You might also like
- 1959 MRC Breathlessness ScaleDocument1 page1959 MRC Breathlessness ScaleJefferson BantawigNo ratings yet
- Drug Name Classificati On Mechanism of Action Indication Adverse Effects Contraindicati Ons Nursing Consideration CNS: Cerebral AssessmentDocument2 pagesDrug Name Classificati On Mechanism of Action Indication Adverse Effects Contraindicati Ons Nursing Consideration CNS: Cerebral AssessmentJefferson BantawigNo ratings yet
- Health Education PlanDocument4 pagesHealth Education PlanJefferson BantawigNo ratings yet
- Knowledge DeficientDocument2 pagesKnowledge DeficientJefferson BantawigNo ratings yet
- Diagnostic TestDocument10 pagesDiagnostic TestJefferson BantawigNo ratings yet
- Health Education PlanDocument4 pagesHealth Education PlanJefferson BantawigNo ratings yet
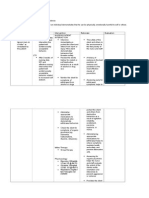
- NCPDocument3 pagesNCPJefferson BantawigNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Good Shepherd Hospital (Swaziland) TB Infection Control Policy Dec 2014Document30 pagesGood Shepherd Hospital (Swaziland) TB Infection Control Policy Dec 2014COMDIS-HSDNo ratings yet
- Hand Hygiene PPT 2020Document24 pagesHand Hygiene PPT 2020bevzie datuNo ratings yet
- Syphilis SeroDocument52 pagesSyphilis Seromarie judimor gomezNo ratings yet
- Morning SicknessDocument3 pagesMorning SicknessRhahadjeng Maristya PalupiNo ratings yet
- How To Describe Skin Rash PDFDocument72 pagesHow To Describe Skin Rash PDFGabrijela PejkićNo ratings yet
- Allergic Manifestation in Oral Cavity. Exudative Polymorphic Erythema. Chronic Recurrent Aphthous Stomatitis.Document38 pagesAllergic Manifestation in Oral Cavity. Exudative Polymorphic Erythema. Chronic Recurrent Aphthous Stomatitis.Alex DaniciNo ratings yet
- Maternal and Child NursingDocument11 pagesMaternal and Child NursingKSY JanedoeNo ratings yet
- ATLS Examination Questions and Answers 2019Document4 pagesATLS Examination Questions and Answers 2019Kamalan Push25% (8)
- Congenital Nasolacrimal Duct ObstructionDocument43 pagesCongenital Nasolacrimal Duct ObstructionAnumeha JindalNo ratings yet
- Immunization ChartDocument1 pageImmunization ChartDesilva ThampiNo ratings yet
- Veterinary Clinical Pathology Clerkship ProgramDocument46 pagesVeterinary Clinical Pathology Clerkship ProgramDrVijayata ChoudharyNo ratings yet
- Mcguckin 2004Document4 pagesMcguckin 2004noviaNo ratings yet
- Shock RosenDocument10 pagesShock RosenJuan GallegoNo ratings yet
- PMBLST of All ConditionsDocument18 pagesPMBLST of All ConditionsMitchell GowNo ratings yet
- Spot The Difference Skin Cancer FlyerDocument2 pagesSpot The Difference Skin Cancer FlyerAditi MorarkaNo ratings yet
- Care Plan Prep May 13 Rheumatic FeverDocument16 pagesCare Plan Prep May 13 Rheumatic Feverapi-256360167No ratings yet
- The RH Blood Group System: Tudy ID NswersDocument2 pagesThe RH Blood Group System: Tudy ID NswersChatie PipitNo ratings yet
- Mindmap Helminth TrematodaDocument1 pageMindmap Helminth TrematodaFadhila Permata SafitriNo ratings yet
- NCP 1Document2 pagesNCP 1Camille SesaldoNo ratings yet
- KNGF Guideline For Physical Therapy in Patients With ParkinsDocument89 pagesKNGF Guideline For Physical Therapy in Patients With ParkinsSrđan ŠarenacNo ratings yet
- Nasal Trauma Due To Continuous Positive Airway Pressure in NeonatesDocument5 pagesNasal Trauma Due To Continuous Positive Airway Pressure in NeonatesFabiano SilvaNo ratings yet
- A New Parameter For The Management of Positional Plagiocephaly: The Size of The Anterior Fontanelle MattersDocument9 pagesA New Parameter For The Management of Positional Plagiocephaly: The Size of The Anterior Fontanelle Mattersquajeutterugrau-6658No ratings yet
- Some Oncology Tips & Tricks by DR Khaled MagdyDocument8 pagesSome Oncology Tips & Tricks by DR Khaled MagdyA.h.Murad100% (1)
- Ascvd Risk Score 062719 KroDocument1 pageAscvd Risk Score 062719 KroQuang TranNo ratings yet
- Cornea and External DiseaseDocument26 pagesCornea and External Diseaserajeshwari saravananNo ratings yet
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Barret's & Tumors of Esophagus, SR, April 20Document52 pagesBarret's & Tumors of Esophagus, SR, April 20Tehreem NadeemNo ratings yet
- TATALAKSANA PROGNOSIS Cushing SyndromeDocument13 pagesTATALAKSANA PROGNOSIS Cushing SyndromeFirda RidhayantiNo ratings yet
- Tatalaksana Tekanan Tinggi Intrakranial Pada Anak-DikonversiDocument48 pagesTatalaksana Tekanan Tinggi Intrakranial Pada Anak-DikonversiAbdurrahman Arsyad As SiddiqiNo ratings yet
- Etiological Study of Autism and Assessment by ISAA (Indian Scale For Assessment of Autism) For Diagnosis of Autism Spectrum Disorder in Children at Hi Tech Medical College and Hospital, BhubaneswarDocument2 pagesEtiological Study of Autism and Assessment by ISAA (Indian Scale For Assessment of Autism) For Diagnosis of Autism Spectrum Disorder in Children at Hi Tech Medical College and Hospital, BhubaneswarMageeNo ratings yet