitisDocument2 pagesBFN MastitisafraxyzNo ratings yet
- Roohafza 150420234337 Conversion Gate02 PDFDocument27 pagesRoohafza 150420234337 Conversion Gate02 PDFKhubaib ImtiazNo ratings yet
- DairyDocument12 pagesDairyHimanshu SoniNo ratings yet
- Fast Moving Consumer GoodsDocument1 pageFast Moving Consumer GoodsAshwini ChaudhariNo ratings yet
- Rules of Subject Verb Agreement Are All You NeedDocument8 pagesRules of Subject Verb Agreement Are All You Needalexandra jacobNo ratings yet
- Lab 2 Assignment: Cnidaria and Porifera BIOL 2P92 - 09 Romil Patel (5844196) TA: Fiona Tuesday, January 24, 2017Document8 pagesLab 2 Assignment: Cnidaria and Porifera BIOL 2P92 - 09 Romil Patel (5844196) TA: Fiona Tuesday, January 24, 2017RomilPatelNo ratings yet
- Final Copy With Page SetupDocument37 pagesFinal Copy With Page SetupPankajDhobleNo ratings yet
- Number: 77-725 Passing Score: 800 Time Limit: 120 MinDocument40 pagesNumber: 77-725 Passing Score: 800 Time Limit: 120 MinArnold KanyindaNo ratings yet
- Coco Leaf NutrientDocument3 pagesCoco Leaf NutrientLive LikeNo ratings yet
- Blue-Tongued Skinks Care Sheet (PDF 472KB)Document4 pagesBlue-Tongued Skinks Care Sheet (PDF 472KB)Prosperline ReptileNo ratings yet
- Atg Worksheet PastsimplespellDocument6 pagesAtg Worksheet Pastsimplespellgabriel sanchez mora100% (1)
- And The Lion Shall Lie Down With The Lamb: An LDS Member's View of VegetarianismDocument32 pagesAnd The Lion Shall Lie Down With The Lamb: An LDS Member's View of VegetarianismKevin PomeroyNo ratings yet
- 2ND Summative Test in Tle 10Document3 pages2ND Summative Test in Tle 10FeGenGelsanoSarong100% (1)
- Saturday, 07 January 2023Document4 pagesSaturday, 07 January 2023Ankit padiyarNo ratings yet
- World07 08 15Document31 pagesWorld07 08 15The WorldNo ratings yet
- Coffee Recipes - Hot and Cold Coffee and Espresso Beverages To Make at HomeDocument66 pagesCoffee Recipes - Hot and Cold Coffee and Espresso Beverages To Make at HomeGiancarlo Braccio100% (2)