You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Drinking Water Contaminants in PakistanDocument4 pagesDrinking Water Contaminants in PakistanSardar Taimur Hyat-KhanNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Annoted Bibliography ObesityDocument8 pagesAnnoted Bibliography Obesityapi-451532782No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Khaled Hasan Resume 20180729Document6 pagesKhaled Hasan Resume 20180729api-312404919No ratings yet
- NursingCarePlan ELEAZAR G2BG4Document3 pagesNursingCarePlan ELEAZAR G2BG4John Cedryck Jhoshua ELEAZARNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Curriculum Vitae (CV) Abdul Malik SetiawanDocument4 pagesCurriculum Vitae (CV) Abdul Malik SetiawanAbdul MalikNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Instructions For The COVID-19 Vaccination - ModernaDocument2 pagesInstructions For The COVID-19 Vaccination - ModernaMarc LiNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 28 April - 1 MEI 2021: Enhancing Patient's Experience in Urogynecology ServicesDocument10 pages28 April - 1 MEI 2021: Enhancing Patient's Experience in Urogynecology ServicesUNS KAMERA BELAKANGNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- One Health: SciencedirectDocument11 pagesOne Health: SciencedirectIsabella GriffithNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
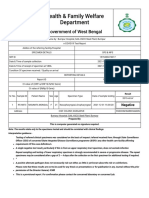
- RT PCR Test ReportDocument2 pagesRT PCR Test ReportMoumita MandalNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Cancer PDFDocument313 pagesCancer PDFAmanda TrebianoNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Visual CommunicationDocument20 pagesVisual CommunicationShiela FranciscoNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Sexual Education Multimedia PamphletDocument19 pagesSexual Education Multimedia Pamphletapi-565393622No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Rift Valley Fever: A Public Health Challenge Zoonotic DiseaseDocument25 pagesRift Valley Fever: A Public Health Challenge Zoonotic DiseaseTesfay HailuNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- NURSING RESEARCH-Questionnaire On Sexually Transmitted InfectionsDocument3 pagesNURSING RESEARCH-Questionnaire On Sexually Transmitted InfectionsEJ Cubero, R☤NNo ratings yet
- Gambaran Faktor Risiko Kejadian Abortus Spontan Pada Ibu Hamil Di Rsud Panembahan Senopati Bantul Tahun 2017-2018Document11 pagesGambaran Faktor Risiko Kejadian Abortus Spontan Pada Ibu Hamil Di Rsud Panembahan Senopati Bantul Tahun 2017-2018W Y OrizadewiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bala AwcDocument23 pagesBala AwcSamrat HazraNo ratings yet
- Get The Nutrition FactsDocument2 pagesGet The Nutrition FactsHayudini, Ashrina J.No ratings yet
- Truenat MTB Leaflet 2Document2 pagesTruenat MTB Leaflet 2yousra zeidanNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Embarazo Ectopico Tubarico ACOG 2018Document13 pagesEmbarazo Ectopico Tubarico ACOG 2018Jesus SuarezNo ratings yet
- Community Nursing Diagnosis and PrioritizingDocument12 pagesCommunity Nursing Diagnosis and Prioritizingsanty27No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Micro Teaching On: Placenta PreviaDocument10 pagesMicro Teaching On: Placenta Previasuchismita pandaNo ratings yet
- DRUGS IN PREGNANCY - A Handbook For Pharmacist and Physician 2021 PDFDocument465 pagesDRUGS IN PREGNANCY - A Handbook For Pharmacist and Physician 2021 PDFadelia100% (1)
- ECO GUARD Brochure (W) PDFDocument4 pagesECO GUARD Brochure (W) PDFSANTHWANAM MED CARENo ratings yet
- 6 Laboratory SafetyDocument17 pages6 Laboratory SafetyNipun ShamikaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- HB - SPARECHIT - SPARECHITCertif 27664632Document4 pagesHB - SPARECHIT - SPARECHITCertif 27664632Adeel RazaNo ratings yet
- Hepatitis ADocument16 pagesHepatitis AIngrid Masson PintoNo ratings yet
- PSM SeminarDocument33 pagesPSM SeminarSamarth JainNo ratings yet
- DGN ExamDocument5 pagesDGN ExamMaiga Ayub HusseinNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- what will happen if you go outside with wet hair - Поиск в GoogleDocument1 pagewhat will happen if you go outside with wet hair - Поиск в GoogleGiorgi AkubardiaNo ratings yet
- Dug Study NCPDocument4 pagesDug Study NCPYamete KudasaiNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)